
Abstract
Human papillomavirus (HPV) infection is known to cause anal condyloma acuminatum (CA) and squamous cell carcinoma. Men who have sex with men (MSM) with HIV infection are frequently co-infected with HPV, especially high risk HPV (HR-HPV) that causes anal squamous cell carcinoma. However, there are few reports of HPV genotype studies in anal lesion of Japanese men. We tried to estimate the distribution of HPV genotypes in anal CA tissue specimens from the Japanese men to elucidate the risk of anal cancer. A total of 62 patients who had anal CA surgically excised were enrolled. They included 27 HIV-positive MSM, 18 HIV-negative MSM, 1 HIV-positive man who have sex with women (MSW), and 16 HIV-negative MSW. HPV genotypes in anal CA tissue were determined by the polymerase chain reaction technique with reverse line blot hybridization. HR-HPV was detected in 45.2% of the CA tissue specimens and high grade squamous intraepithelial lesion (HSIL) was observed in 15.3%. Moreover, the prevalence of HR-HPV in the HIV-positive MSM (70.4%) was higher than the HIV-negative MSM (33.3%, p = .0311) or the HIV-negative MSW (18.8%, p = .0016). The conditional logistic regression analysis suggested HIV positivity as the primary risk factor for the HR-HPV infection in CA. In addition, HSIL was detected in higher frequency in CA tissues from HIV-positive MSM (25.9%) than HIV-negative MSW (0.0%, p = .0346). HR-HPV and HSIL were frequently detected in anal CA tissues from Japanese MSM patients with HIV infection, suggesting the necessity of surveillance for this population.
Introduction
H
Previous reports have suggested that the distribution pattern of HPV genotype in the anal canal of MSM is epidemiologically analogous with that of cervical cancer. 2,14 –17 HPV genotypes 16, 18, 45, 31, and 33 are predominant in cervical cancer worldwide. 2 In Japan, the distribution of HPV genotype in cervical epithelia differs from that of other countries; HPV genotypes 52 and 58 are more frequent and genotype 45 is found less frequently in Japan. 2,18 Therefore, the distribution of HPV genotype in anal lesions of Japanese men would be similarly skewed as it is in Japanese women. However, there are few reports of HPV genotype studies on anal lesions in Japanese men 19 –21 ; HR-HPV was frequently found in the CA swab specimens from HIV-positive Japanese patients. Additionally, several studies reported the distribution pattern of HPV genotype from tissue or swab specimens of CA. 6,7,19,20,22,23
Anal CA is treated with trichloroacetic acid, imiquimod, podophyllin resin, cryotherapy with liquid nitrogen, laser ablation, or surgical excision 24 –27 ; surgical excision is performed for intra-anal canal, large-sized, or recurrent CA. The quadrivalent vaccine against HPV genotypes 6, 11, 16, and 18 and the bivalent against 16 and 18, are employed worldwide for the prevention of cervical HPV infection 28,29 and are known to be effective for preventing cervical cancers. 28,29 These vaccines could be effective for the prevention of anal HPV infection, anal high grade squamous intraepithelial lesion (HSIL), or anal cancer.
In this study, we tried to investigate the distribution of HPV genotype in surgically excised anal CA tissue specimens from Japanese men to elucidate the risk of anal cancer in Japanese men with CA and the possibility of the prevention of anal cancer by HPV vaccines.
Materials and Methods
Patients
Sixty-two male patients with anal CA were treated at Tokyo Yamate Medical Center between November 2013 and April 2015. All patients were native Japanese living in Japan and were candidates for surgical excision of perianal and/or intra-anal canal CA as treatment, suffering from intra-anal canal, large-sized, or recurrent CA. Of 62 male patients, 45 were MSM (HIV-positive: 27, HIV-negative: 18) and 17 were men who have sex with women (MSW) (HIV-positive: 1, HIV-negative: 16). The surgical procedure was performed with surgical scalpel or electric cautery by experienced seven surgeons. The surgically excised CA tissues were fixed in 10% formalin, embedded in paraffin, and cut into sections that were stained with hematoxylin and eosin. Based on the criteria of HPV-associated squamous lesions of the lower anogenital tract, 30 pathological diagnosis of HSIL in CA tissue was determined by the pathologist (K.I.), who was blinded to the data of the clinical information and HPV typing. The excised CA tissue was treated with RNAlater Stabilization Solution® (Thermo Fisher Scientific, Inc., Waltham, MA) and was stored at −80°C until HPV genotyping. Clinical information of patients was retrieved from medical records. The body mass index (BMI) is body weight divided by square of height. Pretreated CA patients were defined as CA patients who were previously treated with therapeutic approaches for CA before the recruitment for the study. Recurrent CA patients were patients who had relapsed CA after the surgical procedure in this study. Intra-anal canal CA lesion was detected with anoscopy. The antiretroviral therapy treatment was defined as the treatment with at least two nucleoside analog reverse transcriptase inhibitors and protease inhibitor, non-nucleoside reverse transcriptase inhibitor, or integrase inhibitor. Infection of hepatitis B virus (HBV) or hepatitis C virus (HCV) was determined by the detection of HBs antigen or anti-HCV antibody, respectively. Treponema pallidum infection was detected with serologic test for syphilis (STS) and T. pallidum hemagglutination (TPHA) tests. HIV copy number was estimated with real-time reverse transcription-polymerase chain reaction (PCR) methods and CD4+ T cell was counted with flow cytometric analysis. This study was reviewed and approved by Tokyo Yamate Medical Center Research Ethics Committee and Nagoya Medical Center Research Ethics Committee. Written informed consent was obtained from all study participants. This study was conducted in accordance with the principles expressed in the Declaration of Helsinki.
HPV genotyping
DNA was extracted from excised CA tissue using the QIAamp DNA Blood kit® (Qiagen, Venlo, Netherlands). Genotyping of HPV was performed by the PCR technique with reverse line blot hybridization (Linear Array HPV genotyping test®; Roche Diagnostics, Basel, Switzerland), which allows us to detect 37 genotypes (HR-HPV: 16, 18, 31, 33, 35, 39, 45, 51, 52 mix, 56, 58, 59, and 68, LR-HPV: 6, 11, 26, 40, 42, 53, 54, 55, 61, 62, 64, 65, 67, 69, 70, 71, 72, 73, 81, 82, 83, 84, IS39, and CP6108).
Statistical analysis
Association of clinical features or HPV genotypes of the CA patients was tested by Fisher's exact test using 2 × 2 contingency tables or Mann–Whitney's U test. p Values less than .05 were considered to be statistically significant. To examine which of the clinical features was primarily associated with the infection of HR-HPV in CA patients, conditional logistic regression analysis was employed and the deviation from 0 was evaluated for coefficients by the Wald test.
Results
Characteristics and HPV genotype distribution of CA patients
Clinical features and HPV genotype distribution of the CA patients are shown in Table 1 and Figure 1. Among these CA patients, 28 were HIV-positive (45.2%) and 45 were MSM (72.6%). TPHA test was positive in 16 patients with CA (26.7%). The HSIL was pathologically observed in 9 CA tissue specimens (15.3%). HPV was detected in all the specimens from CA patients. The average number of co-infected HPV genotypes was 4.0. LR-HPV was detected in all the specimens from CA patients. HPV genotypes 6 (34 [55.7%]) and 11 (39 [63.9%]) were predominant. In contrast, HR-HPV was detected in the specimens from 28 (45.2%) patients. HPV genotypes 16 (9 [14.8%]), 51 (9 [14.8%]), 52 (13 [21.38%]), and 58 (19 [31.1%]) were predominant.
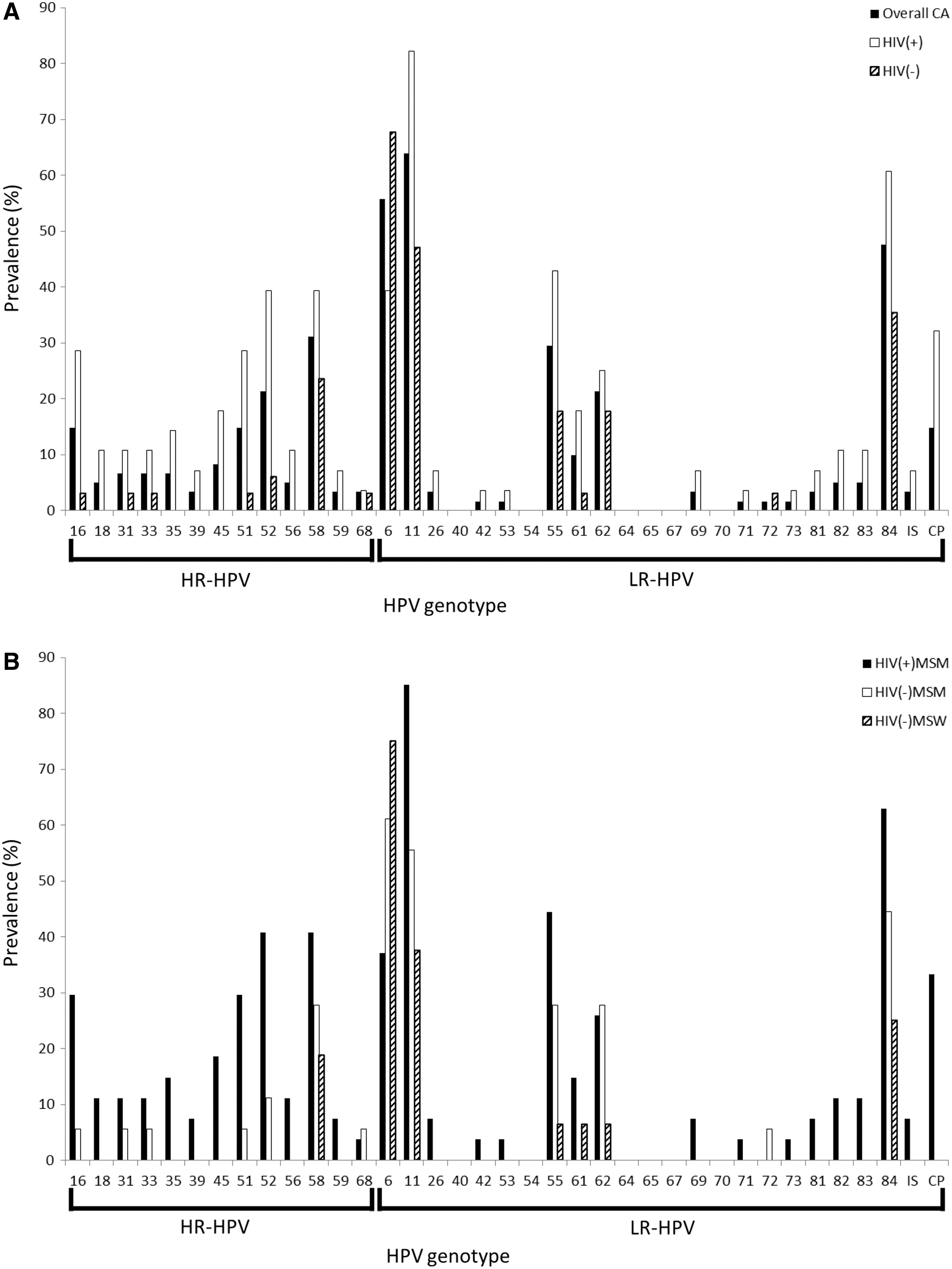
Distribution of HPV genotypes in CA patients.
Numbers or average values of each group are shown. Percentages or standard deviations are shown in parenthesis. Difference was tested by Mann–Whitney's U test or Fisher's exact test using 2 × 2 contingency tables.
Fisher's exact test was employed.
ART, antiretroviral therapy; BMI, body mass index; CA, condyloma acuminatum; HBV, hepatitis B virus; HCV, hepatitis C virus; HIV(−), HIV negative; HIV(+), HIV positive; HPV, human papillomavirus; HR-HPV, high risk HPV; HSIL, high grade squamous intraepithelial lesion; LR-HPV, low risk HPV; MSM, men who have sex with men; STS, serologic test for syphilis; TPHA, Treponema pallidum hemagglutination.
Characteristics and HPV genotype distribution of CA patients with or without HIV infection
Clinical features and HPV genotype distribution of the HIV-positive CA patients were compared with that of HIV-negative CA patients (Table 1). Among the HIV-positive patients, the percentage of MSM is higher than HIV-negative patients (27 [96.4%] vs. 18 [52.9%], p = .0001). The BMI in HIV-positive patients was lower than that of negative patients, whereas TPHA test was more frequently positive.
The prevalence of HR-HPV was significantly higher in HIV-positive patients (19 [67.9%] vs. 9 [26.5%], p = .0019). The number of co-infected HPV genotypes was higher in HIV-positive patients, in addition to that of HR-HPV and LR-HPV genotypes. Of HR-HPV, HPV genotype 16, 51, 52, and 58 were frequently detected in HIV-positive patients (Fig. 1). HPV genotype 58 was also found in HIV-negative patients. Thus, higher prevalence of HR-HPV in HIV-positive patients was found, suggesting the cause of anal intraepithelial neoplasia in CA in these patients.
Characteristics and HPV genotype distribution of HIV-positive MSM, HIV-negative MSM, and HIV-negative MSW
Clinical features of HIV-positive MSM, HIV-negative MSM, and HIV-negative MSW are presented in Table 2. Since the number of HIV-positive MSW was one, the data of this group could not be compared with those of other groups. HIV-negative MSM patients were younger than HIV-positive MSM and HIV-negative MSW. The BMI in HIV-negative MSW was higher than either HIV-positive or HIV-negative groups. STS and TPHA test in HIV-positive MSM were more frequently positive than that in HIV-negative MSW. Intra-anal canal CA lesions were more frequently detected in HIV-positive and negative MSM. The HSIL was detected in higher frequency in CA tissues from HIV-positive MSM (25.9%) than HIV-negative MSW (0.0%, p = .0346), suggesting the association between HIV infection and anal cancer.
Numbers or average values of each group are shown. Percentages or standard deviations are shown in parenthesis. Difference was tested by Mann–Whitney's U test or Fisher's exact test using 2 × 2 contingency tables.
Fisher's exact test was employed.
MSW, men who have sex with women.
The prevalence of HR-HPV in HIV-positive MSM was significantly higher than HIV-negative MSM (19 [70.4%] vs. 6 [33.3%], p = .03) or HIV-negative MSW (19 [70.4%] vs. 3 [18.8%], p = .002). The number of co-infected HPV genotypes in HIV-positive MSM was higher than that of HIV-negative MSM or HIV-negative MSW. Similar patterns were found for the number of co-infected HR-HPV and LR-HPV genotypes. HPV genotypes 16, 51, 52, and 58 were frequently found in HIV-positive MSM, though HPV genotype 58 was also found in HIV-negative MSM and HIV-negative MSW (Fig. 1). Consequently, the prevalence of HR-HPV was higher in HIV-positive MSM compared with HIV-negative MSM or HIV-negative MSW.
Some clinical features of HIV-positive MSM patients with CA were distinguishing (Table 2). To elucidate which of the clinical features was primarily associated with HR-HPV infection, conditional logistic regression analysis was performed (Table 3). In unconditioned analysis, HIV positivity was associated with HR-HPV infection (p = .0016, odds ratio [OR] 5.86, 95% confidence interval [CI] 1.95–17.61). BMI (p = .0401, OR 0.86, 95% CI 0.75–0.99) and MSM (p = .0122, OR 5.83, 95% CI 1.47–23.16) were also associated with HR-HPV infection to a lesser degree. Next, the conditioned analysis on HIV positivity was performed. No association of the clinical manifestations remained significant, when conditioned on HIV positivity, authenticating HIV positivity as the primary risk factor among these clinical manifestations for the HR-HPV infection in CA.
The association of the clinical features with HR-HPV infection was analyzed with logistic regression analysis. The left column indicates the results from unconditioned analyses. The right column indicates the results from analyses conditioned on HIV positivity. p, OR, 95% CI, p adjusted, ORadjusted were calculated by logistic regression analysis.
CI, confidence interval; NA, not applicable; OR, odds ratio.
Discussion
CA has been known as a benign disease caused by LR-HPV. However, HR-HPV was reported to be frequently co-infected in CA from MSM infected with HIV. 6,7 this study is the first to evaluate the distribution pattern of HPV genotypes and the pathological features of anal CA tissue specimens from the Japanese men. HR-HPV and HSIL were frequently detected in anal CA tissues from Japanese MSM patients with HIV infection (Table 2). Additionally, conditional logistic regression analysis confirmed that HIV positivity is the primary risk factor for the HR-HPV infection in CA (Table 3) among the clinical manifestations including BMI, MSM, HBV, STS, and TPHA. The lower BMI values, MSM, and the infections of HBV or T. pallidum superficially seemed to be risk factors, but would be confounding factors of HIV infection. HR-HPV is highly oncogenic and can cause many types of cancer including anal cancer, cervical cancer, vulvar cancer, vaginal cancer, penile cancer, oral cancer, and oropharyngeal cancer. In addition, the distribution pattern of HR-HPV genotype in specimens from cervical cancer in Japan was widely different from that of other countries; HPV genotype 16 was predominant, but 52 and 58 were more frequent than other countries. 2,18 However, there are few reports studying the HPV genotype in anal lesion of Japanese men 19 –21 ; precise distribution pattern of HPV genotype have yet to be reported. Thus, we chose to analyze HPV genotypes in anal CA tissues from Japanese men. HR-HPV in anal CA tissues was found in significantly higher frequencies among HIV-positive Japanese MSM. The distribution of HR-HPV genotype in Japanese men was skewed similar to that of Japanese women. This could be explained by the ethnic difference of HPV resistant HLA allele frequencies. 31 Further HPV genotyping studies using next-generation sequencing are necessary for the precise analysis of distribution pattern of genotypes other than the 37 typed in this study.
Although HPV genotype of the surgically excised anal CA tissues was analyzed in this study (Fig. 1), the distribution pattern of HPV genotype might not be the same as that of swab specimens from anal CA or anal canal. 22 The distribution pattern of HPV genotype of CA specimens in this study was not the same as that of swab specimens from anal canal of Japanese men with HIV 21 ; HPV genotypes 52 and 58 in HIV-positive MSM were more frequent in this study. These differences could be also explained by the different parent populations, HIV-infected patients and CA patients. Thus, distribution of HPV genotype also should be investigated using anal swab specimens from anal CA in Japanese men for the establishment of screening methods of anal cancer.
The HSIL was frequently observed in tissue specimens from anal CA of HIV-positive Japanese MSM (Table 2, 25.9%). These results suggest that HR-HPV in CA tissue of HIV-positive Japanese MSM might cause HSIL, which may potentially lead to the development of anal cancer. Japanese HIV-positive MSM may have a higher risk for anal cancer, as it was indicated in other countries. 9,13 The significant association with HSIL was not observed in the comparison between HIV-positive MSM and HIV-negative MSM (Table 2), because of the modest sample size.
This investigation is a cross-sectional study and further prospective cohort study is required. Since the sample size of this study is modest, the prevalence of HSIL in anal CA among HIV-positive MSM needs to be confirmed in future larger scale studies in Japan.
Two prophylactic HPV vaccines, the quadrivalent vaccine against HPV genotypes 6, 11, 16, and 18 and the bivalent against 16 and 18, are available in the most countries. 28,29 The efficacy of HPV vaccines at preventing cervical cancers has been shown definitely. 28,29 and the similar efficacy of the HPV vaccines against anal intraepithelial neoplasia also is being reported. 32 Although these HPV vaccines could potentially prevent anal cancer caused by HPV genotype 16 they may not induce immunogenic reactions against HPV genotypes 51, 52, or 58 that were frequently detected in Japanese MSM with HIV infection. Both the development and optimized availability of multivalent vaccines are expected.
The positivity of HR-HPV in anal CA tissue was significantly higher in HIV-positive Japanese MSM; HPV genotypes 16, 51, 52, and 58 were predominant. To the best of our knowledge, this is the first study on the precise distribution patterns of HPV genotype in anal CA tissues of Japanese men.
Footnotes
Acknowledgments
This research was partially supported by the Practical Research Project for HIV/AIDS from Japan Agency for Medical Research and Development, AMED. The funders had no role in study design, data collection and analysis, decision to publish, or preparation of the article.
Author Disclosure Statement
SF received honoraria from Mitsubishi Tanabe Pharma Corporation, Maruho Co., Ltd., EA Pharma Co., Ltd., Kyorin Pharmaceutical Company, Limited, Amato Pharmaceutical Products, Ltd., and Merck Sharp & Dohme Corporation. WS was supported by research grants from Abbott Japan Co., Ltd. WS is an employee of GlaxoSmithKline K.K. since April 2015. WS contributed to the study while he was an employee of Nagoya Medical Center. The other authors declare no financial or commercial conflict of interest.