
Abstract

H
Several new direct-acting antivirals (DAAs) are available and successfully used in HCV treatment. All currently available DAAs are strictly correlated with genotype, thus, to avoid treatment failure, an accurate classification of HCV genotypes/subtypes is recommended by guidelines. 1 –3 However, although several methods are routinely available for HCV genotyping, not all viruses can be assigned to a genotype. Sequence analyses of the NS5B and/or of the core region represent the gold standard for HCV genotyping. Among available tests (real-time PCR, restriction fragment length polymorphism, heteroduplex mobility analyses, and line-probe assay), Abbott Real-Time HCV Genotype II (Abbott Molecular) and INNO-LiPA™ HCV II kit (LiPA; Innogenetics, Ghent, Belgium) are the most widely used commercial assays. Both tests target the 5′ untranslated region, but to better discriminate between genotype 1 subtypes, they also target the core region (LiPA) and the NS5B region (Abbott Real-Time HCV Genotype II). 1 –3
Two cases of dual HCV infection are briefly reported. Both have a history of intravenous drug abuse, are HIV-HCV coinfected, and on antiretroviral therapy with a satisfactory immunological profile and undetectable viral load from many years. For DAAs pretreatment screening, they underwent HCV genotyping. LiPA suggested the presence of dual infection (DI) in both patients, 1a+1b (Genoa_018) and 4 + 1a (Genoa_039), respectively (Fig. 1a). Phylogenetic analysis of a conserved fragment within the NS5B region (nucleotide 8281–8679), using a homemade protocol, identified only 1 subtype (4d and 1a, clade 1, respectively—Fig. 1b), whereas the complete NS3/4, NS5A, and NS5B sequences, using homemade protocols and subtype specific primers 3,4 (Fig. 1c) and the Sentosa® SQ Next-Generation Sequencing (NGS; Vela Diagnostics Germany GMBH, Hamburg, Germany) (Fig. 1d) allowed us to confirm the presence of DI.
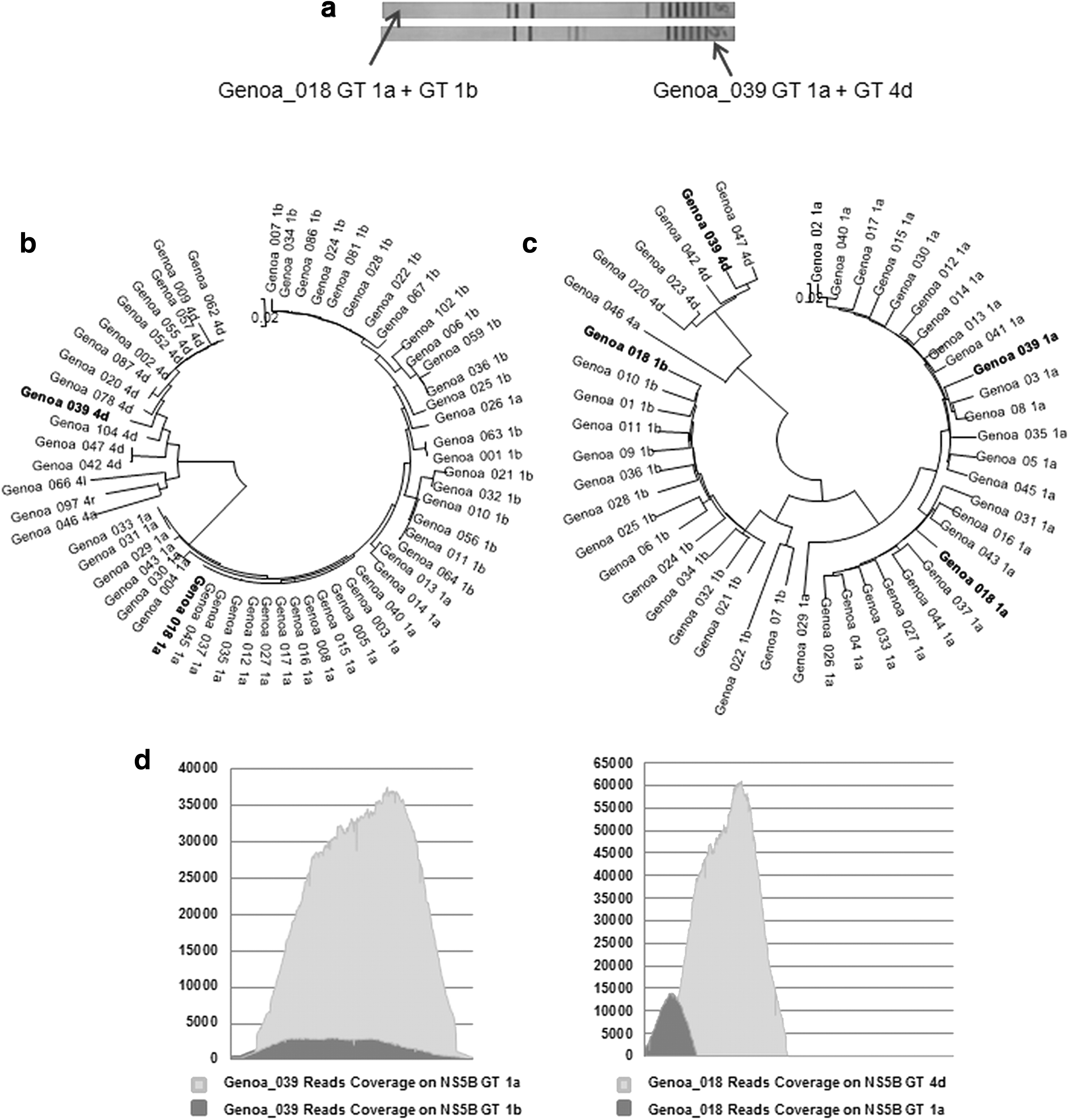
Methods used to confirm the presence of mixed infection in two patients with HCV infection:
These two cases raise an important question. LiPA has been reported to produce errors in about 10% of cases in terms of indeterminate results, wrong subtype, and/or genotype and have also limitations in identifying genotype 6. 1 –3 On the other hand, while it can be agreed that sequencing analyses of a specific region of HCV genome embodies the gold standard for HCV genotyping, 1 –3 it does not seem to represent a suitable method for routine diagnosis. NGS is a new technology that provides additional information especially on minority species prevalence, but can hardly fit routine settings. 1 Should then the aged, nevertheless, convenient and robust LiPA, without which these two DI could not have been identified, be always included in the routine pretreatment diagnostic algorithm of HCV infection, to help avoid preventable failures?
Footnotes
Acknowledgment
The authors thank the Chair of Virology of the University of Rome “Tor Vergata,” Italy for the transfer of the laboratory protocols and the assistance provided.
Author Disclosure Statement
No competing financial interests exist.