
Abstract
Therapeutic vaccination has the potential to contribute to functional HIV cure strategies. However, to show functional HIV cure, study participants must be taken off combination antiretroviral therapy (cART). The availability of suitable biomarkers that can predict viral load (VL) or CD4 count outcomes following therapeutic HIV vaccination would reduce the risks associated with cART interruption in such studies. This report sought to determine baseline and postvaccination biomarker predictors of vaccine effect (VE) on VL and CD4 counts following cART interruption in a double-blind, randomized phase 2 study of the peptide-based therapeutic HIV vaccine, Vacc-4x (n = 93), versus placebo (n = 43). Antibody responses to a novel envelope glycoprotein antigen, C5/gp41732–744, and three safety marker measurements [C-reactive protein (CRP), white blood cell, and lactate dehydrogenase] were considered. Interaction tests in univariate and multivariate linear regression models were used to estimate the effect of biomarkers on VE, defined as the VL or CD4 count difference in Vacc-4x versus placebo groups. The reported q-values (considered significant for hypothesis-generating purposes if ≤0.2) accounted for multiple comparisons using the false discovery rate method. Data were analyzed from all available 58 Vacc-4x and 25 placebo recipients before cART resumption. Lower postvaccination fold-change over baseline of CRP concentration (interaction p- (q-) value = 0.005 (0.11) for VL) and higher fold-change of anti-C5/gp41732–744 antibody levels (0.005 (0.11) for VL and 0.009 (0.20) for CD4) were associated with Vacc-4x benefit. These findings suggest potential roles for inflammation and immune activation markers in predicting therapeutic HIV VE.
Introduction
W
Vacc-4x is a therapeutic HIV vaccine candidate consisting of four modified peptides corresponding to highly conserved cross-clade regions on the major capsid protein p24 of HIV-1. In a randomized, double-blind, placebo-controlled phase 2 clinical study enrolling 137 virologically suppressed HIV-infected participants who received Vacc-4x or placebo immunizations followed by analytical treatment interruption (ATI), Vacc-4x was shown to be safe and immunogenic. 5 In the primary vaccine efficacy analysis, Vacc-4x recipients showed a statistically significant reduction in VL set-point compared to placebo, although the study did not meet the prespecified coprimary endpoints in terms of rate of cART resumption and changes in CD4 counts during ATI. 5 In addition, independent follow-up exploratory analyses showed statistically significant reductions in VL and increase in CD4 counts, especially after accounting for preART VL or CD4 count values, in Vacc-4x versus placebo recipients during ATI. 7
Based on data collected in the phase 2 Vacc-4x trial, this report sought to assess baseline (prevaccination) and post-vaccination biomarker predictors of the previously reported vaccine effect (VE) of Vacc-4x to understand whether and how VE during ATI differ by various biomarker levels measured before ATI. Particular attention was paid to antibody responses to a novel envelope glycoprotein antigen (C5/gp41732–744) corresponding to the fifth constant region (C5) of gp120 and part of the transmembrane glycoprotein gp41. Antibodies to this region on the HIV-1 glycoprotein have previously been associated with slow disease progression and moderate VL in cART-naive individuals. 8
Slow disease progression and moderate VL are indicative of low generalized immune activation. It is therefore anticipated that under conditions of low generalized immune activation, immune responses will be less encumbered and can be more focused towards the therapeutic vaccine antigens provided. This in turn has the potential to improve vaccine efficacy. Prior exploratory analyses have also suggested potential differential associations between anti-C5/gp41732–744 antibody levels and VL set-point reduction (with or without reference to preART VL values) in Vacc-4x versus placebo recipients (Supplementary Tables S1 and S2; Supplementary Data are available online at
Materials and Methods
The Vacc-4x phase 2 clinical study
The Vacc-4x phase 2 clinical study (NCT00659789) took place from July 2008 to June 2010 in Spain, Italy, USA, the United Kingdom, and Germany. 5 Participants aged 18–55 years and virologically suppressed on cART were randomized to receive Vacc-4x or placebo immunizations at weeks 1–4 (priming), 16 and 18 (boosting). Eligible per-protocol (PP) participants (n = 126) were evaluated at week 24 for ATI eligibility (CD4 > 350 cells/mm3 and VL <50 copies/mL). cART interruption was timed such that all participants were off cART at week 28. Participants remained off cART for up to 24 weeks until week 52 (study end). cART was resumed if CD4 counts reached 350 cells/mm3 or dropped by ≥50% from baseline, after which participant monitoring continued. Participants with ATI until after week 40 were in the offARTwk40 subgroup (Vacc-4x n = 72; placebo n = 32) and participants with ATI until week 52 (6 months) were in the offARTwk52 subgroup (Vacc-4x n = 56; placebo n = 25) (Supplementary Tables S1 and S2).
C5/gp41732–744 antibody and clinical chemistry safety measurements
C5/gp41732–744 is a heterodimeric peptide comprising the C5 region of gp120 linked to a region of gp41732–744, to which the C5 region may interact at the cell surface. 10 Antibodies to this peptide have been associated with moderate VL and slow disease progression. 8 The concentration (μg/mL) of anti-C5/gp41732–744 antibodies in serum was measured using an ELISA assay 11 at weeks 1 (baseline), 6, 24, and 52. Clinical chemistry safety measurements, CRP (mg/L), LDH (units/L), and WBC (103/μL) levels, were determined by a central laboratory (Covance) using commercially available validated assays at weeks −4 (screening), 1, 4, 18, and 24 during cART and weeks 28, 32, 36, 40, 44, 48, and 52 during ATI.
Statistical analysis
All analysis approaches and variables were prespecified in the PP cohort before analysis. Univariate and multivariable linear regression models were used to estimate the effect of potential confounders, the effect of Vacc-4x versus Placebo, and their interactions with biomarkers at weeks 48 and 52 VL and CD4 count, or the fold-change over the preART VL and CD4 count. VE was estimated as the difference between the Vacc-4x and placebo groups in log10-transformed preART-adjusted (i.e., subtracted) and/or preART-unadjusted VL or CD4 count values. 7 All available demographics and clinical/laboratory antibody variables were considered, with particular focus on inflammation and immune activation markers. Specifically, 23 continuous factors were examined, including baseline variables: age, time on ART, time since HIV diagnosis, preART VL, PreART CD4, anti-C5/gp41732–744 antibody titer, LDH, CRP, and WBC measurements, as well as postbaseline variables: anti-C5/gp41732–744 antibody fold-change at weeks 24 and 52 relative to week 1 or to the previous measurement (week 24/week 1, week 52/week 1, and week 52/week 24), and safety measurements LDH, CRP, and WBC fold-change at weeks 18, 28, 32, and 40 relative to baseline (week 18/week 1, week 28/week 1, week 32/week 1, and week 40/week 1). In addition, 49 categorical factors were examined, including gender, country, HLA class I type, 7 and dichotomized variables of the above continuous factors.
Because biomarkers may be related to VE through a threshold model, meaning that the effect may be different depending on the biomarker values being above or below a certain value, two methods were used to dichotomize continuous variables: above or below the median value of the specific variable over the entire PP cohort, and above or below the splitting value of the specific variable that best segregate a given study endpoint over both treatment groups at the first node of regression tree analyses using the variable of interest as the sole predictor. 12 To account for multiple comparisons, the Benjamini and Hochberg method 13 was used to control the false discovery rate (FDR) for each endpoint within the raw categorical and continuous variables and derived dichotomized variables, separately. An FDR-adjusted p-value (or q value) ≤ 0.2 was considered significant evidence for hypothesis generation. 14
Results
Eighty-three PP participants (Vacc-4x:placebo = 58:25) were included in the analysis of the week 48 VL and CD4 count endpoints, and 81 (Vacc-4x:placebo = 56:25) for the analysis of week 52 VL and CD4 count endpoints (Fig. 1). Baseline anti-C5/gp41732–744 antibody and safety measurements were highly correlated with measurements taken at subsequent time points in both the Vacc-4x and placebo groups (Fig. 2). Fold-changes of each measurement between the subsequent time points and baseline were hence assessed as potential VE predictors because in this particular context, the use of fold-changes is generally a more powerful approach to account for baseline levels and their variability than adjusting for baseline levels as covariates in the regression model of biomarker levels at the subsequent time points. 4 Both the baseline values and fold-changes for the anti-C5/gp41732–744 antibody titer and safety measurements demonstrated a decent dynamic range of ± 4–6 standard deviations in the placebo and Vacc-4x groups (Supplementary Figs. S1–S6), supporting the subsequent regression model analyses. Among the 23 continuous and 49 categorical variables, 2 dichotomized variables of week 28/week 1 CRP and week 24/week 1 anti-C5/gp41732–744 antibody titer fold-changes were identified as predictors of VE on VL or CD4 count during ATI. 7
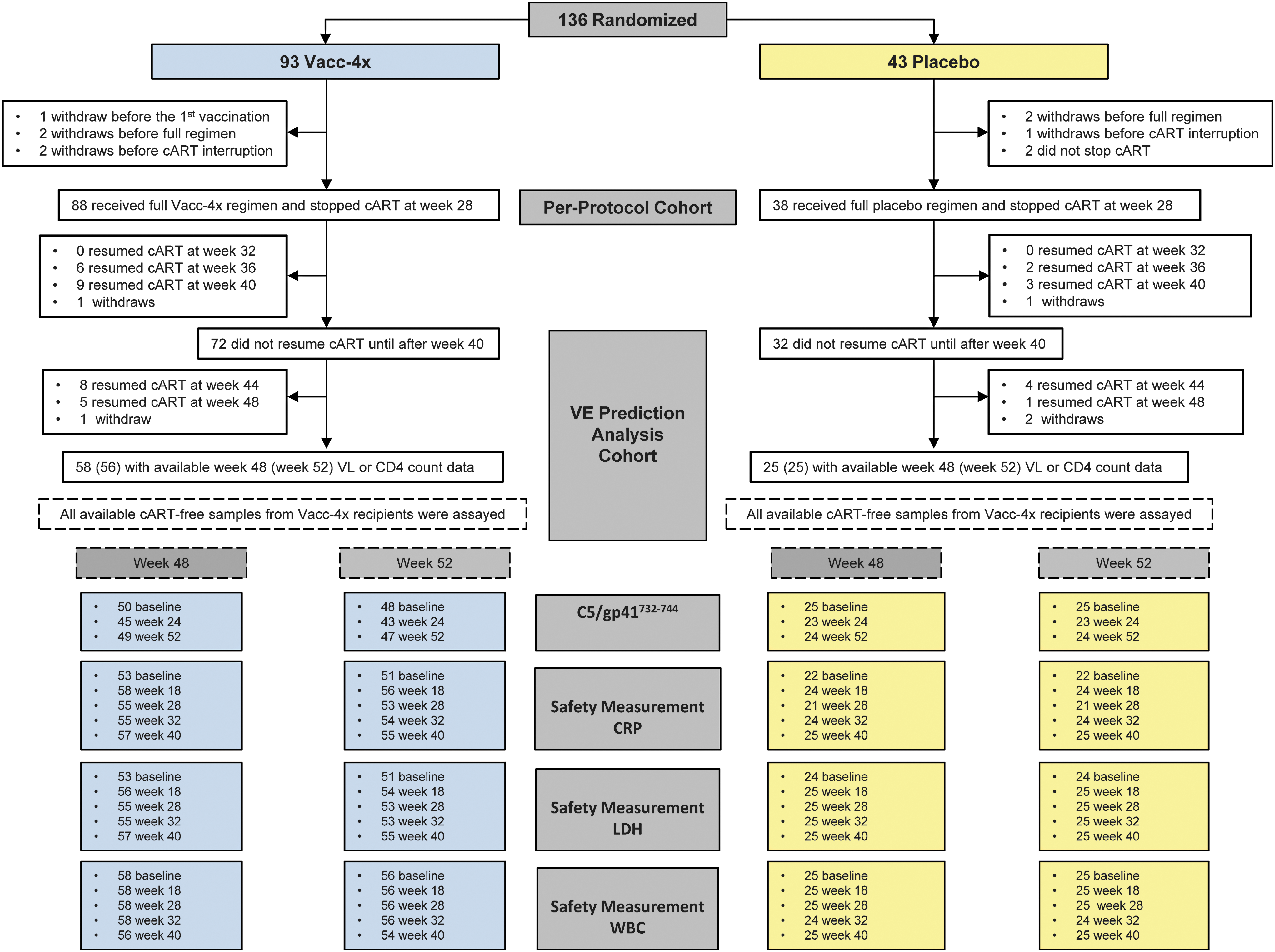
CONSORT diagram for the vaccine effect prediction analysis of the phase 2 Vacc-4x clinical study.
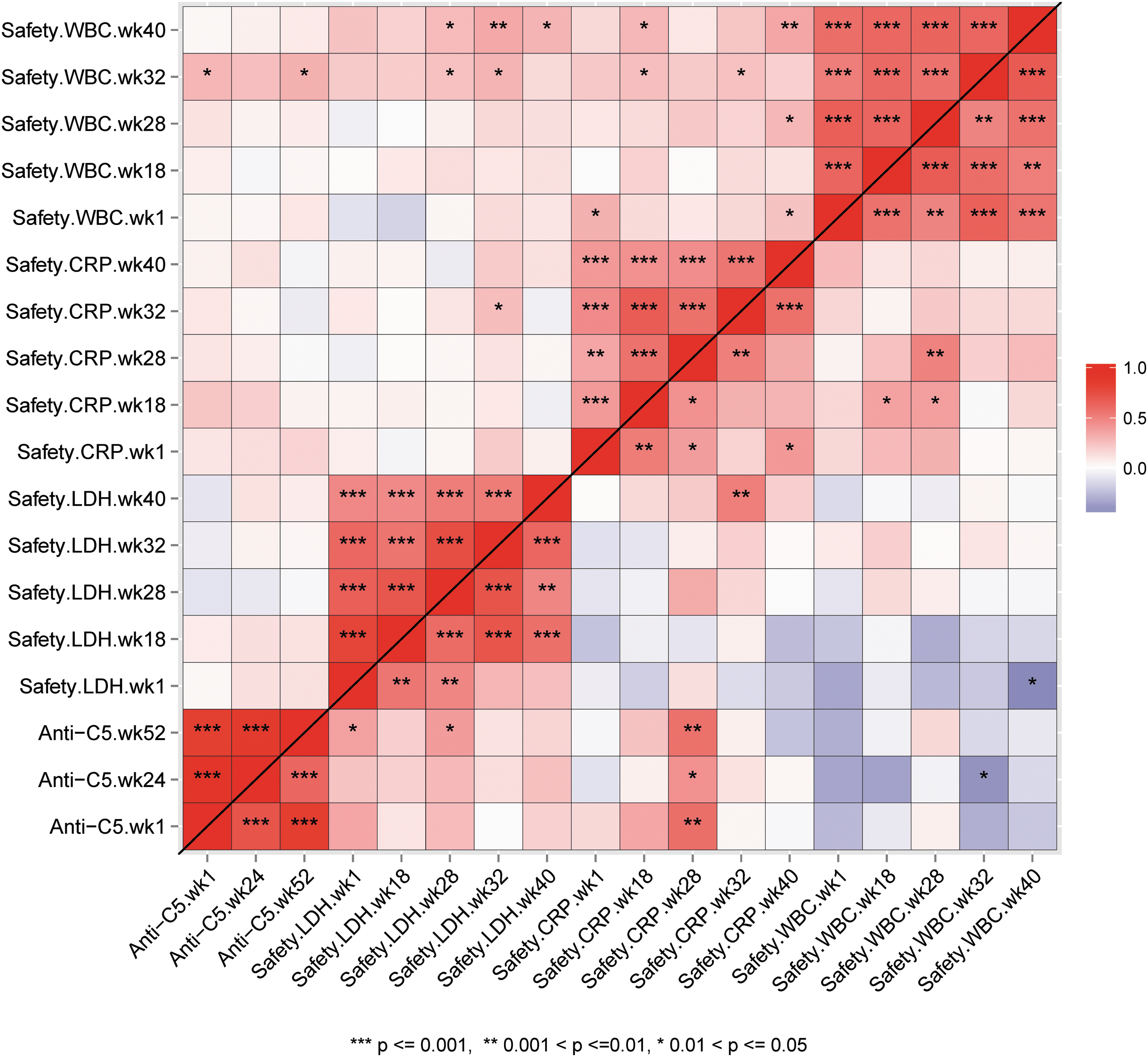
Correlations between anti-C5/gp41732–744 antibody levels measured at baseline, weeks 24 and 52, and safety measurements (LDH, CRP, and WBC) measured at baseline, weeks 18, 28, 32, and 40 in the Vacc-4x group (upper diagonal) and placebo group (lower diagonal). The direction and strength of Spearman correlation coefficients is presented in color grade, where dark red color indicates perfect positive correlation and dark blue color indicates perfect negative correlation. The significance of the correlation is reported as follows: *p < 0.05; **p < 0.01; and ***p < 0.001. CRP, C-reactive protein; WBC, white blood cell; LDH, lactate dehydrogenase.
First, we observed that lower CRP concentration fold-change at week 28/week 1 was significantly associated with Vacc-4x benefit in terms of controlling week 48 VL during ATI (interaction p = 0.005, adjusted q = 0.11) (Fig. 3A). Specifically, for study participants whose week 28/week 1 CRP fold-change was smaller than the median value 0.91, week 48 VL was 0.82 log10 copies/mL lower (95% CI: [−1.35 to −0.30]) in Vacc-4x recipients compared to placebo recipients, whereas no treatment difference in week 48 VL was observed among Vacc-4x and placebo participants with a higher CRP week 28/week 1 fold-change (Fig. 3A). Similar trends were observed for week 52 VL, although not statistically significant, possibly due to smaller sample sizes. This finding suggests that the previously reported effect of Vacc-4x in lowering VL compared to placebo at week 48 during ATI 5 is more pronounced in study participants with a lower CRP week 28/week 1 fold-change.
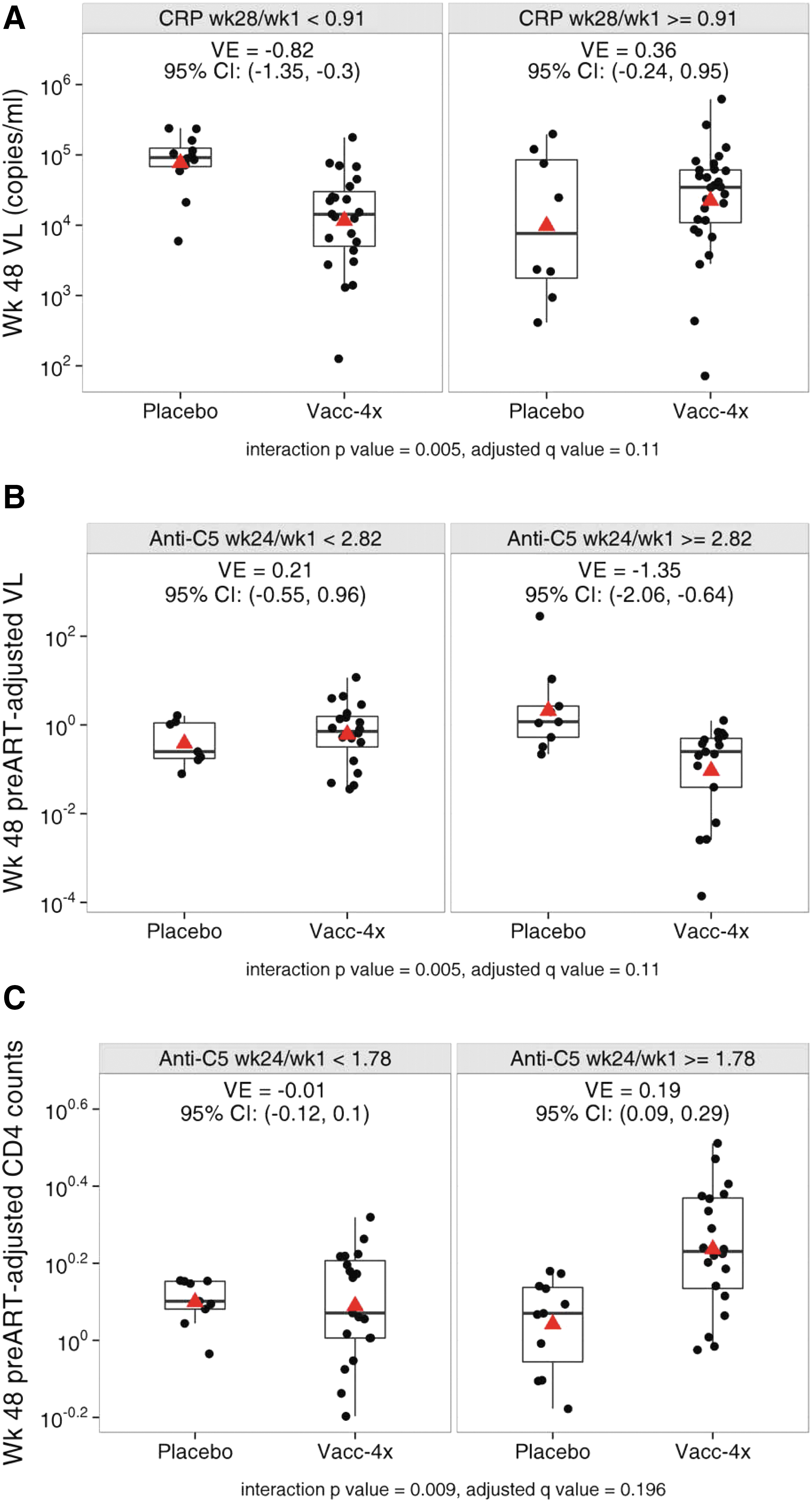
Observed and estimated mean endpoint by CRP and anti-C5/gp41732–744 antibody levels.
Second, we observed that higher anti-C5/gp41732–744 antibody titer fold-change at week 24/week 1 was associated with Vacc-4x benefit, in terms of both controlling VL (interaction p = 0.005, q = 0.11) and maintaining CD4 count during ATI (interaction p = 0.009, q = 0.20) (Fig. 3B, C). Specifically, for study participants whose week 24/week 1 anti-C5/gp41732–744 antibody titer fold-change was high (≥2.82), week 48 preART-adjusted VL was 1.35 log10 copies/mL lower (95% CI: [−2.06 to −0.64]) in Vacc-4x recipients compared to placebo recipients. On the other hand, for study participants whose week 24/week 1 anti-C5/gp41732–744 antibody titer fold-change was low (<2.82), week 48 preART-adjusted VL was not significantly different between the two treatment groups.
Furthermore, for study participants whose week 24/week 1 anti-C5/gp41732–744 antibody titer fold-change was high (≥1.78), week 48 preART-adjusted CD4 count was 0.19 log10 cells/L higher (95% CI: [0.09 to 0.29]) in Vacc-4x recipients compared to placebo recipients, while no difference in week 48 preART-adjusted VL was observed between treatment groups for study participants with lower week 24/week 1 anti-C5/gp41732–744 titer fold-change. Threshold values of 2.82 and 1.78 were identified in the regression tree analysis that best discriminated the week 48 preART-adjusted VL and week 48 preART-adjusted CD4 count, respectively, among vaccine and placebo recipients combined. Similar trends were also observed for week 52 preART-adjusted VL and CD4 count, although not statistically significant, possibly due to smaller sample sizes. These results suggest that the previously reported overall effect of Vacc-4x (vs. placebo) on preART-adjusted VL and CD4 count at week 48 was stronger for participants with a higher week 24 anti-C5/gp41732–744 antibody titer relative to their baseline values.
Discussion
The identification of appropriate biomarkers as potential surrogates for immune response-associated virus control and CD4 count maintenance would improve the safety of treatment interruption studies required in HIV clinical trials towards HIV cure/remission. This study generated important hypotheses for future evaluations of such surrogates. Although this study was only powered to discover predictors of large effect sizes given the study size, through a comprehensive analysis of 72 continuous and dichotomized variables based on safety and antibody biomarkers collected at baseline and postvaccination time points, we found that two fold-change predictors, anti-C5/gp41732–744 antibody and CRP levels, were significantly associated with Vacc-4x benefit in terms of controlling VL and maintaining CD4 count during ATI. To our knowledge, this is the first time these parameters have been systematically evaluated as potential biomarkers for therapeutic HIV VE.
Based on our findings, lower CRP concentration fold-change at week 28 relative to baseline was associated with a vaccine-associated benefit in VL control during ATI. This suggests that the effect of Vacc-4x (vs. placebo) in providing improved control of VL following ATI was more pronounced when the level of inflammation or immune activation was lower during transitioning off cART. Future research is needed to understand whether this finding applies to other HIV therapeutic vaccines. Nevertheless, our finding is consistent with previous reports that, as a marker of inflammation and immune activation, CRP concentration is elevated during HIV disease progression and is predictive of poorer outcomes. 15 –17 Since participants had just transitioned off cART at week 28, our finding supports the monitoring of inflammation and immune activation levels at this critical time point in studies that involve treatment interruption, and suggests the importance of such markers in predicting VE. It is out of the scope of this study to assess factors influencing the level of inflammation or immune activation during cART transition; however, our study highlights the importance of such research to maximize VE in selected study populations for future HIV therapeutic vaccine studies.
In addition, we found that a higher week 24 anti-C5/gp41732–744 antibody level fold-change over baseline was significantly associated with Vacc-4x benefit, in terms of both controlling VL and maintaining CD4 counts, during ATI. This is consistent with previous observations that the median VL set-point was lower in the Vacc-4x group compared to placebo among participants with baseline anti-C5/gp41732–744 antibody levels >4 μg/mL. 9 These findings suggest that the effect of Vacc-4x (vs. placebo) in providing improved control of VL and maintenance of CD4 count following ATI was more pronounced when the level of anti-C5/gp41732–744 antibody before transitioning off cART was higher.
There are a number of mechanisms, including antibody-dependent cell cytotoxicity activities, by which antibodies to this region may reduce immune activation, as demonstrated by antibodies to the C5 region of HIV-1 gp120. 18 In addition, the C5 19 and gp41 20 regions show amino acid homology to regions within HLA-DR and therefore have the potential to induce immune activation following presentation of these HLA-DR-like sequences on HLA-DQ molecules, which have been implicated in autoimmune diseases such as rheumatoid arthritis. 21 Antibodies to C5/gp41732–744 would therefore serve to reduce such immune activation. This finding further highlights the importance of monitoring immune activation and the use of such biomarkers in predicting VE in HIV therapeutic vaccine trials.
Overall, our findings from this study suggest that anti-C5/gp41732–744 antibodies may improve the Vacc-4x effect by reducing HIV-associated immune activation, which drives disease progression. Alternatively, low CRP and high anti-C5/gp41732–744 antibody levels may indicate low generalized immune activation, facilitating the VE.
This study has several limitations. First, not all potential biomarkers that could affect VL, for example, CCR5 coreceptor mutations, 22 were considered. However, the preART VL values of the study participants do not suggest that they possessed this mutation. 5,7 Second, due to the small sample size of this post-hoc study, each biomarker was only considered univariately as a potential predictor of VE. However, all reported analyses adjusted for preART VL or CD4 count as known prognostic factors of VL or CD4 count during ATI. Third, this study sought only to identify predictors of VE as a first step toward hypothesis generation and the identification of biomarkers as potential surrogates for VE. Due to the potential postrandomization imbalance in the treatment groups during ATI, larger prospective studies are needed to validate these findings.
In the absence of any intervention, VL generally returns to preART values on treatment interruption. 23 The accepted surrogate efficacy marker is therefore reduction in VL compared to placebo or compared to preART values. HIV cure initiatives require cART interruption to show effect. However, placebo-controlled treatment interruption studies impose ethical challenges, and preART values may become less informative as current guidelines recommend treatment at HIV diagnosis. Monitored antiretroviral pause (MAP) is emerging as a safer treatment interruption approach measuring time to virus rebound, where cART is reinitiated when VL reaches a specified level associated with minimal transmission risk. 24 Since MAP does not permit establishment of a VL set-point, the biomarkers identified in this study may play an important role as screening markers for safe cART interruption in participants most likely to experience vaccine benefit. Furthermore, safety markers such as CRP represent economical candidate biomarkers, since they are already routinely measured in vaccine trials. Finally, our results highlight the importance of immune activation in HIV pathogenesis and therapeutic vaccine research, where conditions of low immune activation, for example, high anti-C5/gp41732–744 antibody levels, and low CRP concentrations, are associated with therapeutic HIV vaccine (Vacc-4x) benefit.
Footnotes
Acknowledegments
This study was funded by Bionor Pharma AS. M.S., M.Ö., and G.S. were employees of Bionor Pharma AS when the study was carried out. The authors wish to thank the clinical study participants as well as the principal investigators: B. Peters, M. Fisher, G. Moyle, J. Rockstroh, D. Shürmann, G. Fätkenheuer, K. Arastéh A. Plettenberg, A. Lazzarin, B. Clotet, J. Gatell, D. Podzamczer, M. Fischl, D. Hardy, R. Mitsuyasu, D. Asmuth, and B. Taiwo. The authors would also like to acknowledge initial preliminary repeated measures analyses carried out by Bjarne Bodin at BioStata, Denmark.
Author Disclosure Statement
GS, ØJ, MÖ and MS were employees of Bionor Pharma AS during the study. The remaining authors have no conflicts of interest to report.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.