
Abstract
To identify factors that predispose human immunodeficiency virus (HIV)-exposed uninfected infants (HEUs) to higher incidence of severe infections, hospitalization, and death in the first 6–24 months of life compared with HEUs with and without lower respiratory tract infection (LRTI) in the first 6 months of life. Nested case–control study of 107 LRTI+ infants enrolled in the International Site Development Initiative (NISDI) Perinatal and Longitudinal Study in Latin American Countries (LILAC) studies with and 140 LRTI− in the first 6 months, matched by date and place of birth. Infants and mothers had plasma antibodies measured against respiratory syncytial virus (RSV), parainfluenza (PIV) 1, 2, 3, influenza, and pneumococcus 1, 5, 6B, and 14. Compared with LRTI−, mothers of LRTI+ HEUs had lower years of education, lower CD4+ cells, and higher HIV plasma viral load at delivery, but similar use of antiretrovirals and cotrimoxazole and other sociodemographic characteristics. LRTI+ and LRTI− HEUs had similar demographic and hematological characteristics and antibody concentrations against respiratory pathogens at birth. At 6 months, the rates of seroconversions to respiratory pathogens and antibody responses to tetanus vaccine were also similar. However, antibody concentrations to RSV were significantly higher in LRTI+ compared with LRTI− HEUs and marginally higher to PIV1. Maternal factors associated with advanced HIV disease, but unrelated to the use of antiretrovirals, cotrimoxazole, or the level of maternal antibodies against respiratory pathogens, contribute to the increased risk of LRTI in HEUs. In HEUs, antiretroviral and cotrimoxazole use, exposure to respiratory pathogens and humoral immune responses were not associated with the incidence of LRTI.
Introduction
I
Both maternal and infant factors may contribute to the increased susceptibility of HEUs to infections. Maternal HIV infection (especially untreated) compromises vigorous antibody responses to infections and vaccines and produces high concentrations of nonspecific immunoglobulin G (IgG) that compete for the placental IgG receptors. This is reflected in decreased transplacental transfer of pathogen-specific, protective antibodies in HEUs. 16,17 In addition, HEUs may have their own functional immune defects compared with HUUs, including decreased antibody and cellular immune responses to vaccines and decreased natural killer functionality. 18 –25 HEUs have other phenotypic immune differences compared with HUUs, for which functional significance remains to be determined.
The goal of this study was to determine the contributions of common respiratory viruses and Streptococcus pneumoniae (PNC) to the burden of LRTI in HEUs and identify actionable maternal and infant characteristics associated with the risk of LRTI. To this end, we conducted a nested case–control study of LRTI+ and LRTI− HEU infants enrolled in the NISDI Perinatal and LILAC cohorts.
Participants and Methods
Study population
This study used archived plasma from the NISDI Perinatal and LILAC prospective cohort studies. These previously described studies aimed to characterize adverse events in pregnant women with HIV and their HIV-uninfected offspring. 26 The studies were approved by the local Institutional Review Boards and written informed consent was obtained from each participant. Subjects were enrolled during the years 2002–2009. Women eligible to participate had access to antiretrovirals (ARVs), and their infants had access to formula feeding.
Maternal study visits were conducted during pregnancy, at delivery, and hospital discharge, and 6–12 weeks and 6 months postpartum (Perinatal) or every 6 months up to 2 years postpartum (LILAC). Study visits for the infants were conducted at birth, 6–12 weeks and 6 months of age (Perinatal), and every 6 months thereafter (LILAC). During these visits, a medical history was obtained, a physical examination was performed, and blood samples were collected for laboratory studies and for plasma storage at −70°C in a central repository. Infants were considered HIV uninfected if they had ≥2 negative HIV nucleic acid tests with one test performed at ≥1 month and one at ≥4 months of age or if they had ≥2 negative HIV antibody test results, including ≥1 negative test result after 6 months of age.
NISDI Perinatal and LILAC HEUs were included in this analysis if they were born in Brazil, with gestational age >37 weeks, birth weight >2,500 g, and with at least 6 months of follow-up. Multiple gestation births and children with severe underlying cardiovascular or pulmonary conditions were excluded.
As shown in Figure 1, of the children who satisfied the inclusion criteria, we selected 144 children that developed LRTIs (LRTI+) and 144 controls that did not develop LRTIs in the first 6 months of life (LRTI−). An LRTI was defined as having occurred when either a definitive or a presumptive diagnosis of an LRTI was recorded. An infection was considered incident if the infant had been free of any signs and symptoms consistent with the same LRTI for at least 7 days before the incident event. Twenty-five LRTI+ HEUs, whose LRTIs were diagnosed after 6 months of age, were reclassified as LRTI−. Although LRTI+ HEUs could have up to three LRTI− HEUs matched, eight LRTI− were not included in the analysis because they did not have a matched case. In addition, 33 (12 LRTI+ and 21 LRTI−) infants were withdrawn from the analysis because they received ≥1 dose of pneumococcal conjugate vaccine before the 6-month study visit.
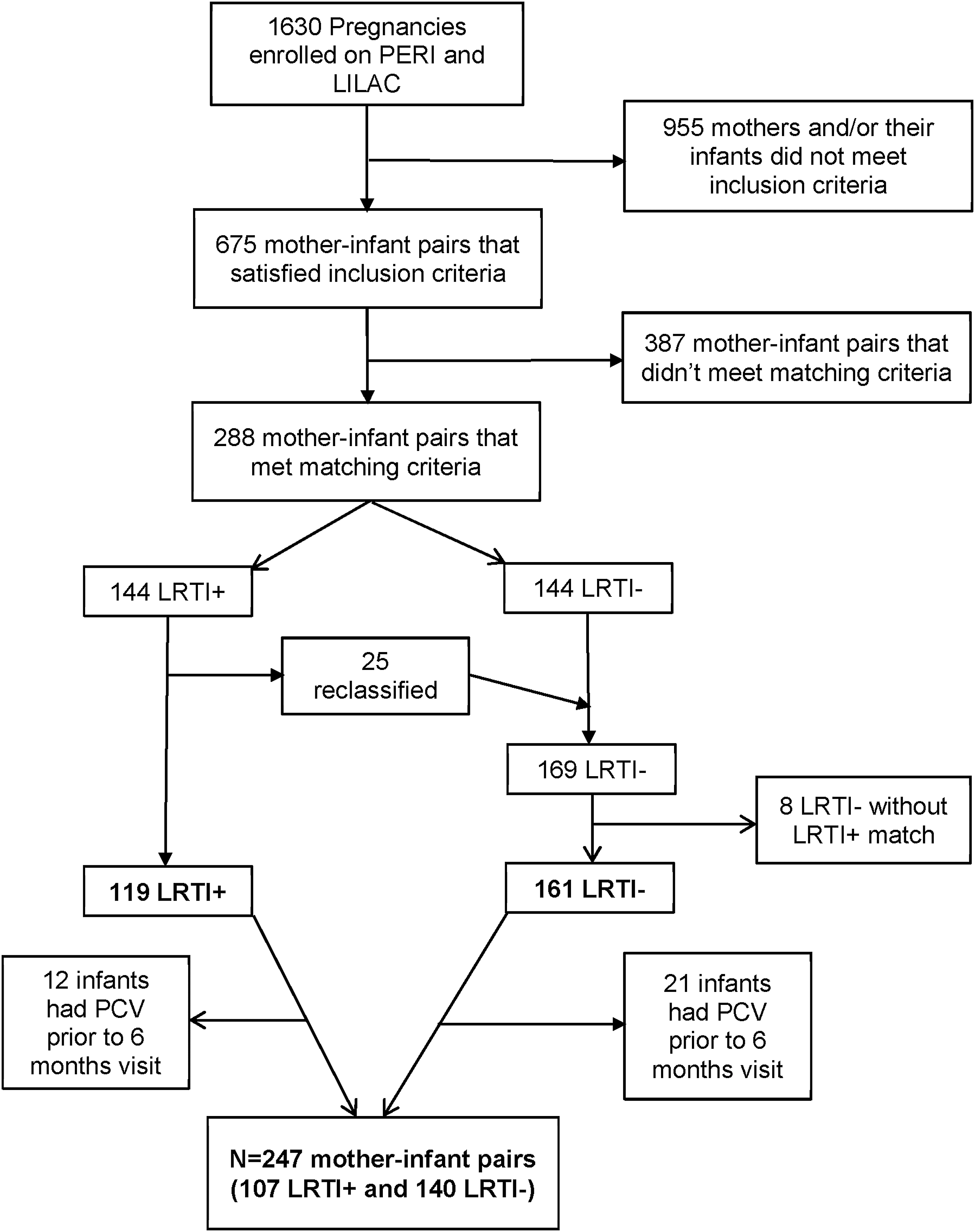
Consort diagram. LRTI, lower respiratory tract infection; PCV, pneumococcal conjugate vaccine.
Laboratory assays
ELISA for antibodies against influenza A, respiratory syncytial virus, parainfluenza 1, 2, and 3, and tetanus
These assays were performed by technologists blinded to the group allocation of the sample using the following kits according to the manufacturer's instructions for quantitative assays: Influenza A IgG ELISA (IBL America), respiratory syncytial virus (RSV) IgG ELISA (IBL America), VIR-ELISA Anti-Parainfluenza (PIV) 1–IgG/IgA (Viro-Immun Labor-Diagnostika Gmbh, Germany), VIR-ELISA Anti-PIV 2–IgG/IgA (Viro-Immun Labor-Diagnostika Gmbh), VIR-ELISA Anti-PIV 3–IgG/IgA (Viro-Immun Labor-Diagnostika Gmbh), and Tetanus IgG ELISA (IBL America), respectively. Laboratory-specific high- and low-positive controls were included in each run as an additional quality assurance of the quantitative aspect of the test. Assays were considered valid when all controls performed as expected. The concentration of antibodies in each plasma sample was calculated by interpolation on a standard curve using Prism 4 (GraphPad, USA) or Excel (Microsoft, USA) software.
ELISA for anti-PNC antibodies
Anticapsular IgG antibody concentrations against serotypes 1, 5, 6B, and 14 were measured using a previously described ELISA protocol that measures binding of serotype-specific IgG to antigen-coated ELISA wells. 27,28 Plasma at a 1:10 dilution in phosphate-buffered saline containing 0.1% Tween 20% and 1% bovine serum albumin was incubated for one hour at room temperature with cell wall polysaccharide at 50 μg/mL and 22F polysaccharide at 40 μg/mL to absorb nonspecific binding antibodies. Absorbed samples from the mother and infant pairs were assayed simultaneously. The antibody concentration in test samples was calculated by interpolation in the standard curve using Prism software (GraphPad).
Statistical analyses
Continuous variables were described using mean and standard deviations or geometric mean concentrations and 95% confidence intervals. p Values for assessing differences between groups (LRTI+ vs. LRTI−) were investigated by linear mixed-effects models to adjust for one-to-n matching, with LRTI status as a predictor. In some of the models, other covariates, such as infant antibody concentration measured at birth, were also included for adjustment. Categorical variables were described by frequencies and proportions and differences by groups analyzed by conditional logistic regression for one-to-n matching, as appropriate. Seroconversion by 6 months of life was defined by ≤2-fold decrease or an increase in antibody concentrations compared with birth. Differences between groups in mean infant/mother antibody ratios and infant antibody concentrations at birth and 6 months were assessed by linear mixed-effects models. All analyses were performed using SAS version 9.4 (SAS Institute, Inc., Cary, NC).
Results
Maternal and infant characteristics at birth
Table 1 shows the demographic and social characteristics of the study population. Maternal characteristics were similar between LRTI+ and LRTI− groups, with the exception of completed years of education, which was higher in LRTI− compared with LRTI+ mothers. In contrast, HIV disease characteristics around the time of birth differed between groups, with LRTI+ mothers having lower CD4+ T-lymphocyte (CD4) cell counts and percent and higher HIV plasma viral loads compared with LRTI− mothers. There were no significant differences with respect to gestational age, intrauterine growth, and hematological parameters at birth between LRTI+ and LRTI− infants.
Bolded p values indicate significant and marginal differences. To adjust for one-to-n matching, p values for continuous measures were calculated by linear mixed-effects models; p values for categorical measures were calculated by conditional logistic regression.
LRTI, lower respiratory tract infection; HIV, human immunodeficiency virus.
STD, standard deviation.
Maternal antibody transfer
At delivery, maternal antibody concentrations against RSV, and PNC1, 5, 6B, and 14 were similar in LRTI+ and LRTI− mothers (Fig. 2). Transplacental transfer of antibodies, defined as the mean of the infant:mother ratio at birth, tended to be lower against RSV and PNC5 in mothers of LRTI+ infants, without reaching statistical significance, and were similar for PNC1, 6B, and 14 (Table 2). Antibody concentrations at birth did not differ between LRTI+ and LRTI− infants (Table 2).
Maternal antibodies at delivery.
Bolded p values indicate marginal differences. To adjust for one-to-n matching, all p values were calculated by linear mixed-effects models.
N, no. of participants tested; GMC, geometric mean concentration; RSV, respiratory syncytial virus; PIV, parainfluenza; CI, confidence intervals.
EU, ELISA units.
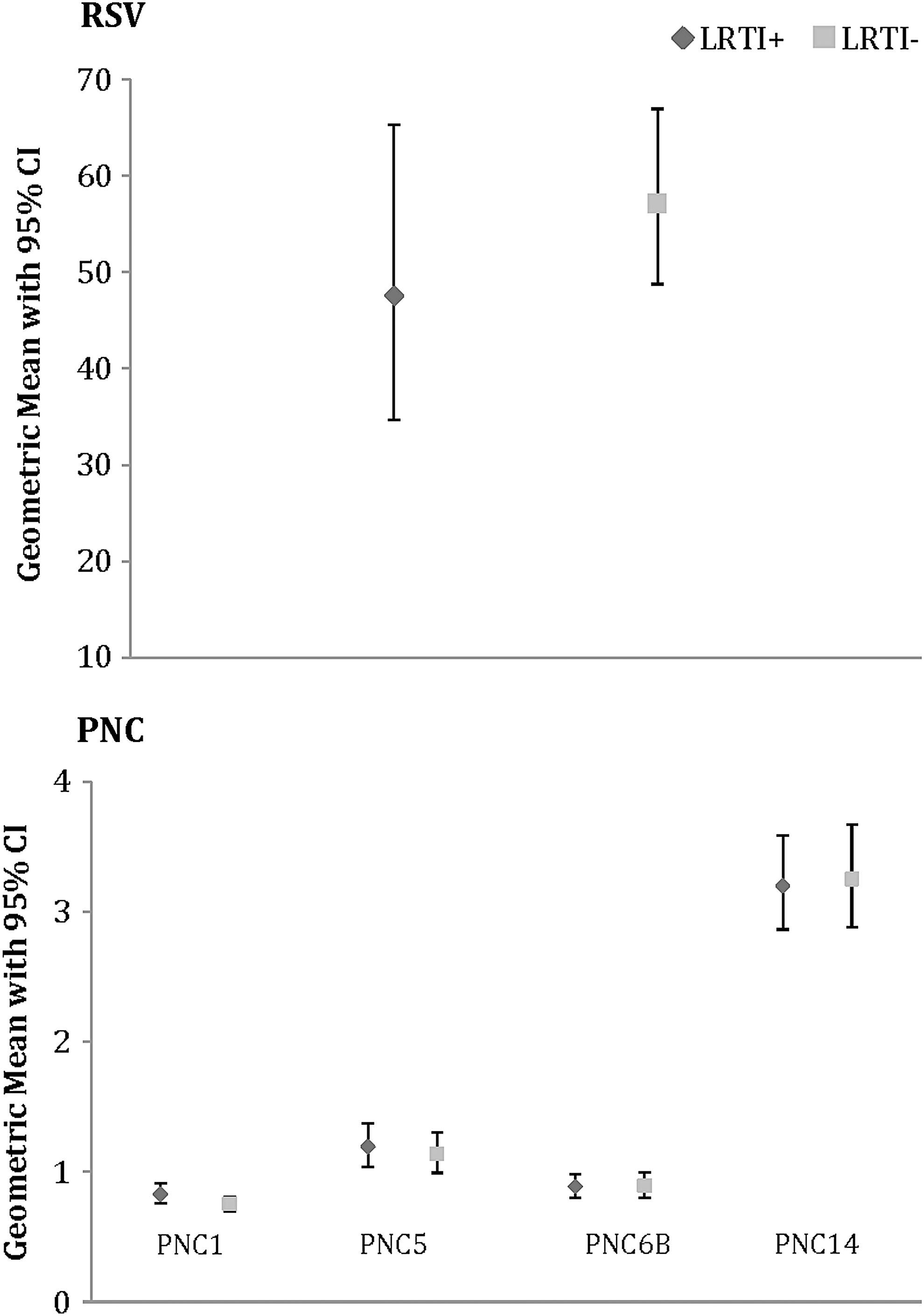
Infections with respiratory viruses and PNC in the first 6 months of life
The incidence of infections with specific pathogens in the first 6 months of life was measured by the incidence of seroconversions to each pathogen (Table 3). In addition to LRTI, seroconversion might have resulted from upper respiratory tract infections or asymptomatic infections. The rate of serconversions/infections did not show any differences between LRTI+ and LRTI− infants. However, the geometric mean antibody concentrations at 6 months of life were significantly higher for RSV and marginally higher for PIV1 in LRTI+ compared with LRTI− infants. There were no differences in antibody concentrations against the other respiratory pathogens.
Bolded p values indicate significant and marginal differences. To adjust for one-to-n matching, p values for antibody concentrations were calculated by linear mixed-effects models; p values for seroconversions were calculated by conditional logistic regression.
N, no. of children tested; Incidence, no. of children with seroconversion; %, no. of children with seroconversion/total no. of children.
To determine if there were any differences in the humoral immune competence of LRTI+ and LRTI− infants, we compared their antibody responses to the tetanus vaccine according to the number of doses received. Anti-tetanus toxoid antibody concentrations, stratified by the number of vaccine doses that each infant received, did not differ between the two groups (Table 4).
To adjust for one-to-n matching, p values were calculated by linear mixed-effects models; p values for the comparison of LRTI+ to LRTI− were determined combining no. of vaccine doses of 0 and 1 and also for combining 2 and 3 doses.
Discussion
In this study, LRTI+ and LRTI− HEUs had similar rates of seroconversions to common childhood respiratory viruses and PNC in the first 6 months of life. The corollary of this observation is that development of LRTIs is not due to increased exposure to respiratory pathogens in a segment of HEUs. Previous investigations showed that RSV and PNC were major causes of severe infection, hospitalization, and death in HEUs. 2,29 There are two important hypotheses that result from merging these observations: (1) HEUs have various degrees of immune deficiency that determine the severity of infections; and (2) environmental and socioeconomic factors differ between HEUs with and without severe infection and death. These hypotheses are not mutually exclusive, but it is important to determine their relative contributions to devise strategies to prevent adverse outcomes in HEUs.
The only socioeconomic difference between LRTI+ and LRTI− HEUs in this study was a lower number of completed years of education in mothers of LRTI+ infants. Maternal education is a strong predictor of socioeconomic and environmental factors that are associated with incidence, morbidity, and mortality of LRTI in low and middle-income countries. 30 –32 Although it is not clear if maternal education plays a direct or indirect role in LRTI mortality in low and middle-income countries, it appears to be a modifiable factor that could be included in the strategy to decrease infant mortality in these countries. 33
There were also differences in maternal HIV disease characteristics, including lower CD4+ cell counts and percentages and higher HIV plasma viral load in mothers of LRTI+ infants. Previous studies in HEUs have also shown that maternal immune status correlates with infant infectious morbidity. 14 As expected with their more advanced degree of HIV infection, mothers of LRTI+ infants tended to have lower RSV transplacental antibody transfer. However, the extent to which the transplacental transfer of maternal antibodies contributed to the risk of LRTI is uncertain, because LRTI+ and LRTI− infants had similar plasma levels of maternal antibodies at birth. There are other maternal factors associated with HIV infection that might have affected the development of infant immune competence, including transfer of immunosuppressive inflammatory or regulatory factors; transplacental passage of HIV subviral particles; and other congenital infections, such as CMV or syphilis, both of which may increase in pregnancies complicated by HIV infection. 34 –39
It is important to note that ARV utilization did not differ between LRTI+ and LRTI− HEUs or their mothers. ARVs have toxic effects on cellular metabolism and may affect immune responses. Zidovudine in particular was thought to be associated with anemia, neutropenia, lymphopenia, and other T cell abnormalities among HEUs compared with HUUs. 40 –43 Drugs in several ARV classes, such as nucleoside and non-nucleoside reverse transcriptase inhibitors, cross the placenta relatively well. 44 –47 Integrase inhibitors were not used by the mothers included in this analysis. Protease inhibitors are subject to a higher transplacental gradient than reverse transcriptase inhibitors, but reach measurable levels in the amniotic fluid and cord blood. 45,48 However, our data do not support the notion that specific ARVs contribute to the risk of LRTI in HEUs.
We analyzed infant and maternal use of cotrimoxazole. Cotrimoxazole is effective in preventing Pneumocystis jirovecii pneumonia and malaria in HIV-infected individuals. There is limited benefit from the use of cotrimoxazole in HEUs outside of malaria endemic areas, such as in our study. However, both maternal and infant use of cotrimoxazole may alter the microbiome and indirectly affect the development of the infant immune system. The use of cotrimoxazole did not differ between LRTI+ and LRTI− HEUs or their mothers, which precluded the assessment of its potential contribution to LRTI.
The main difference between LRTI+ and LRTI− HEUs were the anti-RSV and anti-PIV1 antibody concentrations at 6 months of age. The increased antibody concentrations against these viruses in LRTI+ HEUs suggest that viruses underwent more extensive replication in LRTI+ compared with LRTI− HEUs and the higher antigenic burden generated higher antibody production. The increased viral burden probably also played an important role in the development of LRTI.
Why did viruses replicate more extensively in LRTI+ infants? The most likely explanation is that immune defenses of LRTI+ HEUs were insufficient to contain viral replication. In this study, we found that humoral immunity did not differ between LRTI+ and LRTI− HEUs, suggesting that cellular immunity, adaptive and/or innate, may be the critical risk factors for severe infection in HEUs. Multiple studies have shown decreased cell-mediated immune responses to vaccines in HEUs compared with HUUs. 19,49 –51 In a previous study, we showed decreased natural killer cell function in HEUs compared with HUUs 52 and our unpublished observations also indicate defective antigen-presenting cell function and increased regulatory T cells in HEUs compared with HUUs. Any of these defects may increase the severity of viral infections in HEUs.
Our study has limitations due to its retrospective design. We made an effort to mitigate this problem by matching cases and controls by date of birth and geographic location to ensure that they had similar exposure to seasonal respiratory infectious agents. Additional strengths of our study included the collection of data by uniformly training abstractors, using standardized definitions and data collection instruments that were completed for predefined study visits.
Our findings significantly advance understanding of the factors that increase the risk of severe infection in HEUs by demonstrating that low maternal antibodies or defects in infant humoral immunity were not associated with HEU disease. This suggests that cell-mediated immunity of the HEU is likely to play a major role in their increased susceptibility to infections. We also showed that advanced maternal HIV disease was associated with increased risk of severe infection in the infant, but ARV or cotrimoxazole utilization were not.
Footnotes
Acknowledgments
The authors thank the participants, and the personnel at the NISDI Perinatal and LILAC research sites. NICHD NISDI Perinatal/LILAC Protocol: Principal investigators, co-principal investigators, study coordinators, data management center representatives, and NICHD staff include:
Funding
This work was supported by the Eunice Kennedy Shriver National Institute of Child Health and Human Development (NICHD) contracts N01-HD-3-3345 (2002–2007), HHSN267200800001C (2007–2012), and HHSN275201300003C (2012–2017). The findings and conclusions in this report are those of the authors and do not necessarily represent the views of the National Institutes of Health or the Department of Health and Human Services.