
Abstract
Antiretroviral drug concentrations at sites of HIV exposure are important drivers that influence the development of HIV pre-exposure chemoprophylaxis strategies and regimens. We assessed the effect of collection method—in the presence or absence of tissue culture medium—on tenofovir (TFV) and tenofovir diphosphate (TFV-DP) concentrations in colonic biopsies. We find significant baseline interbiopsy variation in TFV (38% CV) and TFV-DP (33% CV) concentrations. Incubation in medium leads to a fluid absorption-driven twofold increase in tissue weight with a concomitant 75% decrease in weight-adjusted tissue TFV concentrations 120 min post-incubation. In contrast, adjusted TFV-DP concentrations decrease by only 25% during the same period, with this difference not achieving statistical significance. Although colonic biopsies should be collected in the absence of medium for accurate TFV concentrations, the presence of medium does not significantly impact TFV-DP-dependent pharmacokinetic or pharmacodynamic assays. Appropriate assessment of tissue drug concentrations should account for biopsy collection method and drug mechanism of action.
S
One efficient method for tissue collection involves placing biopsies directly into culture medium from biopsy forceps, allowing rapid collection and storage for downstream processing. 2 Biopsies can also be collected in the absence of medium—individual pieces are directly transferred to a storage vial. In previous studies, collecting biopsies in medium required ∼20 seconds per biopsy (7 procedures, 30 biopsies each), whereas direct transfer of biopsies (16 procedures, 4 biopsies each) required ∼32 seconds per biopsy, a significant difference (p < .05). Importantly, direct collection requires additional personnel to transfer tissue to cryovials. The effect of collection method on tissue drug concentrations has not been studied directly. We have assessed the influence of medium incubation on tissue tenofovir (TFV) and intracellular tenofovir diphosphate (TFV-DP) concentrations in colonic biopsies.
After Institutional Review Board (IRB) approval and informed consent, 30 colorectal biopsies were collected from a male volunteer on a TFV-containing HIV treatment regimen. Biopsies were collected between 10 and 20 cm from the anal verge using an Olympus flexible sigmoidoscope and Radial Jaw™ 4 Jumbo forceps. The first six biopsies were transferred directly into six separate preweighed cryovials without contact with culture medium; biopsies were collected for 5 min and frozen within 20 min. The remaining 24 biopsies, collected over the subsequent 10 min, were transferred to either 2 or 20 mL aliquots of medium (Roswell Park Memorial Institute [RPMI] with 10% fetal bovine serum, three biopsies per aliquot) and incubated for 10, 30, 60, or 120 min before weighing and freezing. The 120 min cohort was the first batch submerged while the 10 min cohort was the last group processed. TFV and TFV-DP concentrations were measured using ultra performance liquid chromatography-tandem mass spectrometry (UPLC-MS/MS). Analyte measurements were normalized to tissue weights to obtain tissue concentrations. The volunteer's adherence to treatment was confirmed by measuring TFV in blood plasma via UPLC-MS/MS. 2
There was large interbiopsy variation in TFV (176–428pg/mg, 38% CV) and TFV-DP (33–77 fmol/mg, 33% CV) concentrations among biopsies collected without medium, reflecting physiological heterogeneity in drug content of individual biopsies. Biopsy weights, TFV concentrations, and TFV-DP concentrations varied markedly between biopsy groups processed in the presence or absence of medium. There was no significant difference between tissue weights and drug/metabolite concentrations between biopsies incubated in either 2 or 20 mL medium for any given time point (p > .1). Therefore, these groups were pooled for analysis.
There was marked change in average tissue weight postmedium incubation. Average weight increased rapidly, stabilized at approximately twofold by 60 min (Fig. 1A), and was constant through 120 min. This rapid increase and eventual stabilization of weights suggest medium absorption and retention by colonic biopsies. RPMI medium used for collection is iso-osmolar, suggesting that absorption is due to mucus associated with the tissue, rather than the tissue itself. Changing medium osmolality may lead to decreased absorption, but is likely to have detrimental effects on tissue cells.
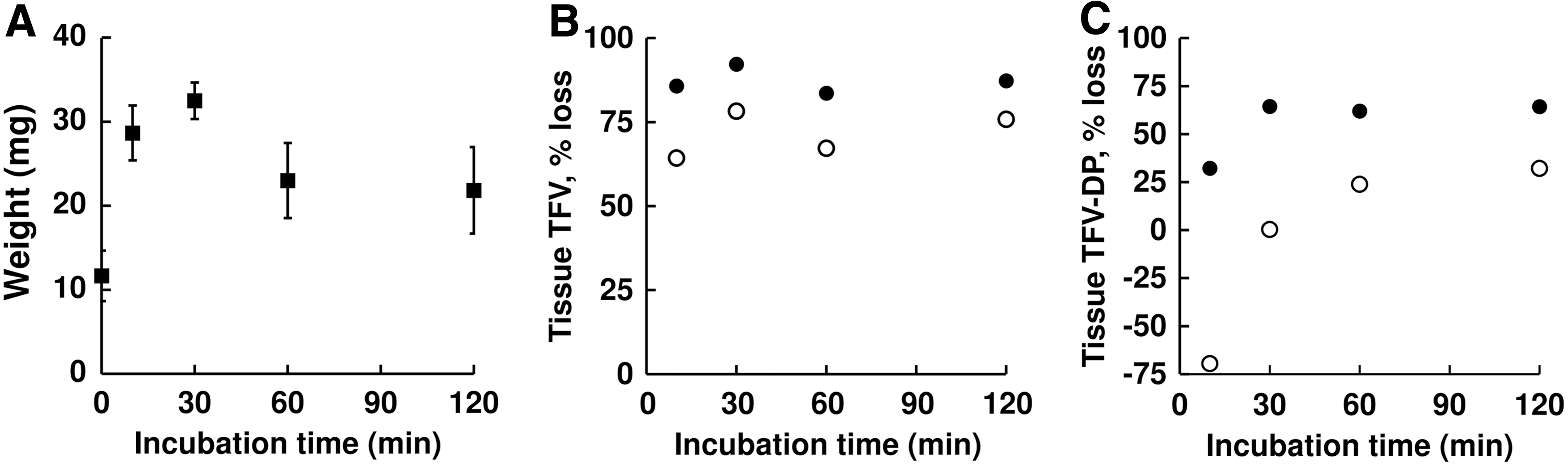
Effect of incubation upon biopsies.
Tissue TFV concentrations decreased upon incubation in medium. There was 85% loss within 10 min, with no decrease thereafter to 120 min (Fig. 1B, filled circles). Because tissue drug concentrations are normalized to tissue weight, the observed weight increase with medium incubation further decreases apparent tissue concentrations. Adjusting TFV concentrations for this weight increase (measured concentration multiplied by fold weight change) revealed a weight-adjusted decrease of ∼75% in tissue TFV concentration (Fig. 1B, open circles), likely due to loss of “available” TFV into incubation medium. Detection of TFV in incubation medium (up to 2.1 ng/mL) corroborated these findings. Matrix-dependent differences in assay methods and sensitivities make a direct comparison between tissue and medium drug concentrations impractical. The sum of drug concentrations in tissue and collection medium for pharmacokinetic (PK) analysis is not scalable and can result in an inaccurate interpretation of drug loss. For accurate tissue TFV measurements, tissue needs to be collected without incubation in medium.
Tissue TFV-DP revealed a similar loss of drug (Fig. 1C, closed circles). Concentrations decreased up to 30 min postmedium incubation, and then remained stable up to 120 min, with a ∼70% loss compared with nonmedium incubated biopsies. However, a major portion of this apparent loss was accounted for by the weight increase that occurred with medium retention. There was an apparent weight-adjusted loss of ∼25% for TFV-DP upon incubation (Fig. 1C, open circles). Differences between nonincubated biopsies and tissue incubated for 30, 60, or 120 min did not achieve statistical significance (p > .1), likely due to large interbiopsy variation in TFV-DP within each cohort. It is possible that the tissue trauma during pinch collection causes cellular damage and release of intracellular drug. In addition, there may be cell lysis when primary tissue is introduced into RPMI, a milieu approximating, but not identical to, in vivo conditions. Any or all of these factors may contribute to the variation in TFV-DP concentrations seen in the experiment. Nevertheless, incubated colonic biopsies provide a reasonable estimate of TFV-DP concentrations in vivo.
Large interbiopsy variation in TFV and TFV-DP concentrations seen in this study is worth noting and demonstrates that PK analyses from single sample measurements must be interpreted with caution. Incubation of biopsies in medium caused a significant increase in tissue weight, likely due to medium retention (Fig. 1A). Medium incubation caused significant reductions in tissue TFV concentrations (weight adjusted and nonweight adjusted), with ∼75% loss of TFV (Fig. 1B), suggesting that the tissue TFV concentration measured in an incubated biopsy may be a gross underestimate of what is found in colonic tissue at the time of collection. In clinical trials, incubation time for tissue collected in solution varies between sample collections, and will impact the heterogeneity observed in tissue TFV concentrations. In contrast to TFV, a large portion of the decrease in tissue TFV-DP concentrations was accounted for by medium retention (Fig. 1C, open circles). Robustness of tissue TFV-DP has important implications for PK–pharmacodynamic (PK–PD) studies. TFV-DP concentrations in isolated mucosal mononuclear cells are a relevant and important PK outcome. Cell isolation requires incubation of tissue in medium for up to 2 h postcollection. Our results suggest that TFV-DP concentrations in isolated MMCs will closely approximate intracellular concentrations in tissue at the time of collection. Ex vivo explant and HIV-infection assays are used as PD surrogates for drug efficacy. 3 These assays involve 2 h of submerged incubation post-HIV challenge, and the pharmacological status of the tissue during and after this incubation has been of concern. We find TFV-DP concentrations to be stable throughout the incubation period (Fig. 1C, open circles). Drug loss during processing is an unlikely contributor to either the observed large inter- and intra-assay in these assays, or the discrepancy in IC90s between ex vivo and in vivo estimates. 4,5
This study also has limitations. First, TFV and TFV-DP are specific in that TFV is converted intracellularly to a membrane-impermeable charged active metabolite (TFV-DP). Second, we have relied on using multiple samples from a single volunteer on oral therapy in an attempt to avoid confounding effects of interindividual variation. The principles derived from our findings, however, should apply to topically dosed drugs, to drugs with similar pharmacologic characteristics, to colorectal biopsies in general, and to cervicovaginal biopsies.
To summarize, biopsy collection methods should be guided by outcomes desired. An accurate estimate of total tissue TFV requires dry collection of biopsies. Accurate PK/PD linkages demand that biopsies used for drug measurement and PD assays must be treated identically. Comparing results between/within studies must account for sample collection/processing methods.
Footnotes
Acknowledgments
We are grateful to the study volunteer and staff of Johns Hopkins Gastroenterology. This study was sponsored by the U.S. National Institutes of Health (NIH), including the National Institute of Allergy and Infectious Diseases (NIAID) under the program project grant 1U19AI113127-01.
Author Disclosure Statement
No competing financial interests exist.