
Abstract

E
A cross-sectional, descriptive, and retrospective study comprising 1,717 patients who were combination antiretroviral therapy naive, diagnosed with HIV, and attending at a health public center in southern Brazil between 2005 and 2016 was conducted. Sociodemographic information of the participants and possible risk factors for syphilis infection were collected by trained nurses and physicians, using a structured and pretested questionnaire. The samples were first analyzed by a nontreponemal test [rapid plasma reagin (RPR)] to diagnose syphilis. Reactive samples were then confirmed by treponemal test [enzyme-linked immunosorbent assay (ELISA)]. Only the reactive samples by both RPR and ELISA were considered positive for syphilis. Those who had an indeterminate diagnosis were retested. Other patients who did not meet the mentioned requirements were considered HIV monoinfected.
Approximately 71% (1,227) of the patients had syphilis serology data, with a mean seroprevalence of 15.9%. Of the total number of HIV–syphilis coinfected, 169 (86.7%) were male and 26 (13.3%) were female (p < .001), and the male-to-female ratio was 6.5:1; the mean ages were 28.7 ± 9.5 and 35.2 ± 12.7 years, respectively (p < .001). The prevalence of HIV–syphilis coinfection remained practically unchanged, with slight fluctuations between 2005 and 2011. However, there was a significant increase in the number of cases with HIV–syphilis coinfection from 2012 to 2016 (p < .001), which was more pronounced among male patients (Fig. 1). There was no statistically significant association between CD4+ T cell count (p = .075) and CD4:CD8 ratio (p = .728) when comparing the HIV-monoinfected and HIV–syphilis coinfected groups.
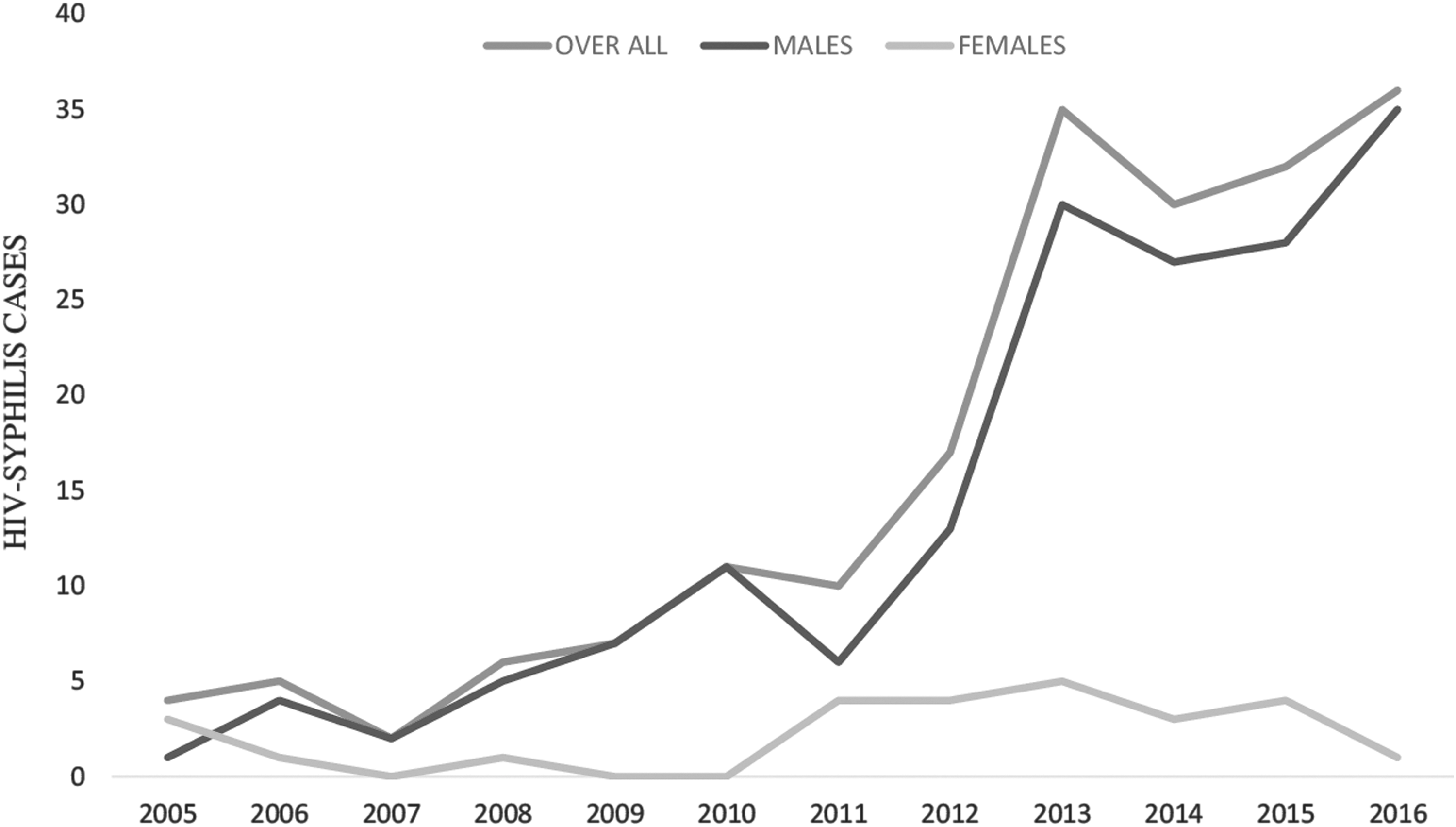
Total HIV–syphilis cases by year.
Regarding the prevalence of HIV–syphilis coinfection, men were found to have a fivefold higher risk of acquiring HIV–syphilis coinfection than women (odds ratio [OR] 5.4; 95% confidence interval [CI] 3.52–8.33; p < .001). In addition, the rate of HIV–syphilis coinfection was higher in the 18–29 years age group than in those aged ≥50 years (OR 4.0; 95% CI 2.01–8.09; p < .001). The rate of HIV–syphilis coinfection was also higher in those who have had more than five partners, or those with two to five partners, than those who had less than or one partner in the past 12 months (OR 4.9; 95% CI 3.26–7.47; p < .001, and OR 2.6, 95% CI 1.69–4.05; p < .001, respectively). Compared with heterosexual behavior, homosexual or bisexual behavior also influenced the rate of syphilis infection among HIV-infected patients (OR 8.6; 95% CI 6.1–12.06; p < .001).
Our study had some limitations. First, we could not determine the cause of the increase in syphilis prevalence during the last 4 years of the study. Second, the reduced sensitivity of nontreponemal tests in primary, as well as late latent syphilis, and the potential for false-negative results owing to prozone reactions might lead to underestimation of syphilis rates. Third, we did not test all of the HIV-infected patients for syphilis, which might have led to selection bias. However, our results are consistent with those of other studies, and are relevant to planning for the clinical care of HIV-infected patients.
In conclusion, the mean HIV–syphilis prevalence was high, especially during the last 4 years of the study. We identified being 18–29 years old, male, having homosexual or bisexual behavior, and having multiple sexual partners in the past 12 months as the main risk factors for syphilis acquisition among HIV-infected patients. Therefore, we believe that individuals with these predictors might be careless with prevention measures, contributing to the increased prevalence of syphilis among HIV-infected patients.
Footnotes
Author Disclosure Statement
No competing financial interests exist.