
Abstract
Immunorecovery could be attenuated in HIV-hepatitis B virus (HBV) coinfection versus HIV monoinfection during antiretroviral therapy (ART), yet, whether it also occurs in individuals from sub-Saharan Africa without severe comorbidities is unknown. In this study, 808 HIV-infected patients in Côte d'Ivoire initiating continuous ART were included. Six-month CD4+ count trajectories and the proportion reaching CD4+ T cell counts >350/mm3, HIV-RNA <300 copies/mL, still alive and not lost to follow-up within 18 months (“optimal immunorecovery”) were compared between coinfected groups. At inclusion, 80 (9.9%) patients were HIV-HBV coinfected, 40 (50.0%) of whom had high HBV-DNA viral load (VL) (>104 copies/mL). Coinfected patients with high HBV-DNA replication initiated ART with significantly lower median CD4+ T cell counts [216/mm3, interquartile range (IQR) = 150–286] compared to coinfection with low HBV-DNA replication (268/mm3, IQR = 178–375) or HIV monoinfection (257/mm3, IQR = 194–329) (p = .003). These patients had significantly faster rates of CD4+ cell count increase from baseline after adjusting for baseline age, World Health Organization stage III/IV, and CD4+ cell counts (p = .04), yet, were not more likely to exhibit optimal immunorecovery (82.5% vs. 80.0% and 77.9%, respectively) (p = .8). In conclusion, change in CD4+ cell counts after ART-initiation was accelerated in coinfected patients with high HBV DNA VLs, but this did not lead to increased rates of optimal immunorecovery.
Introduction
W
One determinant of immune recovery that has received particular attention over the past decade has been coinfection with hepatitis B virus (HBV). Although much of the literature has observed no difference between HIV monoinfected and HIV-HBV coinfected patients in achieving undetectable HIV-RNA after ART-initiation, 10,11 there is some evidence that immunorecovery may be different. 12,13 For example, the Swiss HIV Cohort study recently observed significantly slower increases in CD4+ cell count among patients on-treatment with hepatitis B surface antigen (HBsAg)-positive or isolated hepatitis B core antigen positive serology than HBsAg-negative patients or those with resolved HBV infection. 14
In sub-Saharan Africa (SSA), some reports suggest differences in CD4+ cell count increase after ART-initiation between patients with or without HBV coinfection, 15 while others do not. 16 –18 Studies in these settings are generally confined to patients with severe immunocompromised status where average baseline CD4+ cell counts are <100 cells/mL, thereby altering the course of CD4 recovery. 1 Furthermore, most of these studies lacked information on HBV-DNA, making it difficult to establish the direct link between more active forms of HBV-infection and immunorecovery.
We used existing data from the Trivacan study, a large randomized control trial among treatment-naive HIV-infected patients from SSA without severe comorbidities, to evaluate the effect of HIV-HBV coinfection, including HBV-replication, on CD4 cell recovery during continuous ART. We also examined whether HIV-HBV coinfection was related to reaching specific levels of CD4+ cell count during therapy.
Materials and Methods
Study population
Patients participated in the ANRS 1269 Trivacan study, which was a prospective, randomized, open-label, multicenter trial in Abidjan, Côte d'Ivoire (
A total of 840 patients started ART at inclusion, receiving zidovudine and lamivudine (LAM) with either efavirenz or lopinavir/ritonavir. Patients underwent a 6- to 18-month phase of continuous ART during a prerandomization period, and those achieving CD4 > 350/mm3 and plasma HIV-1 RNA <300 copies/mL were randomized to a treatment strategy arm, as detailed elsewhere. 19,20 The analysis presented herein only includes the prerandomization period.
All participants gave written informed consent, and the study protocol was approved by the Ministry of Health of Côte d'Ivoire and the French National Agency for Research on AIDS and Viral Hepatitis (ANRS, Paris, France).
Assessing biological parameters
All patients were tested for HBsAg at study inclusion (Mini Vidas® assay; Biomerieux, Marcy l'Etoile, France), which was then confirmed using the Architect i2000 assay (Abbott Laboratories, Rungis, France). From samples stored at −80°C, hepatitis B “e” antigen (HBeAg) and anti-HBe antibodies were detected at study inclusion using the Elecsys assay (Roche Diagnostics, Meylan, France). HBV-DNA viral loads (VLs) were quantified at study inclusion using an in-house polymerase chain reaction (PCR)-based assay (detection threshold: 12 copies/mL). 21
Plasma alanine aminotransferase (ALT) and aspartate aminotransferase (AST) were collected at study inclusion, while only AST levels were available every 6 months during follow-up. Elevated transaminase levels were defined as an AST or ALT >40 IU/L.
CD4+ cell counts (True Count technique on FACScan, Becton Dickinson, Aalst-Enembobegem, Belgium) were obtained at study inclusion and every 3 months. Plasma HIV-1 RNA was quantified using real-time PCR and was measured at study inclusion every 6 months.
Statistical analyses
Patients were grouped as HIV monoinfected or HIV-HBV coinfected, the latter of which was further stratified on HBV-VL >104 copies/mL (“high HBV-DNA replication”) and HBV-VL ≤104 copies/mL (“low HBV-DNA replication”) at ART-initiation. The choice of threshold was determined from a previous study in SSA, demonstrating higher mortality rates when HBV DNA VLs were at or above these levels. 22 The clinical relevance of this threshold was confirmed in a previous study from the Trivacan study group. 23 Characteristics between groups were compared at study inclusion using Kruskal–Wallis test for continuous variables and Pearson's chi-squared or Fisher's exact test for categorical variables.
We modeled mean change in CD4+ T cell with mixed-effect linear regression models suppressing the fixed-effect intercept and including a random-intercept to account for patient variability at ART-initiation. To avoid bias due to differential loss to follow-up in patients achieving randomization criteria early, follow-up started at treatment initiation (defined as “baseline”) and included the first 6 months when all patients were not yet randomized. Fractional polynomial (FP) functions up to the second-order were compared by maximum likelihood ratio tests with the highest fitting model achieved as a second-order FP with continuous time and time transformed to the power of 2: FP[2, (1, 2)]. Multivariable adjustment was performed using independent covariables affecting CD4+ cell levels over time (Supplementary Table S1; Supplementary Data are available online at
We then used randomization as an end-point to indicate “optimal” immunorecovery during ART. Patients who were randomized (achieved CD4 > 350/mm3, plasma HIV-1 RNA <300 copies/mL within 18 months, still alive, not lost to follow-up, and absence of ≥1 criteria for nonrandomization) were compared with those who were nonrandomized. Univariable odds ratios (OR) and 95% confidence intervals (CIs) were estimated for baseline determinants using logistic regression models. A multivariable model was constructed by including all covariables with a p value <.1 from univariable analysis in a full model and removing variables above this threshold in backwards-stepwise manner. Coinfection group was forced in the model regardless of p value.
All analyses were conducted using STATA statistical package (v14.2, College Station, TX) and significance was determined using a p value <.05.
Results
Description of the study population
Of the 840 individuals enrolled in the Trivacan study between December 2002 and April 2004, 32 (3.8%) were not included in analysis due to the following reasons: did not have available HBsAg-status at inclusion (n = 1), did not have confirmed HBsAg-status (n = 25), or did not have available HBV-DNA at inclusion (n = 6). In total, 808 patients were included, of whom 728 were HIV monoinfected and 80 were HIV-HBV coinfected (40 with low and 40 with high HBV-DNA VL).
Table 1 provides a description of the study population at inclusion and compares infection groups. HIV-HBV coinfected versus HIV monoinfected patients were significantly more likely to be male and have elevated transaminase levels. Coinfected patients with high HBV-DNA VL, compared to all others, had significantly lower nadir CD4+ cell count (median = 198 vs. 240/mm3, respectively, p = .009), lower current CD4+ cell count (median = 215 vs. 257/mm3, respectively, p = .003), elevated transaminase levels (65.0% vs. 27.1%, respectively, p < .001), and higher ALT (median = 37 vs. 21 IU/L, respectively, p < .001) and AST levels (median = 46 vs. 30 IU/L, respectively, p < .001). Among coinfected patients, there were significantly higher proportions of HBeAg-positive serology (p < .001) and HBV-DNA levels (p < .001) in those with high versus low HBV-DNA VL.
Median (IQR).
n (%).
Significance between HIV-HBV coinfected and HIV monoinfected groups determined using Kruskal–Wallis test for continuous variables and Pearson's chi-squared test or Fisher's exact test for categorical variables.
Defined as ALT or AST >40 IU/L.
ALT, alanine aminotransferase; ART, antiretroviral therapy; AST, aspartate aminotransferase; BMI, body mass index; F, female; HBeAg, hepatitis B “e” antigen; HBV, hepatitis B virus; IQR; interquartile range; M, male; NS, not significant; NTP, no test performed; WHO, World Health Organization.
Change in CD4 cell count from ART-initiation and coinfection status
In this analysis, we included 795 patients with CD4+ cell counts at study inclusion and at least once during follow-up. Median change in CD4+ cell count from baseline increased at month 3 (+118/mm3; IQR = +53, +197) and at month 6 (+140/mm3; IQR = +54, +229). Median changes in CD4+ cell count stratified on HBV-infection group are depicted in Figure 1A, demonstrating rather large variability in individual trajectories. When applying the FP model to change in CD4+ cell count, there was no significant difference in rate of CD4 cell count increase between HBsAg-positive and HBsAg-negative patients (p = .3) after adjusting on baseline age, WHO stage III/IV, and baseline CD4+ cell count. However, as shown in Figure 1B, a significantly faster adjusted increase in CD4+ cell counts was observed among coinfected patients with high baseline HBV-DNA levels compared with HIV monoinfected patients (p = .04), but not compared to coinfected patients with low baseline HBV-DNA (p = .11).
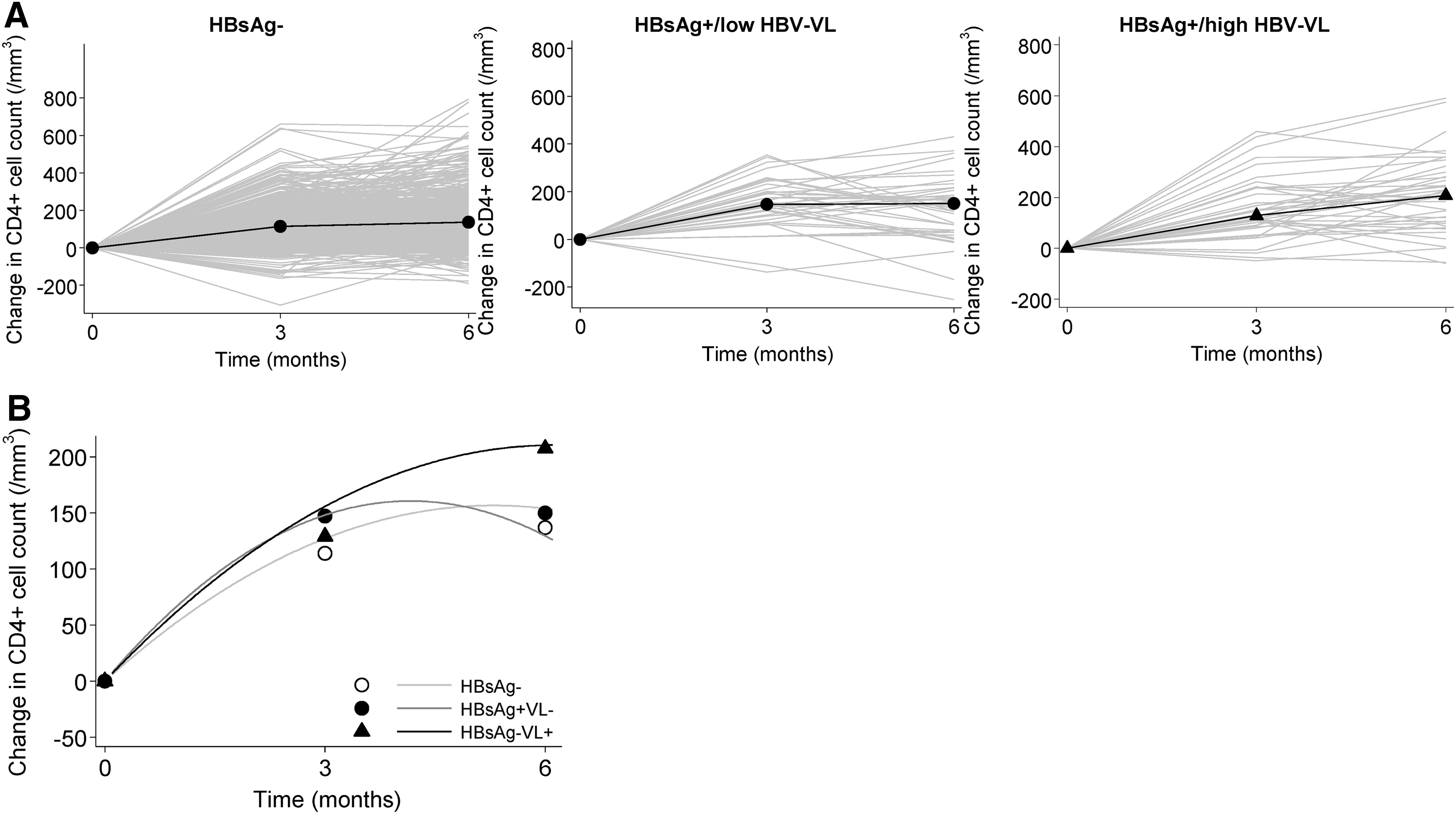
Immunological recovery after initiation of ART by HBV infection status. Individual changes in CD4+ T cell count (gray lines) and their unadjusted medians are given at ART-initiation, 3 and 6 months
Achieving randomization criteria and coinfection status
At the end of the 18-month prerandomization phase, 176 (21.8%) patients were not randomized and 632 (78.2%) were randomized. Reasons for nonrandomization include the following: death before 18 months (n = 20), lost to follow-up before 18 months (n = 22), CD4+ T cell count <350/mm3 (n = 95) and/or detectable HIV-1 RNA at last measurement (n = 28), and other (n = 29). No significant differences were observed between coinfection groups with respect to the CD4+ T cell count (p = .8) or HIV-1 RNA VL (p = .3) randomization criterion. As shown in the multivariable analysis presented in Table 2, the only factor significantly associated with randomization was higher baseline CD4+ T cell count. Of note, there were no significant differences in the odds of randomization between HIV monoinfected versus coinfected patients (p = .19), even when considering high or low baseline HBV-DNA at inclusion (p = .8 and p = .12, respectively). Similar observations were found when comparing HIV monoinfected versus coinfected patients with HBeAg-negative (adjusted OR = 1.26, 95% CI = 0.61–2.59) or HBeAg-positive serology (adjusted OR = 2.25, 95% CI = 0.73–6.91).
Randomization was defined as CD4 > 350/mm3 and plasma HIV-1 RNA <300 copies/mL by the end of 18 months of continuous antiretroviral therapy. Patients switching or permanently discontinuing treatment, lost to follow-up, or dead were considered as nonrandomized.
In the multivariable model, HBV coinfection group was forced. BMI and WHO clinical stage were removed because they no longer had an associated p value below the predefined threshold (p = .284 and p = .561, respectively).
“Low” and “high” VL defined as at or below 104 copies/mL and above 104 copies/mL, respectively.
CI, confidence interval; OR, odds ratio; VL, viral load.
Discussion
Using data from a large patient population in SSA, we demonstrate that HBV coinfected patients with high HBV DNA VLs initiated ART with significantly lower CD4+ T cell counts when compared with HIV monoinfection. During treatment, these patients had significantly faster increases of CD4+ cell change from baseline even after adjusting on well-known factors influencing CD4 levels. 25 Nevertheless, this significant increase did not affect the ability to achieve adequate reconstitution within 18 months of therapy, as largely deemed by having CD4+ cell counts >350/mm3 and HIV-1 RNA <300 copies/mL. We provide particular insight on the immunorecovery of ART-treated coinfected patients from Côte d'Ivoire, exhibiting a markedly improved initial immunological status compared to other studies from SSA. 16 –18
The significantly faster increase in CD4+ cell count among coinfected patients with high HBV DNA VLs was fairly surprising. Most research in this setting has indicated either comparable or decreased rates of CD4+ cell increases after initiating ART between co- and monoinfection. 14 –18 A variety of factors could explain the discrepancies between studies, such as age, gender, BMI, and tuberculosis infection. 3,7,26,27 Importantly, CD4+ T cell count at ART-initiation has been established as one of the more critical determinants of T cell recovery. 1 The fact that coinfected patients with high HBV DNA VL already started ART with much lower CD4 cell levels likely augmented their probability for accelerated immunorecovery compared with other infection groups; nevertheless, we did adjust for baseline CD4+ cell counts. Interestingly, individual trajectories of CD4+ cell counts revealed that stable or slightly decreasing levels during treatment rarely occurred in coinfected patients with high VL. This observation likely influenced the mean change from baseline in this group, lending to a significant association.
Considering that compensated and decompensated liver fibrosis has been linked to severe immunosuppression in HIV-HBV coinfected patients, 28 it is conceivable that liver fibrosis could impact CD4+ T cell trajectories during treatment. Accordingly, some evidence has pointed to reduced CD4+ T cell recovery with higher measures of transient elastography, 29 yet, the implications of HBV-infection from their analysis were unclear. Part of the reason for differences between the studies described above could then stem from the degree of liver fibrosis in coinfected populations. As patients with physician-assessed liver disease were excluded from our study, the prevalence of cirrhosis would be likely low, and hence, immunorecovery would be similar to noncirrhotic patients. Future studies with more specific data on liver fibrosis would help clarify the role of HBV-induced liver fibrosis on immunorecovery.
Suboptimal immunorecovery during ART has been recently exposed as a major problem in SSA, with 38% of HIV-infected patients unable to achieve CD4+ T cell counts >350/mm3 within 5 years after ART-initiation. 30 In our study, randomized patients were mostly reflective of those with “optimal” immunorecovery, whereas nonrandomized individuals constituted a group at-risk of incomplete immunorecovery. HBV-infection status, either at high or low levels of HBV-DNA replication, was not associated with being unable to reach randomization criteria (i.e., CD4 > 350/mm3, plasma HIV-1 RNA <300 copies/mL within 18 months, etc.). This finding would contend that other factors, namely age, gender, AIDS-defining illness at ART-initiation, and most relevant to our data, CD4+ T cell count, 27,30,31 are more predictive of continuously low CD4+ T cell count levels during follow-up.
There are certain limitations of our study that need to be addressed. First, follow-up was shorter compared to other studies in SSA. This forced us to use a different FP approach compared to previous models, possibly masking a plateau-effect of CD4+ T cell counts during later years of ART. 14 Coupled with the lack of follow-up HBV VL measurements, we were also unable to explore the interaction between HIV and HBV VLs. Second, we did not have data on other infections, such as hepatitis C virus, making it difficult to understand their role in immunorecovery. Third, this analysis concerned only antiretroviral agents that were available at the time of the Trivacan study. We cannot conclude whether treatment with newer agents evokes different rates of CD4+ T cell count. Fourth, the definition of suboptimal immunorecovery was not limited to only CD4+ cell count <350 mm3 but other randomization criteria (including death, loss to follow-up, ongoing severe HIV disease, ART regimen modification during the prerandomization phase, pregnancy, and ART regimen, including abacavir or nevirapine). As this represented roughly 40% of nonrandomized individuals, 20 their inclusion could have biased the direct effect of various determinants on immunorecovery. Nevertheless, many of these other criteria could be linked with insufficient immunorecovery, 1 thus reducing the effect of this bias. Finally, there were small groups of coinfected patients in this study, which may have reduced the power necessary to establish significant differences.
In summary, we found an accelerated increase in CD4 T cell recovery among HIV-HBV coinfected patients with high HBV DNA VLs at ART initiation, but this did not influence the probability of insufficient immune recovery. Our findings were likely related to the differences in degree of immunosuppression at ART-initiation between infection groups, the extent of HBV control during treatment, the shorter length of follow-up, or a combination thereof. Although these results are encouraging for coinfected patients, their long-term implications need to be evaluated. As more patients are expected to commence ART at higher CD4+ T cell counts with more effective agents, future research should explore if the lack in differences between HBV-infection groups is maintained in treated patients from SSA with mild immunosuppression.
Footnotes
Acknowledgments
We thank all patients who participated in the Trivacan trial. We also gratefully acknowledge the valuable contributions of the SMIT, CeDReS, CEPREF, USAC, CIRBA, CNTS, the Programme PACCI team, as well as INSERM exU593 and U897 teams. This work was supported by funds from the Agence Nationale de Recherche sur le Sida et les Hépatites (ANRS 1269/ANRS 12104 and ANRS 12240). A postdoctoral fellowship from the ANRS and SIDACTION was awarded to A.B. for some of the work presented in this article.
ANRS 1269 Trivacan study group: Investigators: Clinical care in Abidjan, Côte d'Ivoire–Service des Maladies Infectieuses et Tropicales (SMIT): Emmanuel Bissagnene (principal investigator), Serge Eholie, Auguste Kadio, Gustave Nzunetu, Cyprien Rabe, Aristophane Tanon. Centre Intégré de Recherches Biocliniques d'Abidjan (CIRBA): Olivier Ba-Gomis, Henri Chenal, Charles Diby, Denise Hawerlander. Centre National de Transfusion Sanguine (CNTS): Lambert Dohoun, Charlotte Huet, Seidou Konate, Albert Minga, Abo Yao. Unité de Soins Ambulatoires et de Conseil (USAC): Constance Kanga, Jonas Séri, Calixte Guéhi. Centre de Prise en Charge et de Formation (CePReF): Amani Anzian, Mamadou Diarrassouba, Nicole Dakoury-Dogbo, Joachim Gnokoro, Eugène Messou, Catherine Seyler, Siaka Toure.
Biology–Centre de Diagnostic et de Recherches sur le SIDA (CeDReS), CHU de Treichville, Abidjan, Côte d'Ivoire: Dominique Bonard (mycobacteriologist), Arlette Emieme (trial monitor), André Inwole (immunologist), Hervé Menan (parasitologist), Timothée Ouassa (bacteriologist), François Rouet (virologist), Thomas-d'Aquin Toni (virologist), Ramatou Toure (trial monitor). Service de Virologie, CHU Necker, Paris, France: Marie-Laure Chaix (virologist), Christine Rouzioux (virologist). Service de Pharmacologie Clinique, CHU Bichat Claude-Bernard, Paris, France: Gilles Peytavin (pharmacologist).
Trial coordination team: Abidjan, Côte d'Ivoire–Programme PACCI: Christine Danel (coordinator), Romuald Konan (trial pharmacist), Raoul Moh (trial monitor), Delphine Sauvageot (trial monitor), Souleymane Sorho (data manager). Bordeaux, France–INSERM U593: Xavier Anglaret (coordinator), Delphine Gabillard (trial statistician), Yves-Antoine Flori (economist), Roger Salamon (principal investigator).
Steering Committee: Françoise Barré-Sinoussi, François Boué, Geneviève Chêne, François Dabis, Pierre Marie Girard, Catherine Leport, Yves Souteyrand.
Independent Data Safety Monitoring Board: Dominique Costagliola (independent statistician), Jean-François Delfraissy, Nicolas Meda, Thérèse N'Dri-Yoman, Philippe van de Perre.
Representatives of the French Agence Nationale de Recherches sur le SIDA (ANRS, Paris, France): Brigitte Bazin, Séverine Blesson, Chantal Canon, Michel Kazatchkine.
ANRS 12240 VarBVA study group: Karine Lacombe, Raoul Moh (principal investigators), Mariama Abdou Chekaraou, Fabien Zoulim (study virologists), Anders Boyd, Delphine Gabillard (study statisticians), Christine Danel, Xavier Anglaret, Serge Paul Eholie, Sarah Maylin, Constance Delaugerre, Pierre-Marie Girard (coinvestigators).
Author Disclosure Statement
No competing financial interests exist.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.