
Abstract
Perinatal HIV-infected (PHIV+) adolescents survive longer with the use of readily found combination antiretroviral therapy (cART); however, they still have the risk of developing cognitive deficits. The article aims to explore the brain functional changes in asymptomatic PHIV+ adolescents with cART based on the resting-state functional magnetic resonance imaging (rs-fMRI). rs-fMRI was performed on 20 PHIV+ adolescents and 28 PHIV− controls to evaluate the regional homogeneity (ReHo) in different brain regions by calculating the Kendall harmonious coefficient. Montreal cognitive assessment and laboratory studies (nadir CD4+ T cell counts) were also performed on all the subjects to evaluate their cognitive and immune status. Thirteen PHIV+ adolescents and 22 PHIV− controls were enrolled. There was a significant difference of ReHo values in PHIV+ adolescents compared to PHIV− controls, the areas with increased ReHo values include bilateral precentral/postcentral gyrus and right middle temporal pole. Also, the areas with decreased ReHo values locate in right putamen/pallidum/insula, left caudate/putamen/insula, right superior temporal pole/insula, right caudate/putamen, bilateral anterior cingulate cortex, and left inferior temporal pole. Furthermore, age, cognitive scores, and laboratory studies (nadir CD4+ T cell counts) did not show any significant correlation with altered ReHo values of brain regions neither in PHIV+ groups nor in PHIV− control groups. Among PHIV+ adolescents, brain areas with increased ReHo values were mainly located in the central somatic motor-sensory cortex, which might be related to the compensatory mechanism, whereas brain areas with decreased ReHo values were mainly focused on corticostriatal pathway, which might be associated with abnormal dopamine consumption. Thus, rs-fMRI could demonstrate the brain functional changes in resting state of asymptomatic PHIV+ adolescents.
Introduction
D
The use of cART can improve the cognitive function of HIV+ patients; nonetheless, viruses are not completely eliminated, so even with the stable cART, 20%–40% of patients suffer HIV-associated cognitive impairment (HAND). 3 Several studies have shown the changes of brain structure and function in PHIV+ adolescent patients. Sarma et al. 4 found that the volume atrophy of white matter (WM) was mainly in the bilateral posterior corpus callosum (consistent with HIV+ adult results), indicating WM injury in PHIV+ youth; the gray matter (GM) volume increased in the brain regions, including the left superior frontal gyrus, inferior occipital gyrus, gyrus rectus, right mid cingulum, parahippocampal gyrus, bilateral inferior temporal gyrus, and middle temporal gyrus, indicating neuronal cell swelling caused by brain HIV infection or toxicity from HIV treatment. There were also studies that found the GM and regional GM volume decreased in PHIV+ adolescents and adults. 5,6 As for the brain function, Herting et al. 7 found that in PHIV+ youth, there was an alteration in within- and between-Default Mode Network (DMN) connectivity, and the patterns of DMN connectivity were associated with the biological markers of disease severity (peak HIV-RNA and nadir CD4%), but the peak RNA and nadir CD4% had a different effect on brain function, which may suggest that the history of advanced immune impression and the virus infection have varying effects on brain function. So, this article aims to evaluate the brain functional changes of asymptomatic PHIV+ adolescents based on resting-state functional magnetic resonance imaging (rs-fMRI).
Materials and Methods
Participants
In this study, we recruited 20 PHIV+ adolescents receiving the cART confirmed from Hubei Province Center for Disease Control and Prevention in the study group, age between 12 and 18 years old. In the control group, 28 adolescents were included. All the subjects were enrolled from the summer camp held by AIDS Prevention and Treatment Center at Zhongnan Hospital of Wuhan University. Among them, PHIV+ group came from AIDS orphan family, one or both parents died due to HIV infection, and accompanied by vertical transmission of HIV, PHIV− control group also came from AIDS orphans family, one or both parents died due to HIV infection, but without HIV vertical transmission. This study is approved by the ethics committee of Zhongnan hospital, and all the subjects and their guardians have signed the informed consent. All the subjects were right-handed, and no other neurological or chronic diseases were diagnosed. The Montreal cognitive assessment (MoCA) confirmed no cognitive impairment in any of the subjects enrolled for the study.
MR techniques
All MRI examinations were performed using a 3-T MRI scanner (Simens Healthcare; TrioTim, Erlanger, Germany) with an eight-channel head coil. The scan baseline is parallel to the anterior and posterior commissures. All participants underwent rs-fMRI using a gradient echo, echo planar imaging sequence with the following parameters: Repetition time = 2000 ms, Echo time = 30 ms, Flip angle = 90°, Slices = 30, Slice thickness = 4.5 mm, Gap = 0 mm, and Resolution = 64 × 64, the scan lasted for 7.1 min and contained 210 volumes, and a T1-weighted MRI scan using a magnetization-prepared rapid gradient echo sequence, with the following parameters: Repetition time = 1900 ms, Echo time = 2.1 ms, Inversion time = 900 ms, TI = 900 ms, Flip angle = 9°, Slices = 176, Slice thickness = 1 mm, and Resolution = 256 × 256. All subjects lied flat on the scan bed with rubbers plugged ears to reduce noise while maintaining conscious, relaxed, and eyes closed.
Image processing
The rs-fMRI data were preprocessed by using the statistical parametric mapping software (SPM8,
We used regional homogeneity (ReHo) to characterize the temporally homogeneous functional brain areas at resting state, 10 which assumes that a given voxel was temporally similar to that of its neighbors; then, the ReHo value of a given voxel with those of its neighbors of the time series was measured by calculating Kendall harmonious coefficient (KCC), and the KCC value was the ReHo value of this voxel. ReHo analysis was conducted with the Resting-State fMRI Data Analysis Toolkit (REST). 11 For each voxel, ReHo was defined as the KCC of the time series of this voxel with its nearest 26 neighboring voxels. 10 Individual ReHo maps were generated by calculating KCC at each voxel within a mask without non-brain tissue, and for standardization purposes, the maps were divided by their own mean KCC within the mask. The WM and cerebro-spinal fluid (CSF) signals were regressed out to remove confounding artifacts. Then, the ReHo maps were smoothed using a Gaussian filter with a full width at half-maximum (FWHM) of 6 mm to reduce noise and residual difference in gyral anatomy.
Statistical analysis
SPSS for Windows (v.21.0; SPSS, Chicago, IL) was used for data analysis. Student's t tests were used for comparing the distributions of age, MoCA score, and duration of education between the PHIV+ and PHIV− groups, and chi-squared test was used for comparing gender between groups. To investigate the between-group ReHo differences across the brain between two groups, a voxel-wise two-sample two-tailed t test with age, gender, and duration of education as covariates was performed. Pearson's correlation coefficient was used for the evaluation of correlation between the altered ReHo of brain regions and the age, MoCA score, and nadir CD4+ T cell counts. Multiple comparisons were corrected by Monte Carlo simulation to calculate the probability of false positive detection by considering both probability thresholding and cluster size at each voxel. The following parameters were used: single voxel p = .05, cluster size = 23 voxels (621 mm3), FWHM = 6 mm, cluster connection radius r = 5 mm, mask = automated anatomical labeling template, and 5,000 simulations.
Results
Study population
We recruited 20 asymptomatic PHIV+ adolescents under cART as the study group and 28 PHIV− adolescents as the control group (Table 1). In the PHIV+ group, 7 patients were excluded from the study (one case had the head motion >2 mm, two cases were infected by blood transfusion, and four cases were not treated with cART), finally, 13 PHIV+ adolescents were included in our study (eight males and five females, mean age = 15.06 ± 1.61 years). Among PHIV− group, 7 patients were excluded (three cases had excessive head motion, one case had poor image quality and two cases were <12 years), then, the final study consisted of 22 control cases (10 males and 12 females, mean age = 15.41±1.5 years). There were no significant differences in age, sex, and educational attainment between the two groups; the nadir CD4+ T cell counts of PHIV+ group was 641.75 ± 291.67 cells/μL, only one patient has the nadir CD4+ count <200 cells/μL, which is 187 cells/μL; the average time of cART was 78.08 ± 34.72 months. There was no statistical difference in MoCA score between the two groups.
PHIV, perinatal HIV; NA, not available; cART, combination antiretroviral therapy; MoCA, Montreal Cognitive Assessment.
ReHo results between PHIV+ and PHIV− adolescents
Compared to PHIV− adolescents, PHIV+ adolescents' brain areas with increased ReHo values demonstrated significant difference in bilateral precentral/postcentral gyrus and right middle temporal pole regions, and brain areas with decreased ReHo values depicted significant difference in right putamen/pallidum/insula, left caudate/putamen/insula, right superior temporal pole/insula, right caudate/putamen, bilateral anterior cingulate cortex, and left inferior temporal pole regions (Tables 2 and 3; Fig. 1).

The yellow areas showed that the ReHo values increased significantly in the brain regions in PHIV+ group compared to the PHIV-group, including: bilateral precentral/postcentral gyrus and right middle temporal pole; the blue areas showed that the ReHo values decreased significantly in brain regions in the PHIV+ group, including: right putamen/pallidum/insula, left caudate/putamen/insula, right superior temporal pole/insula, right caudate/putamen, bilateral anterior cingulate cortex and the left inferior temporal pole (p < .05, corrected). PHIV, perinatal HIV; ReHo, regional homogeneity. Color images available online at
MNI, Montreal Neurological Institute.
p < .05, corrected.
ReHo, regional homogeneity.
Correlation between brain areas with altered ReHo values and age, cognitive state, and laboratory studies
In the PHIV+ group, there was no significant correlation between the altered ReHo values of brain regions and age. Figure 2 showed that there was a positive correlation trend between the ReHo values of postcentral-R and age; however, the correlation coefficient was <0.5 and p value was >.1. The MoCA scores and the nadir CD4+ T cell counts had no correlation with the altered ReHo values. In the PHIV− group, no correlation was found between the ReHo values and age, MoCA scores, and the nadir CD4+ T cell counts.
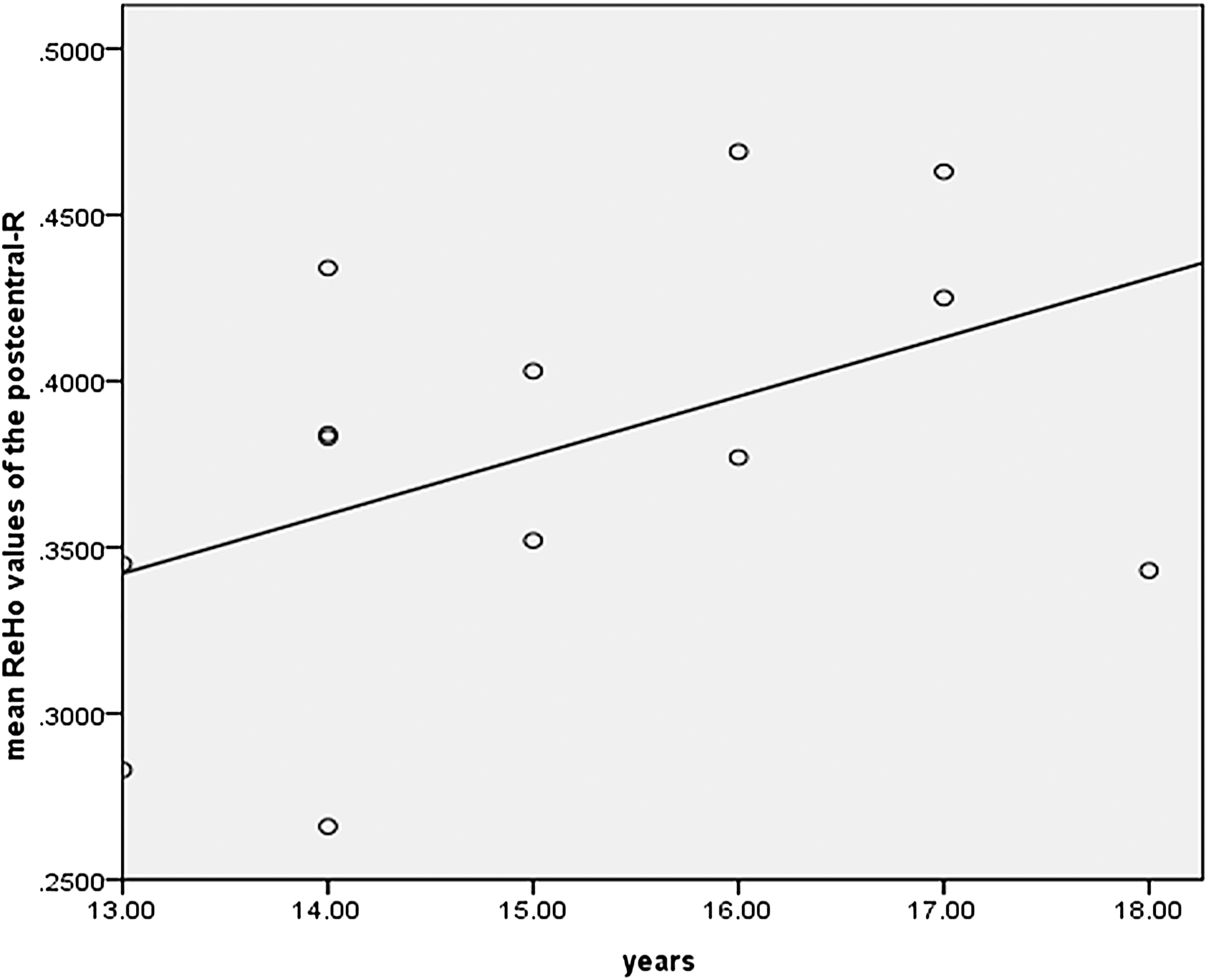
The linear correlation formula between the right postcentral gyrus and age is y = 0.111 + 0.018x, correlation coefficient R is 0.46, R 2 is 0.212, p = .114.
Discussion
This study demonstrates the brain functional changes in resting state of asymptomatic PHIV+ adolescents based on rs-fMRI. PHIV+ adolescents' ReHo values were significantly increased in bilateral precentral/postcentral gyrus and right middle temporal pole, and significantly decreased in right putamen/pallidum/insula, left caudate/putamen/insula, right superior temporal pole/insula, right caudate/putamen, bilateral anterior cingulate cortex, and left inferior temporal pole. Increased ReHo values of brain regions, mainly in the central somatic motor-sensory cortex, suggest that HIV infection can lead to brain damage; nonetheless, the nervous system has storage network, 12 which can achieve the same function by compensation from other brain regions. Another study on PHIV+ patients showed that the recombination within and between-DMN network (including the decrease of the connection within DMN network and the increase of connections with other networks) could improve the speed processing in HIV infected patients. 13 However, there was also a study that showed with the progress of the HIV infection, the ReHo of regions with motor function will decrease gradually causing motor impairment. 13 In this study, the ReHo values decreased in brain regions, mainly in bilateral striatum and some of the cortex. Langford et al. 14 found that HIV tends to invade striatum and WM fiber tracts between striatum and cortex, suggesting that the corticostriatal pathway is abnormal. Also, in functional connectivity studies, either based on the rs-fMRI 15,16 or the task-based fMRI, 17,18 the corticostriatal connectivity was reduced. The possible mechanism may be associated with the abnormal consumption of dopamine, including the decrease in the melanic neuron (the main site of the synthesis of dopamine) and the loss of the dopamine receptor (D2 receptor) region (putamen and caudate nucleus). 19,20
Previous studies on HIV+ adult patients found that age of the patient also played a role in brain function. Jewell B. Thomas 18 found that HIV infection and age, both resulted in reduced connectivity within the DMN and salience (SAL) network and between DMN and SAL networks, and the impact of HIV is bigger compared with the age factor; there were several studies showing that HIV infection and age have synergistic effects on brain function changes. 21 –23 However, in adolescents, the brain develops gradually and the changes of brain function should be positively correlated with age. Previous study 24 found that the blood oxygen level dependent (BOLD) signal in the DMN network was positively correlated with brain development during adolescence, and its BOLD signal gradually increased with age, but, in our study, we did not find such correlation between brain function development and age, which may be due to the HIV infection that hindered the normal brain development. Moreover, no correlation was found between the altered ReHo values of brain regions with MoCA score and laboratory test results (nadir CD4+ T cell count), which were similar to previous studies on HIV+ adult patients, 17,18 suggesting that the brain function changes may occur earlier than the changes of cognitive function.
As for the cART, traditional marker of HIV disease status may be affected, although HIV+ patients in nominal laboratory values and good virologic control may still experience neurologic dysfunction. Recent studies have shown that serological markers fluctuate throughout the course of disease and lose correlation with the severity of the disease. 25,26 Therefore, it is important to combine metrics such as rs-fMRI that is sensitive to early changes of the brain not detected by other typical tests used in evaluating HIV+ patients, providing HAND more accurate visual diagnostic biomarkers.
Now, there are still about 2.1 million (1.4–2.6 million) young people living with HIV in the world. 27 With the use of cART, HIV has become a manageable chronic disease, HIV+ patients survive longer, and the incidence of severe HAND is reduced, but for PHIV+ patients, due to HIV infection and cART neurotoxicity, mild HAND (minor neurocognitive disorder, MNI) is still very common. So in many previous studies, cART was thought to be a confounding factor that may affect the brain function related to HIV. Although a study of HIV+ adults found that the HIV+ group had lower corticostriatal connectivity than the HIV− group and the treatment of cART could improve the connectivity, 17 studies for school-age PHIV+ children found that early virus inhibition was associated with increased cognitive function. 28,29 However, for PHIV+ patients who need a lifetime of cART, the advantages and disadvantages of long-term cART still need further study to confirm.
Lifelong HIV infection has physiological and psychological effects on PHIV children. Vreeman et al. 30 found that PHIV infection and cART may have a potential impact on all important organs and systems, including metabolic disorders (hyperlipidemia and insulin resistance), bone abnormalities (fractures and osteoporosis), anemia, kidney failure, and reproductive health, it also includes psychological illness (mental and behavioral disorders) and so on. 31 So for PHIV+ adolescents, we should not only be concerned about the effects of the disease itself but also its secondary effects.
The important feature of this article is that the control group and PHIV+ group have the same social background and life experience, and similar exposure to educational degree, so the comparability is strong and the conclusion is credible. Unfortunately, the sample size is small because of special volunteers, and large samples are needed to further study.
In conclusion, the resting-state brain functional changes in the asymptomatic PHIV+ adolescents with cART, with increased ReHo of brain regions, are mainly located in the central somatic motor-sensory cortex, which may be related to the compensatory mechanism, whereas reduced ReHo of brain regions were mainly concentrated in the corticostriatal pathway, which may be associated with abnormal dopamine consumption. Thus, rs-fMRI could demonstrate the brain functional changes in resting state of asymptomatic PHIV+ adolescents.
Footnotes
Acknowledgments
The authors would like to thank Dr. Fuchun Lin and Dr. Hao Lei for help with the data analysis. This study was funded by Major Program of the National Natural Science Foundation of China (grant no. 81227902) and the National Key Basic Research Program National Natural Science Foundation of China (grant no. 2016YFC1304702).
Author Disclosure Statement
No competing financial interests exist.