
Abstract
As oral tenofovir-based regimens for preexposure prophylaxis (PrEP) are adopted as standard of care for HIV prevention, their utilization in clinical trials among women in southern Africa will require an accurate estimate of oral PrEP efficacy in this population. This information is critical for women in choosing this prevention strategy, and in public health policy making. Estimates of the efficacy of oral PrEP regimens containing tenofovir have varied widely across trials that enrolled women, with some studies reporting high efficacy and others reporting no efficacy. Although poor adherence is strongly associated with lack of efficacy, other factors, such as mode of transmission (sexual vs. parenteral), predominant HIV subtype (C vs. non-C), intensity of exposure, and percentage of stable serodiscordant couples, may also contribute to the variation in efficacy estimates. In this article, we evaluate the evidence for PrEP efficacy in women and propose potential explanations for the observed differences in efficacy among studies. Our review emphasizes the need to continue to refine estimates of efficacy and effectiveness of tenofovir-based oral PrEP so as to best develop the next generation of HIV prevention tools, and to inform public policies directed toward HIV prevention.
Introduction
A
ARVs can also be used as oral or topical preexposure prophylaxis (PrEP); we focus in this study on oral PrEP. Studies on nonhuman primates have demonstrated partial to high efficacy of tenofovir disoproxil fumarate (TDF)-based oral PrEP regimens against simian immunodeficiency virus or simian/HIV acquisition. 15 –19 While an early study using TDF-FTC in men who have sex with men (MSM) showed only modest protection from HIV acquisition, 20 subsequent studies of TDF-containing regimens in MSM, 21,22 injection drug users (IDUs), 23 and men in serodiscordant partnerships 24 have demonstrated high efficacy, even with concomitant sexually transmitted infections (STIs). 25
However, evidence for oral PrEP efficacy in women at high risk of HIV acquisition has been mixed. Among the four efficacy trials that enrolled African women at risk of sexual acquisition, 24,26 –28 only the Partners PrEP study in serodiscordant couples found statistically significant PrEP efficacy for women (66% for TDF-FTC, 95% CI 28%–84%; 71% for TDF, 95% CI 37%–87%). The study of IDUs in Thailand also found significant efficacy in women (79%; 95% CI 17%–97%). 23 The reasons for the heterogeneity in efficacy for TDF-FTC as PrEP in women as compared with men are unclear, although measurements of ARVs in the blood have established differential adherence to daily pill taking as a major factor. 26 –29 More recently, pharmacological differences in vaginal versus rectal tissue concentration 30 –32 and the unique composition of the vaginal microbiome milieu 30,31,33 have emerged as additional potential explanations for the observed differences in efficacy between men and women.
The World Health Organization (WHO) reviewed the evidence on PrEP efficacy and recommended in 2015 that oral PrEP-containing TDF be considered not only for specific populations of MSM and serodiscordant couples, but also for all individuals at high risk of HIV infection, including women, where a 3% or higher annual incidence was used to define high risk. 34
For women at high risk in southern Africa, where the HIV incidence is 3% or higher in the general population, the WHO's guidance around the use of oral PrEP has created much discussion as to the role this medication should play in population-based approaches to HIV prevention. This discussion is hindered by gaps in our knowledge of the potential effects of factors beyond adherence, such as genetics, age, and subpopulation-specific differences in pharmacokinetics, tissue penetration, and target cell kinetics on the efficacy of oral PrEP. While oral PrEP is registered for use in many parts of southern Africa, its use on a population basis has not yet been pursued. In South Africa, oral PrEP uptake and adherence acceptance is being evaluated in demonstration projects among specific high-risk populations: MSM and commercial sex workers, 35 and more recently targeted programs primarily aimed at young women, aged 18–25. 36
In this context, discussions are taking place among community groups, regulators, ethicists, and researchers in many countries, and opinions vary as to the role PrEP should play in efficacy trials of other HIV prevention modalities. 37,38 Several efficacy trials evaluating HIV vaccines (HVTN 702 and 705), 39,40 monoclonal antibodies (HVTN 703/HPTN 081), 41 injectable PrEP (HPTN 084), 42 and contraception methods (ECHO) 43 are ongoing or recently underway. These trials are primarily recruiting young women in southern Africa, who bear the brunt of the HIV epidemic in this region, and who tend to be unmarried and to have multiple sexual partners, 44,45 and are sexually exposed to HIV in a subtype C epidemic. This is a population most similar to those enrolled in studies in which oral tenofovir-based PrEP has not been found to be effective, and in which adherence to PrEP has been low. 26 –28 Annual HIV incidence rates in this population have ranged from 4% to 10%. 46
Obtaining a reliable estimate of the efficacy of oral PrEP for women in southern Africa is important to HIV prevention research and to developing PrEP as part of the standard of HIV prevention. Knowledge of the magnitude of PrEP efficacy is needed to ensure that trials are large enough to accommodate the decreased rate of HIV infections attributable to PrEP, to optimize participant and community education and counseling around PrEP, and to facilitate research on the impact of oral PrEP in these populations.
Given the biological complexity and behavioral challenges associated with the use of oral PrEP, we review the available evidence of PrEP efficacy in women. As stated in the primary publication for the Partners PrEP trial, 24 “Biologic and behavioral hypotheses have been proposed to explain the failure of two trials of PrEP among African women to show protection against HIV-1 infection, 23,24 including a lack of adherence to daily doses of PrEP, vaginal concentrations of tenofovir achieved with oral dosing that may be particularly sensitive to nonadherence, 25 STIs or other cofactors affecting infection with HIV-1 in young women, high HIV-1 concentrations in the seropositive partner during primary HIV-1 infection, and innate or acquired immunologic factors that may provide adjunctive protection in long-term couples with HIV-1 serodiscordance.” We discuss these and other potential explanations for the observed differences in efficacy among studies. We argue that, while the available data suggest that PrEP is effective in women, the wide variation in efficacy estimates makes it difficult to quantify the level of efficacy, and call for continued data collection to inform on the level of PrEP efficacy in southern African women.
What has been Learned About PrEP in Women from Efficacy Trials?
The clinical effects of PrEP can be viewed as lying along a spectrum. At one extreme is the pure biological efficacy of PrEP, which captures only PrEP's direct biological effect on preventing HIV acquisition; and at the other extreme is the program effectiveness of PrEP, which includes both direct and indirect effects 47,48 as well as biological and behavioral effects, such as imperfect adherence and potential risk compensation. 49 Our focus is on summarizing the PrEP effect estimated in a blinded and placebo-controlled trial. Recognizing that terminology varies in field, we refer to this as PrEP efficacy, which does not reflect pure biological efficacy and is far shy of program effectiveness.
Five oral PrEP efficacy trials to date have enrolled women: TDF2, 27 Partners PrEP, 24 Bangkok-TDF, 23 FEM-PrEP, 28 and VOICE 26 (Table 1). Three of the studies (FEM-PrEP, VOICE, and TDF2) were conducted in regions with subtype C epidemics, one among discordant couples in East Africa (subtypes A and D), and one among IDUs in Thailand (subtype A/E). None of the studies conducted in subtype C regions found statistically significant efficacy in women overall of any oral PrEP regimen—either individually or collectively. The two largest studies, FEM-PrEP and VOICE, conducted exclusively in women, found no trend toward efficacy of oral PrEP. While the TDF2 study in men and women in Botswana was not powered to evaluate efficacy in women alone, it found a nonstatistically significant trend for efficacy of TDF-FTC among 557 women (49% efficacy; 95% CI −22% to 81%, p = .11); seven of the nine participants who became HIV infected despite the receipt of TDF-FTC were women. 27 The overall efficacy (men and women combined) was 62% (95% CI 22%–83%, p = .03) and efficacy in men was 80% (95% CI 25%–97%, p = .03). However, challenges have been raised regarding interpretation of the TDF2 data 50 and the TDF2 adherence data pertained to the as-treated cohort—participants who reported having used medication within the last 30 days. 27 We estimate considerably lower adherence for the modified intention-to-treat (MITT) cohort, which was the basis for adherence analyses in other PrEP trials: (64% of TDF2 MITT participants vs. 81% of as-treated participants had detectable drug; Table 1 and Appendix 1).
Data are shown for the MITT cohorts (the set of enrolled participants, excluding those who were retrospectively found to have been HIV infected at enrollment) of each study. Details on the adherence and HIV subtype data are included in Appendix 1.
For TDF2, number of women by arm are in the randomized population; two placebo recipients and one TDF-FTC recipient were found to be HIV infected at enrollment, but gender was unknown. Incidence is approximated assuming equal follow-up in men and women and by arm. Drug level testing results are for the active arm at large (men and women) and average duration of follow-up is for all participants in the MITT cohort (men and women). Pregnancy incidence is calculated as the number of pregnancies divided by total person-years of follow-up among women.
For Bangkok-TDF, number of women by arm are in the randomized population; two placebo recipients were found to be HIV infected at enrollment, but gender was unknown. Drug level testing results are for the active arm at large (men and women). To our knowledge, pregnancy data have not been published.
MITT, modified intention to treat; PrEP, preexposure prophylaxis.
Partners PrEP, which demonstrated high efficacy of oral PrEP among women, enrolled HIV-serodiscordant couples from Kenya and Uganda. 24 Both TDF and TDF-FTC were found to reduce HIV acquisition among 1,780 female HIV-negative partners. 24,51 In the Bangkok-TDF study among IDUs, TDF had just a statistically significant, estimated efficacy in women. 23 Since all evidence points to parenteral transmission in the Bangkok-TDF study, 23 its relevance to sexually acquired HIV is unclear and we focus further discussion on the studies with sexual transmission.
Variation in adherence to oral PrEP is the leading explanation for the differences in efficacy across trials (Fig. 1). This variation in adherence may be attributable to the conduct of the trials and/or to characteristics of the trial participants themselves. 26,29 Poor adherence, as measured by lack of detection of drug in plasma, was above 65% in VOICE and FEM-PrEP, which found no efficacy, and below 25% in Partners PrEP and Bangkok-TDF, which found high efficacy.

Characteristics of the populations of women enrolled in PrEP efficacy trials with sexual HIV transmission. Varying adherence is the leading explanation for different efficacy results across trials, but the role of adherence cannot be studied in isolation: adherence is confounded with circulating HIV subtypes, placebo group incidence, and whether HIV serodiscordant partners or individual women at risk were recruited. For each trial the estimated PrEP versus placebo HR is reported. Details on the adherence and HIV subtype data are included in Appendix 1. HR, hazard ratio; PrEP, preexposure prophylaxis.
While adherence is clearly an important factor, the circulating HIV subtypes in the populations and the type of potential sexual exposure also differed markedly between the trials and may also modify efficacy. TDF2, VOICE, and FEM-PrEP recruited individual women at high risk of HIV, whose acquisition was more likely from persons with unknown HIV status and unknown duration of HIV infection, and who may have recently initiated sexual contact. High viral load—as in patients with acute HIV infection—is associated with increased transmission risk. 52 –54 In contrast, Partners PrEP recruited serodiscordant partners, where the HIV-positive partner was not on antiretroviral therapy (ART) at enrollment. 24 These serodiscordant couples were long-term sexual partners (median duration of cohabitation, 7 years 24 ), and the placebo group incidence rate was about half of what was seen in the trials, in which community-based acquisition was the major mode of acquisition (Table 1).
Moreover, HIV-1 subtype C infections are predominant (>67% of HIV sequences) in the populations where FEM-PrEP, VOICE, and TDF2 were conducted, and rare in eastern Africa where Partners PrEP was conducted. Therefore, it is not possible, given these data alone, to determine whether factors other than adherence—HIV subtype, level of HIV exposure, or recruitment of serodiscordant partners—explain some part of the observed differences in efficacy across trials; these factors are intrinsically linked, or confounded, with one another.
Three meta-analyses have synthesized data on PrEP efficacy, but the above differences in trial populations have not been systematically considered. 55 –57 The Cochrane Review 55 has limited value for informing on efficacy in women because only Partners PrEP and TDF2 were included; VOICE, FEM-PrEP, and Bangkok-TDF data were not yet available. Fonner et al. 57 combined data from all PrEP efficacy trials—in men and women and in different at-risk populations. Not finding statistically significant evidence of effect modification, they concluded that gender does not modify PrEP efficacy and reported an overall efficacy estimate of 51% (95% CI 27%–67%). However, the lack of a significant interaction is not sufficient for concluding absence of effect modification, given the low power of the test to detect moderate but clinically meaningful differences in efficacy. 58 Hanscom et al. 56 considered data on women only, and found strikingly different results depending on whether the Partners PrEP data were included: the estimated PrEP versus Placebo relative risk for women based on VOICE, FEM-PrEP, and TDF2 was 1.05 (95% CI 0.78–1.71); adding Partners PrEP data changed this to 0.70 (95% CI 0.42–1.18). These results suggest that the other differences highlighted between trial populations deserve further exploration.
In the sections that follow, we examine each of the key differences in turn between populations of women enrolled in PrEP efficacy trials: circulating HIV subtype, intensity of HIV exposure, recruitment of serodiscordant couples versus individual women at risk of community-acquired HIV, and adherence to oral PrEP. We focus on the potential for these factors to explain some part of the observed differences in efficacy in women across trials.
Evidence of PrEP Efficacy Against Sexual Exposure to Subtype C HIV
Given the lack of efficacy of PrEP based on the combined data of the three studies among women in predominantly subtype C settings (TDF2, VOICE, and FEM-PrEP), 56 in contrast to the high PrEP efficacy among women in Partners PrEP, it is of interest to evaluate efficacy against subtype C infections in Partners PrEP; however too few subtype C HIV-1 infections occurred during the trial to permit this analysis. 59 There are data suggesting that HIV subtype may influence sexual HIV transmissibility. 60 –65 Studies of heterosexual couples have reported that subtype E (CRF01_AE) viruses may be more sexually transmissible than subtype B viruses 63 and that subtype A viruses are significantly more sexually transmissible than subtype D viruses. 60 The factors underlying these variations in transmissibility by subtype are uncertain. There may be unique virological characteristics of different subtypes, for example, as yet unidentified polymorphisms associated with HIV replication, or greater rates of certain types of genital tract inflammation. It is also possible that sexual exposure to acutely infected partners occurs more frequently in certain countries. Regarding subtype C, ex vivo studies have shown that subtype C HIV isolates have higher transmission fitness compared to other group M isolates 61 and higher transmission efficiency across the cervical mucosa compared to subtype A isolates, 62 although Kahle et al. did not report a difference in sexual transmissibility in subtype C versus non-subtype C viruses. 66 Given that much of the work comparing sexual transmissibility of different HIV subtypes has been conducted among serodiscordant couples, who differ from the general population in multiple respects as discussed below, it remains an open question whether there are differences in sexual transmissibility of subtype C versus non-subtype C viruses in the general population.
PrEP Efficacy and Intensity of Sexual Exposure
PrEP efficacy in women may depend on the intensity of exposure to HIV, particularly under poor adherence. 67 Higher viral loads in the blood 52,68 and higher levels of genital HIV RNA 69,70 in the exposing partner predict higher sexual transmission risk, raising the question of whether the level of exposure to HIV modifies the efficacy of PrEP for preventing HIV transmission.
There is a strong correlation across trials in women between PrEP efficacy and placebo group incidence—a marker of level of HIV exposure (Fig. 2A). Notably, the incidence–efficacy association is nearly as strong as the association between adherence and efficacy (Fig. 2B). However, study-level meta-analyses are challenging to interpret due to many other differences between trials and trial populations that covary with placebo group incidence (Fig. 1). Thus, one cannot conclude from these analyses alone that high HIV exposure causes low PrEP efficacy.
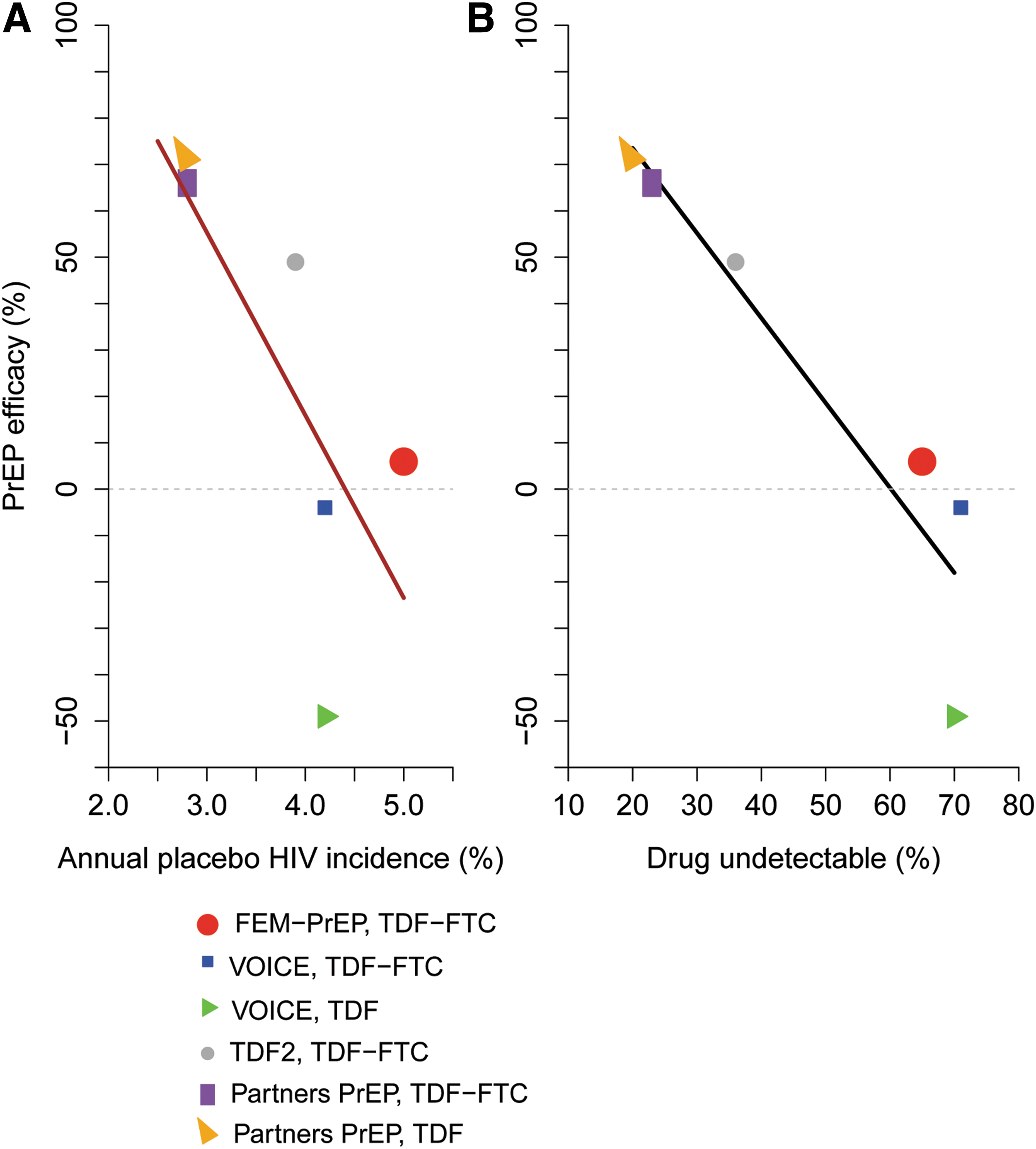
Correlation between PrEP efficacy estimates in women and placebo group HIV incidence
The question of whether PrEP efficacy in women varies with level of HIV exposure has been examined using data from the Partners PrEP study. In prespecified subgroup analyses, estimates of PrEP efficacy in various high-risk/high-exposure baseline subgroups are as high, or even higher, than estimates of PrEP efficacy overall, and statistical significance is retained. 24,51 Murnane et al. 51 found 64%–80% PrEP efficacy (p < .05) in subgroups of women defined based on high partner baseline viral load (viral load above 50,000 copies/mL), young age (under age 30), or high HIV risk score. 71 Estimated placebo group HIV incidence in these female subgroups ranged from 5.4% to 6.6% annually, much higher than the 2.8% incidence in women at large, and adherence was uniformly high (>70% had drug detected in all subgroups). Importantly, these analyses are not subject to confounding; within each subgroup defined by baseline characteristics, PrEP and placebo groups are comparable due to blinding and randomization. Their limitation is that how PrEP efficacy varies as a function of the partner's continuous viral load has not been described, nor has efficacy as a function of the partner's viral load proximal to infection. Moreover, it is difficult to bridge the results to other populations of women, as discussed below.
It is difficult to examine whether PrEP efficacy varies with level of HIV exposure in the other PrEP efficacy trials that enrolled individual at-risk women, since there are limited data available on the exposing partners. Furthermore, it is challenging to interpret subgroup analyses in trials with lack of efficacy overall. 58
Evidence of PrEP Efficacy Against Sexual Exposure Outside Stable Serodiscordant Partnerships
VOICE, FEM-PrEP, and TDF2 directly assessed the efficacy of PrEP among women not selected on the basis of being in HIV serodiscordant partnerships and an analysis of the pooled data failed to find evidence of PrEP efficacy. 56 While the Partners PrEP trial enrolled serodiscordant partners and estimated 66%–71% efficacy, 24 intriguingly, genetic analyses showed about 25% of HIV infections in the study were unlinked to the HIV-positive partner (Jared Baeten, personal communication). This rate is similar to those in earlier serodiscordant couple studies (36% in HPTN 0529 and 29% in the Partners in Prevention HSV/HIV Transmission Study 72 ). Therefore, the Partners PrEP study could potentially provide evidence of PrEP efficacy among women outside stable serodiscordant partnerships, although with limited precision.
The level of sexual exposure to HIV may differ for individuals exposed in the context of a serodiscordant partnership, compared with those exposed in a generalized HIV epidemic. 67,73 Lower placebo group HIV incidence was seen among women in Partners PrEP (Table 1) and was also noted in earlier trials in HIV serodiscordant partners (e.g., Refs. 72,74 ), as well as in HIV serodiscordant couple studies, where the HIV-infected partner was also HSV-2 seropositive. 72 The consistency of this finding is intriguing, since one of the partners in each serodiscordant couple is known to be HIV infected, whereas the majority of sexual partners of participants in an individually randomized study would be expected to be HIV negative, even in high-incidence populations. These data suggest that the HIV-positive partner in couple studies transmits infection at a lower rate than in other settings.
The source partner's viral load is one possible explanation. There are likely differences in the exposure of viral load between source partners in serodiscordant couple studies versus in the general population of HIV-infected subjects: Serodiscordant couple studies generally require that HIV-infected partners are not on ART or ART eligible at enrollment. In Partners PrEP, 24% of HIV-positive partners had a viral load below 2,000 copies/mL at enrollment, 75 similar to other serodiscordant couple studies. 9,66,76 Surreptitious ART use has been noted in previous serodiscordant couple studies, but explains only a fraction (22%–33%) of the low viral loads. 66,77 Accordingly, the low viral load more likely reflects the selection of long-term sexual partners who have not transmitted HIV and who therefore may be less infectious. 78
Importantly, HIV-positive partners in serodiscordant couple studies generally have chronic HIV infection, and thus have lower viral loads in the blood and genital tract (and lower risk of HIV transmission) 78 –80 compared with acutely infected individuals. 81 –83 Other host characteristics of the HIV-infected partner or of the infecting virus may also partially explain the lower HIV incidence in this population. Genital tract inflammation and the vaginal/rectal microbiome (which may influence acquisition) may differ between long-term sexual partners and those with recent onset of sexual partnership or in settings where multiple partnerships are the norm.
Risk behavior may also differ in the serodiscordant couples' context. The couples' counseling that was implemented in Partners PrEP 24 and other serodiscordant couple studies, in contrast with the individual risk-reduction counseling in other PrEP trials, may have increased condom usage or otherwise reduced the HIV-negative partner's exposure to HIV. 84 –87
The HIV-negative individual in a serodiscordant partnership is also unique: This exposed uninfected population is well studied and some potential mechanisms mediating their protection from HIV infection have been identified. 88 –92 Women in serodiscordant couple studies also tend to differ demographically from women in the general population. An estimated 98% of couples in Partners PrEP were married, with many years of cohabitation, 24,93 indicating long-term exposure to HIV and relatively inefficient transmission. Women in Partners PrEP were older: about 45% of HIV-negative partners were older than 35. In contrast, in VOICE for example, the majority of women was younger than 25 and unmarried or not cohabitating, and was likely to have a STI, 26 which suggests an increased risk of encountering a partner with unknown HIV status; 18.8% of adults 15–49 years of age in South Africa are HIV positive. 94
Importantly, knowledge of the HIV status of the sexual partner is likely to play a large role in the adherence to HIV prevention intervention, as evidenced by the high adherence among women in Partners PrEP as compared with other trials in women (Table 1). 95,96 Women not selected on the basis of being in serodiscordant partnerships may not be aware of their partners' HIV status. For example, of 2,746 women enrolled to VOICE at South African sites, 61% reported not knowing at baseline if their partner had other sexual partners (Gita Ramjee, personal communication; knowledge of the HIV status of the partner was not ascertained).
These attributes of HIV-negative and HIV-positive subjects enrolled in serodiscordant couple studies are likely to affect the HIV-negative partner's risk of HIV acquisition. It is unclear whether they modify the efficacy of PrEP. The one exception is adherence, which has been strongly linked with PrEP efficacy as we discuss next.
Dependence of PrEP Efficacy on Adherence
Differential adherence is the primary explanation for differences in PrEP efficacy among trials enrolling women, 26,28,97,98 and the role of adherence is difficult to underestimate. Study-level meta-analyses 55 –57 have found significant associations between PrEP efficacy and study-level adherence (Fig. 2B). At one extreme, in VOICE, 30% of TDF recipients and 29% of TDF-FTC recipients had tenofovir detected in plasma 26 ; in contrast, in Partners PrEP, 80% of female TDF recipients and 77% of female TDF-FTC recipients had detectable tenofovir, more than 80% of participants had drug levels consistent with daily pill taking, and pill count data suggested that study medication was used during 92.1% of the total follow-up time. 24 Hanscom et al. 56 estimated a PrEP relative risk for women of 1.19 (95% CI 0.89–1.61) under “low adherence,” compared with a relative risk of 0.39 (95% CI 0.25–0.60) under “high adherence.”
However, study-level meta-analyses have limited value for inferring PrEP efficacy in a new population, because PrEP adherence cannot be isolated as the cause of differences in efficacy. Other differences between trials and trial populations may explain some portion of the observed differences in efficacy. In particular, the meta-analyses have not considered potential differences in efficacy between serodiscordant partner studies and nonpartner studies.
Another approach to examining the impact of adherence is to assess how PrEP efficacy varies with adherence within individual trials, using causal inference methods. Murnane et al. 93 analyzed Partners PrEP with principal stratification and controlled effects methods, reporting that PrEP efficacy was higher in high adherers than in the trial population at-large. 93 However, these analyses rely on strong assumptions that cannot be empirically verified, even if the study is very large. 99 For example, the principal stratification approach relies on the assumption that the PrEP and placebo arms have the same risk of HIV, within subgroups defined by the level of potential adherence if assigned PrEP. 93 As such, they are generally seen as constituting a lower standard of evidence than traditional intention to treat analyses of a randomized and controlled trial.
The only adherence result that can be demonstrated within an efficacy trial without strong unverifiable assumptions is that adherence correlates with risk among PrEP recipients. Indeed, in Partners PrEP, PrEP recipients with high adherence were found to be at lower HIV risk than PrEP recipients with low adherence, even after adjustment for factors predicting both adherence and HIV infection (RR = 0.04, 95% CI 0–0.65). 29 However, the association between adherence and risk among PrEP recipients was not statistically significant or large in magnitude in the other trials that enrolled women, 26 –28 although this may be due in part to insufficient variability in adherence to establish the association.
Even if the mathematical relationship between PrEP efficacy and adherence is correctly estimated within Partners PrEP, or across trials based on study-level meta-analyses, it is still difficult to use this relationship as a basis for predicting how an increase in the level of adherence in southern African women would increase the level of PrEP efficacy. Such a prediction would rely on an unverifiable assumption that the mathematical relationship between PrEP efficacy and adherence would be the same in southern African women, that is, the “constancy” assumption. This assumption could fail due to key differences between PrEP efficacy trial populations, as discussed above.
A final issue in adherence-based analyses is uncertainty due to the partial sampling of participants for plasma drug testing; case–control and case–cohort designs have been used to select trial participants in whom adherence is assessed using stored specimens. In some studies, the uncertainty due to sampling is considerable given the small number of participants that were sampled for adherence assessment. For example, in FEM-PrEP study-level adherence was assessed using 95 randomly selected participants 28 and in TDF2 using 69 HIV-negative controls. 27 Study-level meta-analyses have treated the adherence estimates as fixed and known, whereas for some studies there is considerable uncertainty in the estimates. A second limitation of all reported adherence-based analyses is that they have not accounted for the error in the measure of adherence. Although validated, gold standard laboratory assays are used to quantitate plasma levels of drug, 100 all empirical measurements contain some level of uncertainty. To understand how true adherence modifies efficacy, an additional model would be needed to capture the error in the measured adherence variable.
Discussion and Conclusions
There is a large body of evidence demonstrating high efficacy of oral tenofovir-based PrEP in MSM, IDUs, and serodiscordant partners, 20 –24 with 44%–79% efficacy seen in blinded, placebo-controlled efficacy trials, and up to 97% effectiveness seen in some open-label studies and demonstration projects. 22,25,101 –103 However, evidence of oral PrEP efficacy in women in southern Africa is less conclusive; while the data suggest that PrEP prevents HIV infection, the magnitude of the efficacy is unclear. This uncertainty is attributable to considerable heterogeneity in efficacy estimates across trials in southern African women, and the difficulty in bridging efficacy results seen in other populations such as women in serodiscordant partnerships in eastern Africa, to women in the general population in southern Africa. Therefore, we recommend that additional data be collected to more precisely quantify PrEP efficacy in southern African women.
Pharmacological studies and simulations suggest some potential explanations for the observed differences in efficacy of oral PrEP in women as compared with men. For instance, after a single dose, tenofovir concentrations are lower in vaginal versus rectal tissue 30,31 ; with daily dosing, tenofovir concentrations peak later in vaginal versus rectal tissue 32 ; and when on-demand dosing is used, 104 tenofovir persists at high levels in rectal tissue many more days than in vaginal tissue. 105 Moreover, the concentrations of the nucleotide substrates of DNA synthesis with which tenofovir and emtricitabine metabolites compete for incorporation into HIV proviral DNA are significantly higher in vaginal versus rectal tissue. 32 Therefore, even if equivalent tenofovir/emtricitabine concentrations are achieved in vaginal and rectal tissue, tenofovir and emtricitabine may be less effective at inhibiting HIV reverse transcription in the former. 106 Finally, genetic variants have been identified that may negatively impact tenofovir activation in women and that may have different frequencies in men. 107
The need to collect additional data to quantify the efficacy of oral PrEP in women is supported by the accelerated approval processes used by multiple regulatory agencies, including the U.S. FDA. 108 Accelerated approval processes provide a relatively low bar for rapidly approving treatments that fill an unmet medical need for a particular population, based on a surrogate endpoint. Under FDA guidelines, the requirement is that there exists a surrogate endpoint that has not yet been validated, but has been demonstrated to be “reasonably likely” to predict real clinical benefit, and that a commitment is made to directly study the treatment's effect on the true clinical endpoint in the population in a Phase 4 postapproval study. In the PrEP context, the requirements would be that high adherence to oral PrEP is reasonably likely to predict sufficient overall prevention efficacy, and that rigorous Phase 4 studies are planned to document oral PrEP efficacy. Based on the above review, adherence has not yet been validated as a surrogate for bridging to the general population of women in southern Africa. However, the lower bar that adherence is “reasonably likely” to predict protection may have been met. Either way, accelerated approval processes would require that additional data be collected to confirm sufficient PrEP efficacy.
New data on the efficacy of oral PrEP among women in southern Africa will need to come from demonstration projects and observational studies; placebo-controlled trials of PrEP agents are no longer considered ethical. Given HIV endpoint data from demonstration projects or observational studies, statistical methods can be employed to estimate the causal effect of PrEP on HIV acquisition, using data on factors associated with HIV infection risk and with propensity to receive oral PrEP. 109 –112 Ideally, the data to be collected would be standardized across studies.
In addition, several ongoing trials should help inform on the level of PrEP efficacy. In HPTN 067, an open-label study of PrEP in young women (18–25 years of age) in Cape Town, South Africa, 4 HIV seroconversions have been observed among 178 women randomized to daily, time-driven, or event-driven dosing. 113 The CHAMPS PillsPlus study of daily PrEP in adolescents (15–19 years of age) in Cape Town and Soweto, South Africa has reported 1 HIV seroconversion among 99 women. 114 However, these studies are underpowered for formal efficacy assessments. HPTN 082 is a phase 4 study of adherence and acceptability of oral TDF-FTC in 600 women in southern Africa, which is designed to assess acceptability of and adherence to oral TDF-FTC under standard versus enhanced adherence support. HPTN 084 is a Phase 3 trial comparing oral TDF-FTC to injectable cabotegravir for HIV prevention in 3,600 women in southern Africa. Importantly, TDF-FTC usage is being monitored using stored specimens. Finally, the Gilead Phase 4 TDF-FTC Demonstration Projects will provide larger databases for estimating oral PrEP efficacy in southern African women.
The WHO's recommendation that TDF-based oral PrEP be considered for all populations at substantial risk of HIV acquisition 34 is based on a study-level meta-analysis that pooled data across men and women and across different at-risk populations, yielding an estimated PrEP efficacy of 51% (95% CI 27%–67%). 57 Given the considerations discussed above, we contend that the uncertainty in the level of efficacy of oral PrEP in southern African women should be better reflected; the considerable heterogeneity in efficacy results and the multiple behavioral, virological, and biological differences between populations suggest that the efficacy is difficult to quantify with the data available.
Given the importance of HIV prevention among women in Africa, it is not surprising that tenofovir-based oral PrEP has been embraced as a prevention tool. 34 However, the heterogeneity in efficacy results among women and difficulty bridging between populations requires us to keep refining estimates of efficacy, to best develop the next generation of HIV prevention tools and inform public health policies for HIV prevention.
Footnotes
Acknowledgment
This work was supported by the SDMC: HIV Vaccine Trials Network (award UM1AI068635 from the National Institute of Allergy and Infectious Diseases [NIAID] of the National Institute of Health [NIH] to P.B.G.).
Author Disclosure Statement
Dr. Cohen is on the Advisory Board for both Merck and Gilead, and has served on Merck and Gilead advisory boards. The other authors declare no conflicts of interest.
Appendix 1
*
There are two types of HIV, HIV-1 and HIV-2. The vast majority of HIV infections worldwide are HIV-1 and the main body of literature on ARVs and PrEP deals with HIV-1; thus, we use “HIV” throughout this article for simplicity.