
Abstract
Maximizing the rates of virologic suppression (VS) among gay, bisexual, and other men who have sex with men (MSM) is essential to limiting HIV morbidity and sexual transmission of HIV in the United States. We analyzed data for MSM of non-Hispanic white (white), non-Hispanic black (black), or Hispanic/Latino race/ethnicity in the HIV Outpatient Study (HOPS) at nine U.S. HIV clinics. VS (HIV RNA <50 copies/ml) was measured closest to January 1, 2015. We modeled factors associated with VS among persons prescribed antiretroviral therapy (ART) for ≥6 months and assessed VS for a subset of participants with behavioral interview data. Among 1,303 MSM studied, 24% were black and 11% were Hispanic/Latino. Fewer black than white or Hispanic/Latino MSM had any documented ART use history (92% vs. 99% and 94%, respectively), and fewer had VS (72% vs. 91% and 81%), p < .001. In analyses of MSM prescribed ART, which adjusted for insurance type, duration of ART use, and CD4+ cell count, blacks had lower prevalence of VS than whites [adjusted prevalence ratio (PR) 0.87, confidence interval (95% CI) 0.81–0.93] and Hispanics/Latinos did not (PR 0.95, 95% CI 0.88–1.02). Among 331 MSM with interview data, 6% had no VS, but reported anal sex without a condom with an HIV-uninfected or unknown HIV serostatus male partner in the past 6 months. In this study of HIV-infected MSM, blacks had a significantly lower prevalence of VS than white men. Optimizing HIV care and prevention among all MSM will require addressing underlying risk factors and social determinants of health that contribute to racial/ethnic disparities in HIV outcomes.
Background
A
Materials and Methods
The HIV Outpatient Study
The HIV Outpatient Study (HOPS) is an ongoing prospective dynamic observational cohort study of HIV-infected adults receiving care at nine HIV clinics (university based, public, and private) in six U.S. cities (Chicago, IL; Denver, CO; Stony Brook, NY; Philadelphia, PA; Tampa, FL; and Washington, DC) since 1993. Patient data, including sociodemographic characteristics, symptoms, diagnoses, treatments, and laboratory values, are abstracted from medical charts and entered into an electronic database (Discovere©; Cerner Corporation, Kansas City, MO) by trained staff. These data are reviewed for quality and analyzed centrally. Through December 2015, the HOPS has collected information on more than 10,600 patients at over 490,000 clinical encounters.
HOPS participants are also offered participation in an optional brief telephone or web-based Audio-Computer Assisted Self-Interview (ACASI) survey that collects sociodemographic characteristics and risk behavior information. Participants are assigned unique 4-digit numbers, and asked to complete this confidential survey by dialing a 1–800 number or by accessing a website from a private location in the clinic or from home. The information collected includes age, sex at birth, use of alcohol and recreational drugs, cigarette smoking, adherence to ART, types of sexual intercourse, condom use, and disclosure of HIV serostatus to partners.
Since its inception, the HOPS protocol has been reviewed and approved annually by the Centers for Disease Control and Prevention (Atlanta, GA), Cerner Corporation (Kansas City, MO), and each local site's institutional review board. The study protocol conforms to the guidelines of the U.S. Department of Health and Human Services for the protection of human subjects in research. This analysis is based on HOPS data collected through December 31, 2015.
Study population
For the primary analyses, we included patients who had at least two HOPS visits since cohort inception in 1993, of which at least one occurred in 2014 or later, were MSM (defined as having had male-to-male sexual activity as a risk factor for HIV infection), and who had at least one HIV viral load (VL) result available from January 1, 2014–December 31, 2015 (index window) (see Fig. 1). We restricted analyses to MSM of self-reported white non-Hispanic/Latino (white), black non-Hispanic/Latino (black), or Hispanic/Latino race/ethnicity because of an insufficient number of individuals in other racial/ethnic categories for robust analyses. We selected the VL measurement closest to January 1, 2015, if there were multiple measurements available in the index window (termed “index VL”). For secondary analyses, we further limited the study population to MSM who completed ACASI within a year of the index VL test in 2014–2015, and who reported, through ACASI, having had sex with men during the previous 6 months. In this subset, we explored patterns of self-reported adherence to ART and sexual risk behavior by race/ethnicity.
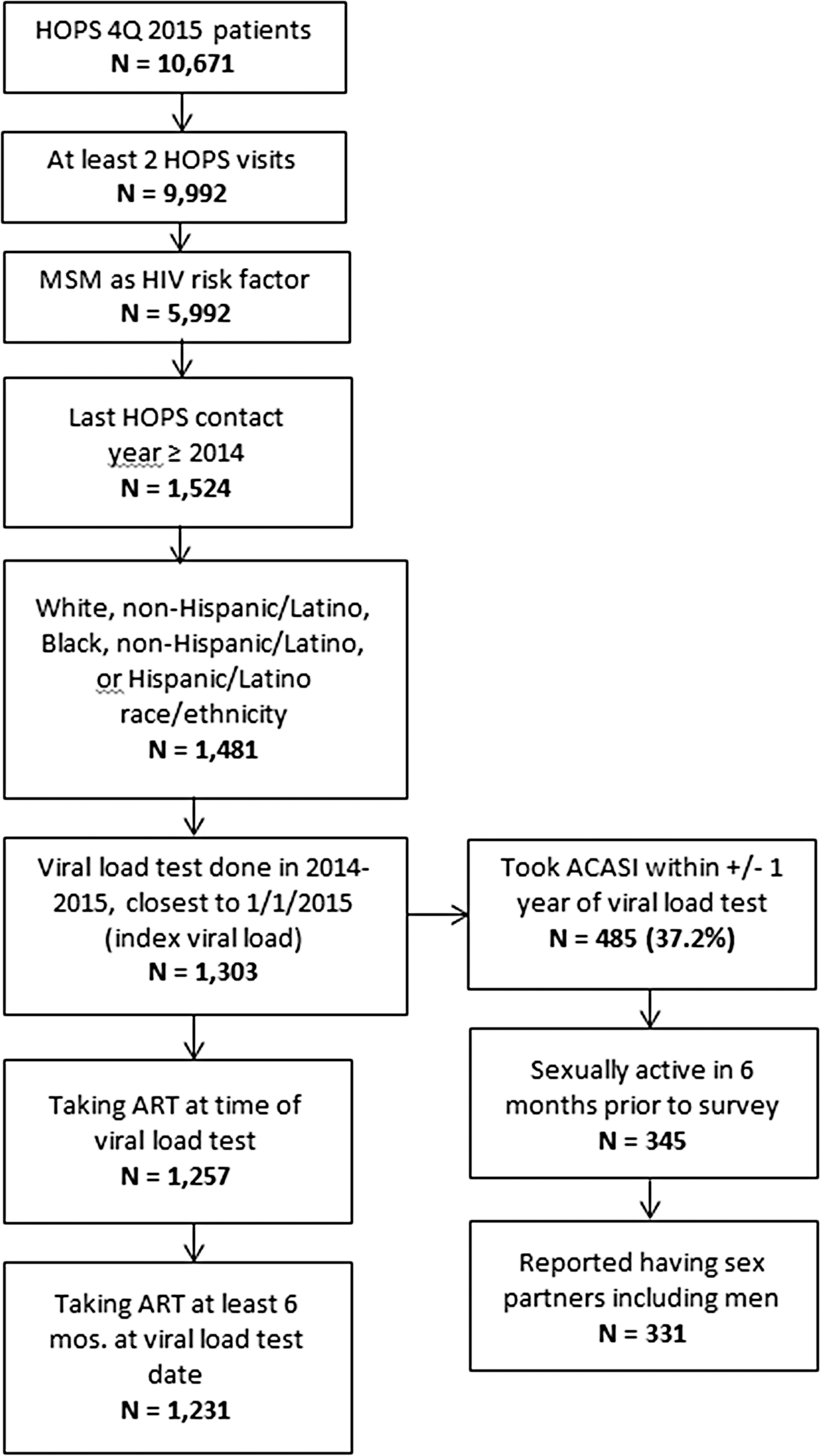
Selection of the study population and the subset of participants with ACASI survey data. ACASI, audio computer-assisted self interview; ART, antiretroviral therapy; MSM, men who have sex with men.
Measurements and definitions
The main outcome of interest was VS, defined as an index VL <50 copies/ml. We also assessed VS among men prescribed ART for at least 6 months, and further examined durable VS for these men, which was defined as having all available VL measurements <50 copies/ml (82.4% of men had >1 VL, but those with 1 VL were also evaluated) during the index window, per published method. 20 –22 In sensitivity analyses, we applied an alternate VS cutoff of <200 copies/ml to the index VL, as per DHHS ART treatment guidelines. 14 The demographic predictor variables included age in years at index VL date, race/ethnicity (black, white, or Hispanic/Latino), insurance (private, public, or none), year range of HIV diagnosis (<1996, 1996–2006, or 2007–2013), cumulative years of prior ART use, prior AIDS diagnosis, receipt of HIV care at a public clinic or otherwise, current/prior smoking status, nadir CD4+ cell count, and CD4+ cell count closest to and type of ART received at index VL [type of ART classified as integrase strand transfer inhibitor (INSTI) containing, protease inhibitor (PI) containing, or non-nucleoside reverse transcriptase inhibitor (NNRTI) containing].
For secondary analyses, conducted within the subset of patients who participated in the ACASI and reported male-to-male sexual activity, we assessed the frequency of engaging in anal sex when no condom (ASNC) with an HIV-uninfected or unknown HIV serostatus male partner during the 6 months before the survey. Additional collected variables included number of sex partners, recreational drug use [including cocaine, amyl nitrite (“poppers”), heroin, methamphetamine, “club drugs,” or erectile dysfunction drugs], alcohol binge drinking, report of any missed ART doses in the 3 days before taking the survey, and disclosure of HIV serostatus to all, some, or none of the sexual partners.
Statistical analyses
Descriptive summaries of the data, and univariate and multivariable logistic and linear regression model analyses were done using SAS version 9.4 (SAS Institute, Cary, NC). Likelihood ratio chi-square or Fisher's exact test was used to compare patient characteristics (binary or class variables) and Kruskal–Wallis or Wilcoxon rank-sum test were used to compare continuous variables by race/ethnicity. For the primary analyses, we used univariate and multivariable generalized linear modeling, assuming a binomial distribution, and a log link to investigate factors associated with VS among all MSM and among men prescribed ART for ≥6 months. We constructed the final multivariable model by including factors with p-value <.2 in the full multivariable model. For the secondary analyses, we descriptively assessed the frequency of VS among men who reported engaging in ASNC with an HIV-uninfected or an unknown HIV serostatus male partner(s) during the prior 6 months. Results with p < .05 were considered statistically significant.
Results
Characteristics of the study population
Among the 1,303 MSM studied, 856 (66%) were white, 308 (24%) were black, and 139 (11%) were Hispanic/Latino. Median age was 50 years, 35% were diagnosed with HIV infection before 1996, median duration of ART use was 10.1 years, and 55% had a documented AIDS diagnosis. Approximately 60% had private insurance, and the median CD4+ cell count was 607 cells/mm3. The majority of men (91%) were prescribed ART (at the time of VL measurement) and ∼40% were prescribed INSTI-containing ART. During the index window period of January 1, 2014, to December 31, 2015, the 1,303 men had a median of 5 [interquartile range (IQR) 3–10] visits to the HOPS clinic, and a median of 3 (IQR: 2–4) VL measurements recorded.
In univariate analyses, compared with white men, black and Hispanic/Latino MSM were significantly (p < .05) younger, more likely to have been diagnosed with HIV infection after 2006 and treated with ART for a shorter time, more likely to have been publicly insured, and more frequently cared for at public rather than private clinics (Table 1). Black MSM had lower current CD4+ cell counts, but similar nadir CD4+ cell counts compared with white and Hispanic MSM, and were less frequently prescribed ART at the time of index VL measurement. Among men prescribed ART, INSTI-containing regimens were less common among black (29%) and Hispanic/Latino (35%) MSM compared with white MSM (45%) (Table 1).
p-Values obtained using likelihood ratio chi-square test.
Public clinics sites are Stony Brook University, Temple University, and University of Illinois in Chicago; the remaining HOPS clinics were classified as private.
ART, antiretroviral therapy; HOPS, HIV Outpatient Study; IQR, interquartile range; MSM, men who have sex with men; NNRTI, non-nucleoside analog reverse transcriptase inhibitor; PI, protease inhibitor.
Frequency and correlates of VS, by race/ethnicity
Among all 1,303 men, 91.1% of white, 71.8% of black, and 80.6% of Hispanic/Latino MSM had VS (three-way p < .001, black vs. white p < .001, Hispanic/Latino vs. white p < .001, Hispanic/Latino vs. black p < .05). These VS disparities persisted when limiting analyses to 1,231 MSM who had been prescribed ART for ≥6 months (Fig. 2). Noted disparities in VS by race/ethnicity were apparent for younger men, for men seen in public and private clinics, and regardless of insurance type (Table 2). In the final multivariable model for 1,231 MSM prescribed ART for ≥6 months, which was adjusted for duration of ART use, insurance type, and CD4+ cell count (Table 3), blacks had lower prevalence of VS than whites [adjusted prevalence ratio (PR) 0.87, confidence interval (95% CI) 0.81–0.93], but Hispanics/Latinos did not have lower prevalence than whites (PR 0.95, 95% CI 0.88–1.02).

Percent of MSM by race/ethnicity with plasma viral load <50 copies/ml (viral suppression), 2014–2015 closest to January 1, 2015, the HIV Outpatient Study, USA, 2014–2015 (N = 1,303). VL, viral load.
p-Values obtained using likelihood ratio chi-square test or Fisher's exact test.
Public clinics sites are Stony Brook University, Temple University, and University of Illinois in Chicago; the remaining HOPS clinics were classified as private.
Full multivariable model determined by selecting factors with p-value <.2 in univariate models; except that type of insurance was excluded due to correlation with type of clinic care provider.
Final multivariable model determined by selecting factors with p-value <.2 in full multivariable model and including insurance status.
Regimen type describes regimen taken when viral load test was done.
aRR, adjusted relative risk; CI, confidence interval; RR, relative risk.
In supplementary analyses of data defining VS as <200 copies/ml, similar disparities as those depicted in Figure 2 were observed: the overall level of VS was 90.2% and it was 95.0% for white men, 79.2% for black men, and 84.9% for Hispanic/Latino men. The frequency of durable VS <50 copies/ml among men on ART for at least 6 months was somewhat lower for all men, but racial/ethnic differences persisted. The overall level of durable VS in this subset was 74.0%, and it was 75.7% for white men, 60.9% for black men, and 78.9% for Hispanic/Latino men.
VS and sex without condoms by race/ethnicity
Among the 1,303 MSM, 485 (37.2%) participated in an optional ACASI survey (293 completed by telephone and 38 completed online) within 1 year of index VL measurement (median time lag of 0.0 months, IQR: 6.0 months before VL to 0.9 months after VL); of these, 345 reported any sexual activity in the past 6 months, and 331 reported sexual activity involving male partners. The characteristics of these 331 MSM (Supplementary Table S1; Supplementary Data are available online at
Among the 331 MSM who had both VL data and ACASI data available, there were 194 (58.6%) who reported engaging in ASNC with an HIV-uninfected or unknown HIV serostatus male partner during the previous 6 months: this behavior was reported by 154 (62.3%) of white men, 22 (47.8%) of black men, and 18 (47.4%) of Hispanic/Latino men (three way p = .06) (Supplementary Table S2). There were few differences by race/ethnicity in reported drug use, and no differences in the percentage of men disclosing HIV serostatus to sexual partners. However, a significantly higher percentage of both black (21.7%) and Hispanic/Latino (23.7%) than white (8.9%) MSM reported missing an ART dose in the 3 days before completing the ACASI (p = .008).
Of the 194 (58.6%) men with both VL and ACASI data available, who reported engaging in ASNC with HIV-uninfected or unknown HIV serostatus partners, the vast majority also had index VL <50 copies/ml (Fig. 3). There were 21 MSM (6.3% of 311) who reported ASNC with an HIV-uninfected or unknown HIV serostatus male partner in the past 6 months with index VL ≥50 copies/ml (Fig. 3): this included 13 of 247 (5.3%) white men, 7 of 46 (15.2%) black men, and 1 of 38 (2.6%) Hispanic/Latino men (p = .024).
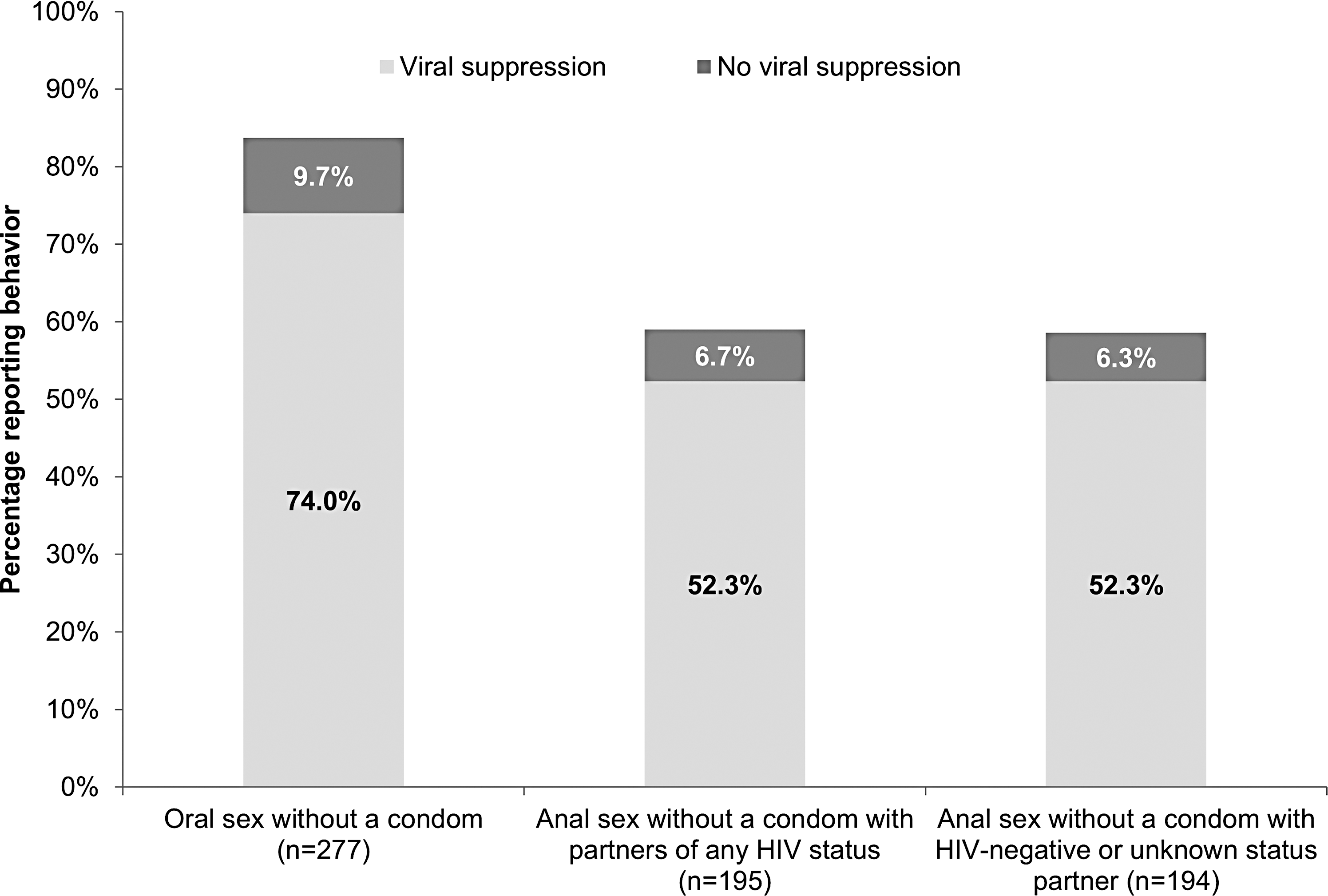
Prevalence of sex acts without a condom among sexually active MSM ACASI participants comparing men with viral suppression (<50 copies/ml) with men with no viral suppression (≥50 copies/ml), the HIV Outpatient Study, USA, 2014–2015 (N = 331).
Discussion
In our diverse U.S.-based population of patients in HIV care, black MSM had a lower prevalence of VS than white men after controlling for other variables, while Hispanic/Latino MSM did not significantly differ by VS from whites. Factors such as type of insurance and clinic site, as well as being prescribed INSTI-containing ART regimens, were not independently associated with VS among men receiving ART. In secondary analyses limited to men who completed an optional ACASI survey, self-reported medication adherence was lower among black and Hispanic/Latino men compared with white men, which might explain, in part, the observed ethnic/racial disparities in the frequency of VS. The racial/ethnic disparities we observed stem, in part, from structural, social, and behavioral risk factors—largely unmeasured in medical record databases like ours—that tend to disproportionally affect men of color in the U.S.
Interventions aimed at improving HIV care outcomes for all MSM may need to address underlying structural factors (e.g., poverty, housing status, potentially underinsurance, and access to state-of-art treatments), and social inequalities (e.g., homophobia, stigma, and racial/ethnic discrimination) that correlate with poorer adherence to HIV care and treatments. 6,8 –10,12
It is presently recognized that there is effectively no risk of sexual HIV transmission in MSM couples when the HIV-infected partner maintains VS with ART. 17,23,24 However, as we and others have shown, not all MSM are continuously in care, prescribed ART, and adherent to ART, and thus able to maintain VS. 5,6,11,12,25 At a minimum, consistently attending HIV care visits is a prerequisite to being prescribed and remaining on ART, but sociodemographic disparities in the HIV care continuum have been reported. 26,27 Notably, we found that nearly 60% of sexually active MSM reported ASNC with partners of unknown or HIV-negative serostatus in the previous 6 months, and a minority (6.3% of the total surveyed) reported this behavior when the proximal VL was ≥50 copies/ml. We do not have data as to whether any of these ASNC acts involved preexposure prophylaxis use among sexual partners. 28 Although the findings cannot be directly compared, our estimates are in line with earlier results from a national probability sample of HIV-infected patients in care in 2009, in which 6% of MSM reported vaginal or anal sex without a condom with an HIV-uninfected or unknown HIV serostatus partner in the prior 12 months and when not virally suppressed (i.e., had at least one VL >200 copies/ml). 22
Our study is subject to some further caveats and limitations. We analyzed data from nine HIV clinic sites (private practice and public/university based) using a convenience sample of HIV-infected patients in care. We relied on information abstracted from medical records of routine HIV care and a brief optional (median = 7 min) telephone/web-based ACASI survey, and did not collect information on psychosocial and economic factors that could explain potential differences in ART adherence and VS by race/ethnicity. For our secondary analyses, only 37% of men completed the ACASI survey within 1 year of VL measurement and contributed behavioral information (see Fig. 1). Nonetheless, ACASI was offered to HOPS participants on an annual basis, and MSM who completed ACASI were similar to all MSM studied (Table 1 vs. Supplementary Table S1). We relied on a VS definition based on a single VL measurement, which is subject to variability and imprecision 29 ; however, when we focused on durable VS (all VL in the year <50 copies/ml), the disparities by race/ethnicity continued to persist, consistent with earlier reports. 6,20 Furthermore, because sexual behavior data could have been collected up to 1 year from VL measurement, we cannot be certain of VS status at the time of ASNC. Finally, although HOPS is a convenience sample of patients seen at nine U.S. HIV clinics, our population is demographically diverse and similar clinically to HIV-infected persons in care across the nation. 21
In conclusion, black MSM prescribed ART for at least 6 months had ∼13% lower prevalence of viral suppression than white MSM, although there was no marked difference in VS between Hispanic/Latino and white MSM. Reasons for this black vs. white discrepancy are not altogether clear. However, based on research and programmatic findings, there appear to be a myriad of underlying factors (psychosocial, behavioral, and structural) that affect ability to achieve and maintain adherence to ART. Combined interventions are needed to support adherence to HIV care and treatment among black MSM to improve health outcomes overall and facilitate secondary prevention in this priority population.
Footnotes
Acknowledgments
For the HOPS: Centers for Disease Control and Prevention (contract nos. 200-2001-00133, 200-2006-18797, 200-2011-41872, and 200-2015-63931).
Disclaimer
The findings and conclusions in this report are those of the authors and do not necessarily represent the views of the Centers for Disease Control and Prevention.
Author Disclosure Statement
No competing financial interests exist.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.