
Abstract
Pre-exposure prophylaxis (PrEP) with TDF/FTC significantly reduces the risk for HIV-1 transmission, but, to date, nobody knows if PrEP can still be useful in case of viruses harboring resistances to TDF/FTC or if alternative antiretroviral drugs might be rather proposed in selected cases. We promote the debate by describing a case of an acute infection with multiresistant HIV that occurred in a young girl who started a relationship with an HIV-infected partner who had a known multiresistant HIV.
F
Failures of standard PrEP have already been reported for patients acquiring a virus resistant to the drugs included in the regimen. 12 What is the best strategy to protect the sexual partner of a patient with detectable HIV-RNA and resistance mutations remains an open issue, when condom use is absent, occasional, or judged to be unlikely by the clinician.
We report, in this study, the case of a documented acute HIV-1 infection in a discordant couple in the presence of drug-resistant HIV. In June 2016, the couple presented to our Outpatient Service, reporting multiple unprotected sexual intercourses in the last weeks. The HIV-infected partner was a 27-year-old male with mother-to-child transmission and a history of poor adherence to care and medications over the last 5 years, which caused the development of a multiclass resistance, an issue that is not uncommon among perinatally infected adolescents. 13
His most recent HIV genotype, performed while the patient was not taking the antiretroviral therapy, revealed a wild-type HIV, but the historical sequences documented multiple resistance mutations: 41L, 62V, 70T, 103N, 184V, 215Y, 20T, 46I, 58E, 90M, and a X4-tropic virus. The detected mutations, according to the Stanford HIV Drug Resistance Database (HIVDB) algorithm, 14 confer high-level resistance to efavirenz (EFV), nevirapine (NPV), and all nucleoside reverse transcriptase inhibitors, excluding TDF, intermediate resistance to TDF and atazanavir, and low-level resistance to lopinavir. Among protease inhibitors, only darunavir (DRV) maintained full activity.
His current CD4 count was 20 cells/mmc and his HIV-RNA was 30,300 copies/mL. Despite the severe immunodeficiency, he was asymptomatic and he had recently started a new relationship with a seronegative 20-year-old female. At the first visit, she tested negative at a fourth generation HIV serology assay (HIV-RNA not performed). On that occasion, the couple was counseled about the risk for HIV transmission and condom use. The patient accepted to restart his last antiretroviral treatment with TDF/FTC/cobicistat (COBI)/elvitegravir (EVG), with whom he had previously (before the treatment discontinuation) reached HIV-RNA <50 copies/mL. His adherence was strongly encouraged. After one month, the female partner repeated the HIV serology, which was still negative. In August, however, after 2 months, her new test revealed the presence of the HIV p24 antigen, with HIV antibody negativity; the Western Blot was indeterminate, according to WHO criteria (reactivity limited to GAG p55 band); HIV-RNA was 190,000 copies/mL, confirming an acute infection in Fiebig stage II. CD4 count was of 400 cells/mmc (25.7%). The HIV genotype revealed the presence of 41L, 74I, 184V, 215Y, 98G, 103N, 179I, 181C and 58E mutations.
According to HIVDB algorithm, 14 these mutations confer high-level resistance to lamivudine, FTC, abacavir, EFV, NVP, and rilpivirine, intermediate-level resistance to AZT and etravirine, and low-level resistance to TDF. In the male partner, a new genotype test was done showing a virus identical to the partner's one and phylogenetic analysis established a pairwise distance of 0.000 between the two sequences (Fig. 1). Finally, the 92Q and 157Q mutations were also detected in integrase sequences obtained from both partners' samples. They confer intermediate- and high-level resistance to raltegravir and EVG, respectively, but they do not seem to compromise on DTG susceptibility (potential low-level resistance). The girl started DRV/COBI + DTG immediately after the diagnosis and obtained HIV-RNA <50 copies/mL at month 4. The event described is relevant for the implications of PrEP prescription in similar settings. Although PrEP is not yet available in Italy, this case highlights that we have limited options for PrEP in case of absent or inconsistent condom use within discordant couples, with detectable HIV-RNA and multidrug-resistant genotype. In fact, an appropriate PrEP regimen might have prevented a new HIV infection in a young girl, with a resistant virus, aggravated by the presence of integrase and protease gene mutations in a naive patient. However, which drug should have been prescribed with the hindsight? Should the regimen be chosen according to the historical resistance test? Should the genotypic resistance pattern in both serum and genital tract be considered, as a different genotypic profile is possible? Should the pharmacokinetic characteristics or drug distribution in the genital tract be taken into account in selecting alternative antivirals? Should the alternative PrEP regimen include one, two, or even more agents to be cautious in the absence of any evidence of its efficacy?
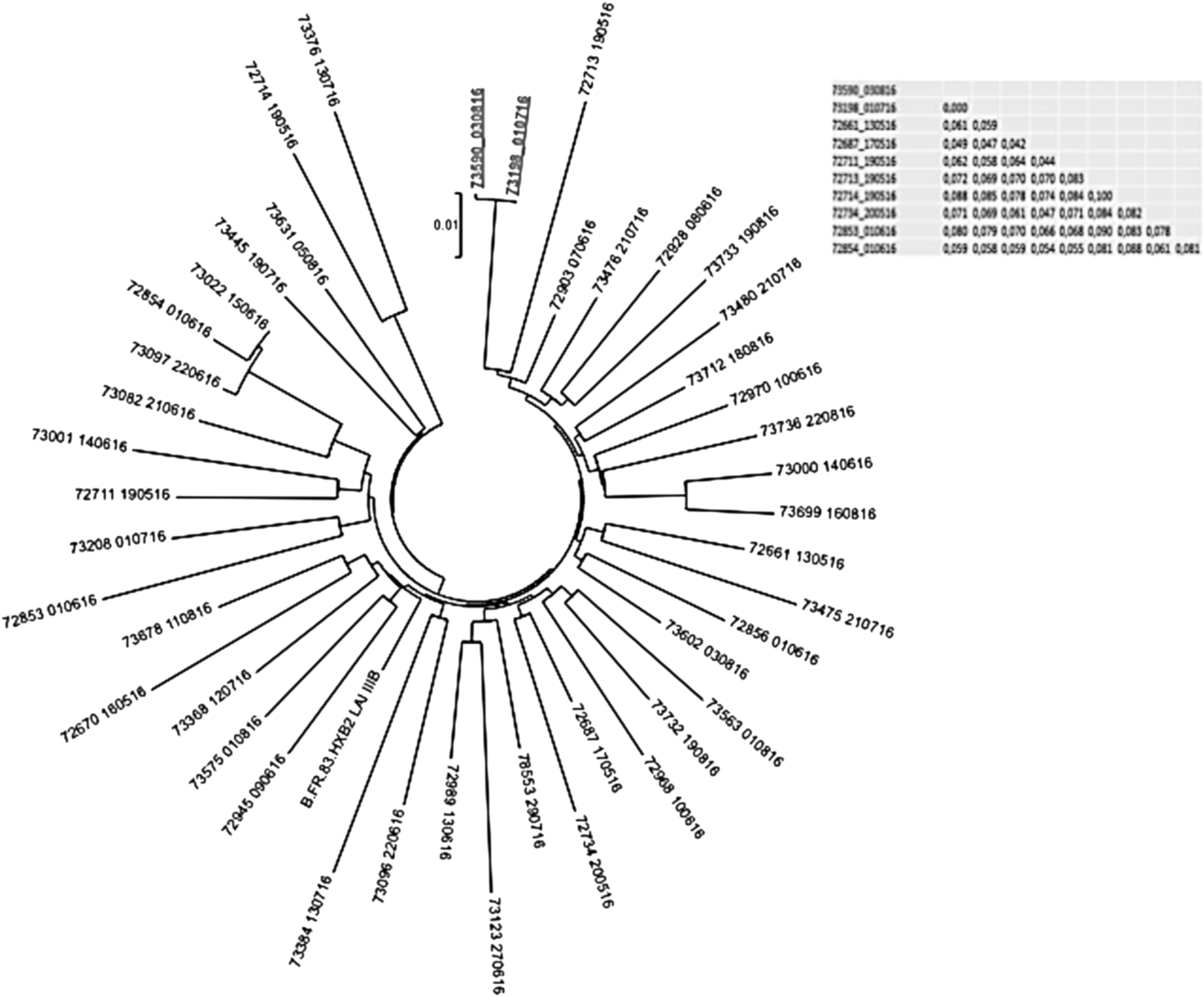
Phylogenetic tree was created with MEGA 5 by using HIV-1 subtype B pol sequences selected from the HIV-1 strains circulating in the same period in our region. Phylogenetic analysis showed identical HIV sequences in the two partners, indicated in bold and underlined in the figure. In the box are given the distances between all the sequences and, in the first line, the precise distance between the two partners (0.000).
While PrEP is slowly implementing in industrialized countries, new questions rapidly emerge for clinicians who call for the assistance of timely guidelines.
Footnotes
Disclosure Statement
No competing financial interests exist.