
Abstract
We have estimated the prevalence of the different viral subtypes between January 2012 and December 2016 in HIV-1-infected patients of the Aquitaine region (southwest part of France) who had a routine HIV-1 genotype resistance testing (GRT) centralized at the Bordeaux University Hospital. GRT was performed on viral RNA (1,784 samples) before treatment initiation or at failure, whereas proviral DNA was used as template (1,420 samples) in the event of a treatment switch in patients with viral load below 50 copies/mL. Pol and integrase sequences were obtained; subtypes, circulating recombinant forms (CRFs), and unique recombinant forms (URFs) were assigned by combining the results of SCUEAL, REGA, COMET, and HIV BLAST. Globally, subtype B was predominant with 71.7%, whereas non-B subtypes accounted for 28.3%. Within the non-B viruses, CRF02_AG was the most prominent (11.6%) followed by non-B non-URF (13.5%), A, CRF01_AE, G, CRF06_cpx, F, C, D, H, J, and finally URF (3.2%). The analysis of the two compartments separately showed that RNA exhibits higher percentages of non-B viruses than DNA. This study reveals a high degree of diversity of HIV-1 non-B subtype strains in Aquitaine, with an increasing prevalence of CRF02_AG and URF in the population investigated for viral RNA, that is, including more recently detected HIV-1-infected patients. Future studies should attempt to identify the transmission clusters while paying special attention to URF, since they seem to be increasing in the population and could potentially host CRF.
Introduction
HIV
There are several reasons for studying the molecular epidemiology of HIV-1 circulating in different areas, but the main ones are to assess the dynamics of introduction and transmission of non-B viruses and to be able to identify any technical gaps in the commercial assays devoted to antibody–antigen detection and viral load quantitation.
In the present study, we analyzed our routine production of HIV-1 sequences, which is carried out for all hospitals in the Aquitaine region (now a part of “Nouvelle Aquitaine”) and including 3,204 different nonredundant patients from January 2012 to December 2016.
Materials and Methods
Patients
HIV pol and integrase sequences obtained between January 2012 and December 2016 were generated in the context of routine HIV-1 genotype resistance testing (GRT) of patients followed in Aquitaine, France (nine hospital centers: Saint André, Pellegrin, Haut-Leveque, Bayonne, Dax, Orthez, Arcachon, Libourne, Mont de Marsan). GRT was performed on viral RNA before treatment initiation or at failure, whereas proviral DNA was used as template in the event of a treatment switch in patients with viral load below 50 copies/ml. The global prevalence of the different viral subtypes and CRF was determined by removing duplicate sequences for a given patient.
Genotype resistance testing
GRT was performed from plasma viral RNA (1,784 samples) or proviral DNA (1,420 samples) according to the French ANRS procedures. Briefly, viral RNA was extracted by using the High Pure Viral RNA Kit (Roche). Five microliters were used for reverse transcription followed by a nested PCR. Proviral DNA was amplified by two successive PCR by using 5 μl of total DNA extracted on TECAN (Bio-Rad) from whole blood. Sequencing was done on ABI 3500xL and sequences were analyzed and stored in the SmartGene database (SmartGene, Lausanne, Switzerland).
Sequences
Nucleotide sequences of protease, reverse transcriptase, and integrase were extracted from the Smartgene database as FASTA files. For each gene, sequences were identified as patient ID_sample ID_date of analysis_template nature (RNA or DNA).
Subtyping
Subtypes were assigned using SCUEAL, 5 REGA 6 and COMET. 7 For a given gene, the subtype was directly assigned if the three analyses were concordant. In the event of discrepancy, sequences were submitted to BLAST to conclude. Unique Recombinant Form (URF) was concluded in the event of a difference between the subtyped genes.
Results
We retrieved a total of 3,204 GRT carried out between 2012 and 2016 in different contexts: before ART initiation in naive patients, at virologic failure, or before a switch of ART when no historical GRT was available. The global prevalence of the different HIV-1 subtypes was determined by removing duplicate sequences for a given patient. Therefore, we analyzed 2,409 sequences. The results are presented in Figure 1. Subtype B was predominant with 71.7%, whereas non-B subtypes accounted for 28.3%. Within the non-B viruses, CRF02_AG was the most prominent (11.6%) followed by non-B non-URF (13.5%), A, CRF01_AE, G, CRF06_cpx, F, C, D, H, J, and finally URF (3.2%). In our presentation in this study, the non-B non-URF denomination encompasses the HIV-1 group M subtypes and CRF described in the Los Alamos database, except for B and CRF02_AG.
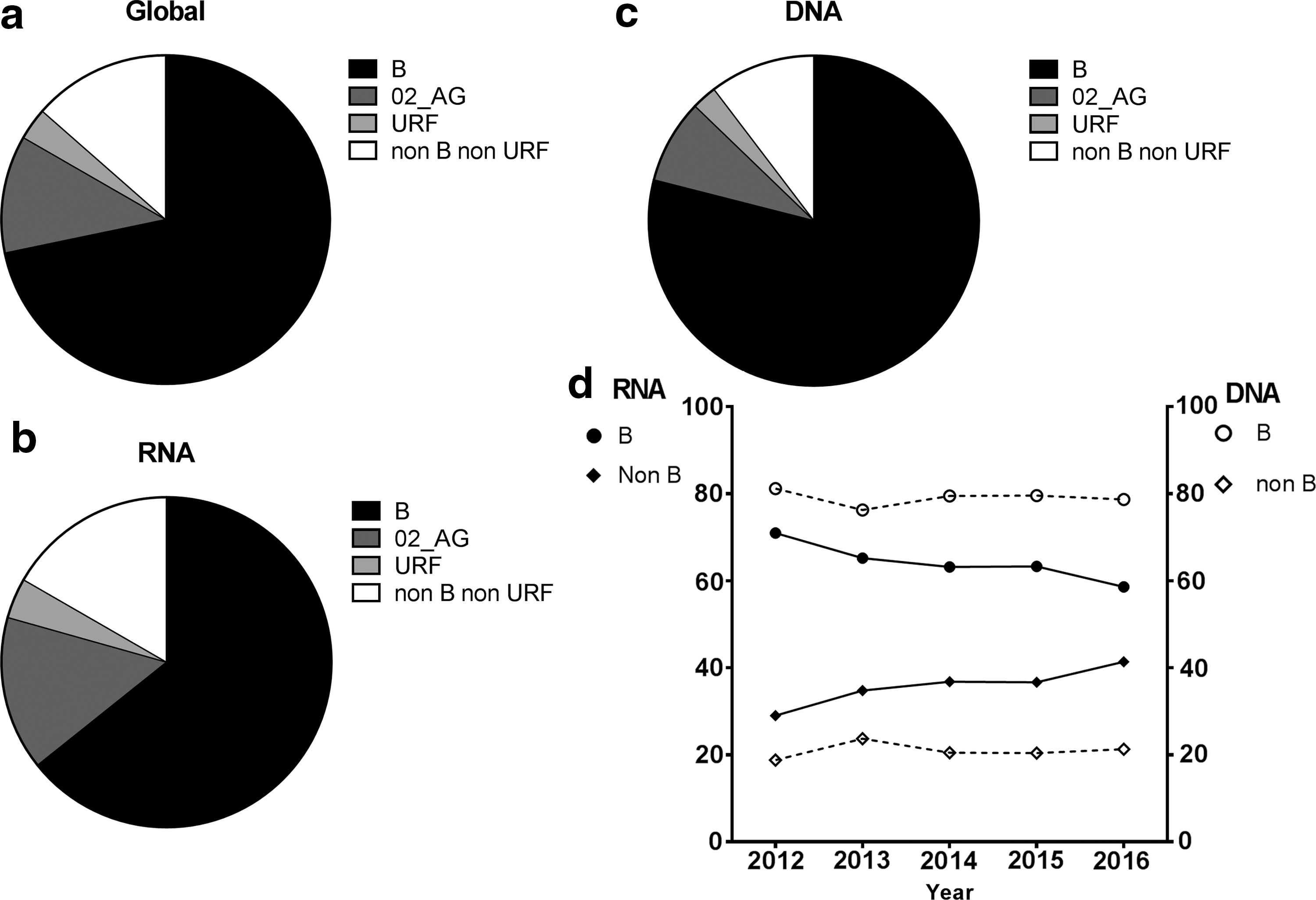
Distribution of HIV-1 subtypes and recombinants (B, CRF02_AG, URF, non B-non URF);
We then estimated the prevalence of the different subtypes according to the compartment analyzed (viral RNA or proviral DNA). They are presented in Figure 1b (RNA) and 1c (DNA). The percentage of subtype B HIV-1-infected patients who had a GRT from viral RNA is lower than from proviral DNA (64.3% vs. 79%), whereas we observed an opposite trend for CRF02_AG-infected patients (15% vs. 8.2%). URF viruses accounted for 4% of GRT from RNA and 2.4% from DNA, whereas non-B non-URF accounted for 16.7% and 10.4%, respectively.
The Figure 1d shows the evolution of the respective parts of B and non-B HIV-1 viruses between 2012 and 2016 according to the RNA and DNA compartments. There was a decrease of B subtype viruses genotyped from the RNA compartment, whereas the non-B viruses increased over time. Regarding the viruses identified by genotyped proviral DNA, the proportion of these two groups of HIV-1 subtypes remains constant with a higher prevalence of subtype B.
Discussion
These data are in accordance with data from other parts of Western Europe with a largely higher prevalence of subtype B versus non-B viruses. There is a high diversity within the non-B viruses as previously described, although CRF02_AG is the most common. France and especially the southwestern part of the country have long-standing relationships with the French-speaking countries of Sub-Saharan Africa and most of the non-B viruses have already been described in West and Central Africa. An increase in the prevalence of non-B viruses has been observed in France in the last 15 years as reported by national collaborative studies. 8,9 Although the prevalence of non-B viruses in Aquitaine seems lower than their global prevalence in France (∼30% vs. ∼45%), the amount of non-B viruses has increased in this area compared with the 16.4% prevalence described in recent seroconverters during the 1996–2006 period. 10
We have also differentiated the data from RNA and DNA compartments. GRT can be performed on proviral DNA when no previous sequence data are available, as mentioned by French recommendations. This gave us supplementary data for this epidemiological study, allowing us to evaluate more precisely the global distribution of HIV-1 subtypes and CRF in our area. With regard to putative circulating viruses, GRT performed with viral RNA is more informative since it includes newly diagnosed patients. The proportion of non-B viruses (mainly CRF02_AG) has been higher in the RNA compartment than in the DNA compartment since 2012. We hypothesize that recently detected HIV-positive patients who have been investigated for transmitted resistance before initiation of ART are at the origin of the increase in the amount of non-B viruses within this compartment, whereas DNA was investigated in patients who have received long-term treatment and whose therapeutic initiation was established at a moment when the percentage of B viruses was higher. Finally, future studies should attempt to identify the transmission clusters while paying special attention to URF, since they seem to be increasing in the population and could potentially host CRF.
Footnotes
Acknowledgments
The authors thank Ray Cooke for revising the article. This work is part of the Provir/Latitude 45 project funded by MSD Avenir (DS-2016-0005), GERMATAN and DRCI (Direction de la Recherche Clinique et de l'Innovation) at the University Hospital of Bordeaux. The different virologic and immunologic parameters of the patients are stored by the Unite de Surveillance Biologique (USB) at the University Hospital of Bordeaux under the terms of agreement 106897 of the Commission Nationale Informatique et Liberté (CNIL).
Author Disclosure Statement
No competing financial interests exist.