
Abstract
Kepulauan Riau is a famous tourist destination in Indonesia. The epidemic of human immunodeficiency virus type 1 (HIV-1) infection is gradually increasing in this region. We collected peripheral blood samples from 62 antiretroviral therapy-experienced individuals. The amplification of viral genomic fragments, HIV-1 subtyping, and the detection of HIV drug resistance (HIVDR) were performed. Viral subtyping revealed that the most prevalent HIV-1 subtype/circulating recombinant form (CRF) was CRF01_AE (55.6%), followed by recombinants between CRF01_AE and subtype B (17.8%) and then subtype B (15.6%). Recombinants containing CRF02_AG gene fragments were also detected (11.1%). Regarding HIVDR, no drug resistance-associated major mutations were found in pol genes encoding protease, although minor mutations were frequently detected. Furthermore, major mutations, including M184V (2.2%) and Y188L (2.2%), were identified in the viral pol gene encoding reverse transcriptase derived from a study participant, suggesting that the prevalence of HIVDR is low in the region.
H
HIV is divided into two types, HIV-1 and HIV-2. HIV-1 is distributed worldwide, while HIV-2 is confined primarily to West Africa. HIV-1 is subdivided into four groups: M (major), O (outlying), N (new or non-M, non-O), and P, which are prevalent in specific geographic regions. Group M is responsible for the pandemic and has been further divided into 11 subtypes and subsubtypes, and into recombinant forms, which have, in turn, been divided into circulating recombinant forms (CRFs) and unique recombinant forms. Subtype B is the predominant subtype in the Americas, Europe, and Australia, whereas there is a growing epidemic of non-B subtypes and CRFs in Africa and Asia. 6 CRF01_AE is one of the major CRFs of HIV-1 dominating the global epidemic, and is prevalent throughout Southeast Asia. We previously reported that CRF01_AE was a dominant type of HIV-1 in Indonesia, while other recombinants, including the recombinant between CRF01_AE and subtype B, have emerged in Indonesia. 3,5
Kepulauan Riau is a famous tourist destination in Indonesia. According to its geographic position, the Kepulauan Riau province is located on the borders with Vietnam and Cambodia to the north and Singapore and Malaysia in the west. Kepulauan Riau has seven islands, Karimun, Bintan, Natuna, Lingga, Anambas, Batam, and Tanjung Pinang. 7 The Kepulauan Riau province is one of the top five provinces in Indonesia for new HIV cases per 100,000 population in 2011 after Papua, West Papua, Bali, and Jakarta. 8 The Directorate General of Disease Prevention and Control, Ministry of Health, Republic of Indonesia reported that the annual number of HIV cases was still increasing in the Kepulauan Riau province in recent years, for example, 973 cases in 2014, 885 cases in 2015, 1,037 cases in 2016, and 174 cases between January and March 2017. A total of 6,971 HIV cases were reported between 2009 and March 2017. In this province, HIV has spread rapidly among specific population groups that are generally regarded as high risk groups, namely, injecting drug users, commercial sex workers, and men who have sex with men. The proportion of HIV cases by gender was reported to be 57.4% men versus 42.6% women. 9 Effective prevention and treatment programs are needed against HIV infection. In Indonesia, prevention and monitoring programs for HIVDR are limited; however, a HIVDR analysis may provide helpful information for clinicians to decide whether to start ART for new HIV-infected individuals and switch ART regimens for ART-experienced individuals when treatment failure is suspected. In this study, we aimed to identify the HIV-1 subtypes and CRFs present in Kepulauan Riau, Indonesia and monitor HIVDR among ART-experienced individuals in this region.
Sixty-two HIV-1-infected, ART-experienced individuals were recruited from the voluntary counseling and testing program in Tanjung Pinang “Kemuning” hospital in Kepulauan Riau. The inclusion criterion for study participants was HIV-1-infected individuals on ART for more than 1 year. Ethical clearance was obtained from the Institutional Ethics Committees of Airlangga University (approval number: 25-995/UN3.14/PPd/2013) and Kobe University Graduate School of Medicine (approval number: 784). An informed consent form and questionnaire were provided to each participant for acceptance before their enrollment in this study. Socio-demographic, behavioral, and clinical data, including opportunistic infections and the recent conditions of these individuals, were retrieved retrospectively from medical records (Table 1). The mean age of participants was 40 years, whereas the gender distribution was 33 men (53.2%) and 29 women (46.8%). Regarding the ethnicity of participants, most were Melayu (43.5%) and Tionghoa (related geographical location near Singapore and Malaysia) (33.9%). Fifty-two participants (83.9%) had been on ART for more than 3 years. Nineteen participants (30.6%) were prescribed a first-line regimen of lamivudine (3TC), zidovudine (AZT), and nevirapine (NVP). Thirteen participants (21.0%) were prescribed a first-line regimen of 3TC, AZT, and efavirenz (EFV). Twenty-two participants (35.5%) were prescribed a first-line regimen of tenofovir (TDF), 3TC, and the NNRTI, NVP, or EFV. Thirty-seven patients (59.7%) had opportunistic infections including tuberculosis and cytomegalovirus.
ART, antiretroviral therapy; 3TC, lamivudine; AZT, zidovudine; NVP, nevirapine; EFV, efavirenz; TDF, tenofovir; SD, standard deviation.
Ten milliliters of ethylenediaminetetraacetic acid-anticoagulated whole blood samples were collected from each individual. Plasma was separated by centrifugation for 10 min at 2,000 rpm and stored at −80°C for future analyses. Peripheral blood mononuclear cells (PBMC) were isolated by the BD Vacutainer CPT (Cell Preparation Tube) System (Becton, Dickinson and Company, Franklin Lakes, NJ). DNA was extracted from PBMC using the QIAamp DNA blood mini kit (Qiagen, Hilden, Germany). The HIV-1 pol gene encoding protease (PR gene), RT, gag, and env genes were amplified by the GoTaq green master mix (Promega, Madison, WI) and primer sets as follows. The PR gene was amplified by nested PCR with the primers DRPR05, 5′-AGACAGGYTAATTTTTTAGGGA-3′ [corresponding to nucleotides (nt) 2074–2095 of the HIV-1 reference strain, HXB2 (GenBank accession no. K03455)] and DRPR02L, 5′-TATGGATTTTCAGGCCCAATTTTTGA-3′ (nt 2716–2691) in the first round and DRPR01M, 5′-AGAGCCAACAGCCCCACCAG-3′ (nt 2148–2167) and DRPR06, 5′-ACTTTTGGGCCATCCATTCC-3′ (nt 2611–2592) in the second round. The RT gene was amplified by nested PCR with the primers RT1L, 5′-ATGATAGGGGGAATTGGAGGTTT-3′ (nt 2388–2410) and DRRT4L, 5′-TACTTCTGTTAGTGCTTTGGTTCC-3′ (nt 4402–4380) in the first round, and RT7L, 5′-GACCTACACCTGTCAACATAATTGG-3′ (nt 2485–2509) and DRRT6L, 5′-TAATCCCTGCATAAATCTGACTTGC-3′ (nt 4309–4285) in the second round. The viral gag gene was amplified by nested PCR with the primers H1G777, 5′-TCACCTAGAACTTTGAATGCATGGG-3′ (nt 1231–1255) and H1P202, 5′-CTAATACTGTATCATCTGCTGCTCCTGT-3′ (nt 2352–2325) in the first round, and H1Gag1584, 5′-AAAGATGGATAATCCTGGG-3′ (nt 1577–1595) and G17, 5′-TCCACATTTCCAACAGCCCTTTTT-3′ (nt 2040–2017) in the second round. The viral env gene was amplified by nested PCR with the primers M5, 5′-CCAATTCCCATACATTATTGTGCCCCAGCTGG-3′ (nt 6858–6889) and M10, 5′-CCAATTGTCCCTCATATCTCCTCCTCCAGG-3′ (nt 7661–7632) in the first round, and M3, 5′-GTCAGCACAGTACAATGIACACATGG-3′ (nt 6948–6973) and M8, 5′-TCCTTCCATGGGAGGGGCATACATTGC-3′ (nt 7547–7521) in the second round. PCR conditions are available upon request. PCR products were electrophoresed on a 1.5% agarose gel and visualized under UV light after staining with ethidium bromide. The PCR products amplified at the end-point dilution of DNA templates were subjected to a sequencing analysis to examine the genomic fragment of the major viral population in a sample.
A sequencing analysis was performed using the BigDye Terminator v3.1 Cycle Sequencing kit and ABI PRISM3500xL genetic analyzer (Applied Biosystems, Foster City, CA). Sequencing data were then assembled and aligned using Genetyx version 10 software (Genetyx, Tokyo, Japan). The sequencing data of 39 PR genes [296 base pairs (bp); nt 2253–2543], the N terminus of 29 RT genes (741 bp; nt 2571–3311), the partial fragment of 24 gag genes encoding Gag p24 (390 bp; nt 1633–2002), and the partial fragment of 36 env genes encoding the gp120 C2-V3 region (389 bp; nt 7020–7408) were obtained from 62 peripheral blood samples. The nucleotide sequences of the PR, RT, gag, and env genes have been registered in the GenBank database under accession numbers MG717590–MG717628 (PR genes), MG717629–MG717657 (RT genes), MG717566–MG717589 (gag genes), and MG717530–MG717565 (env genes).
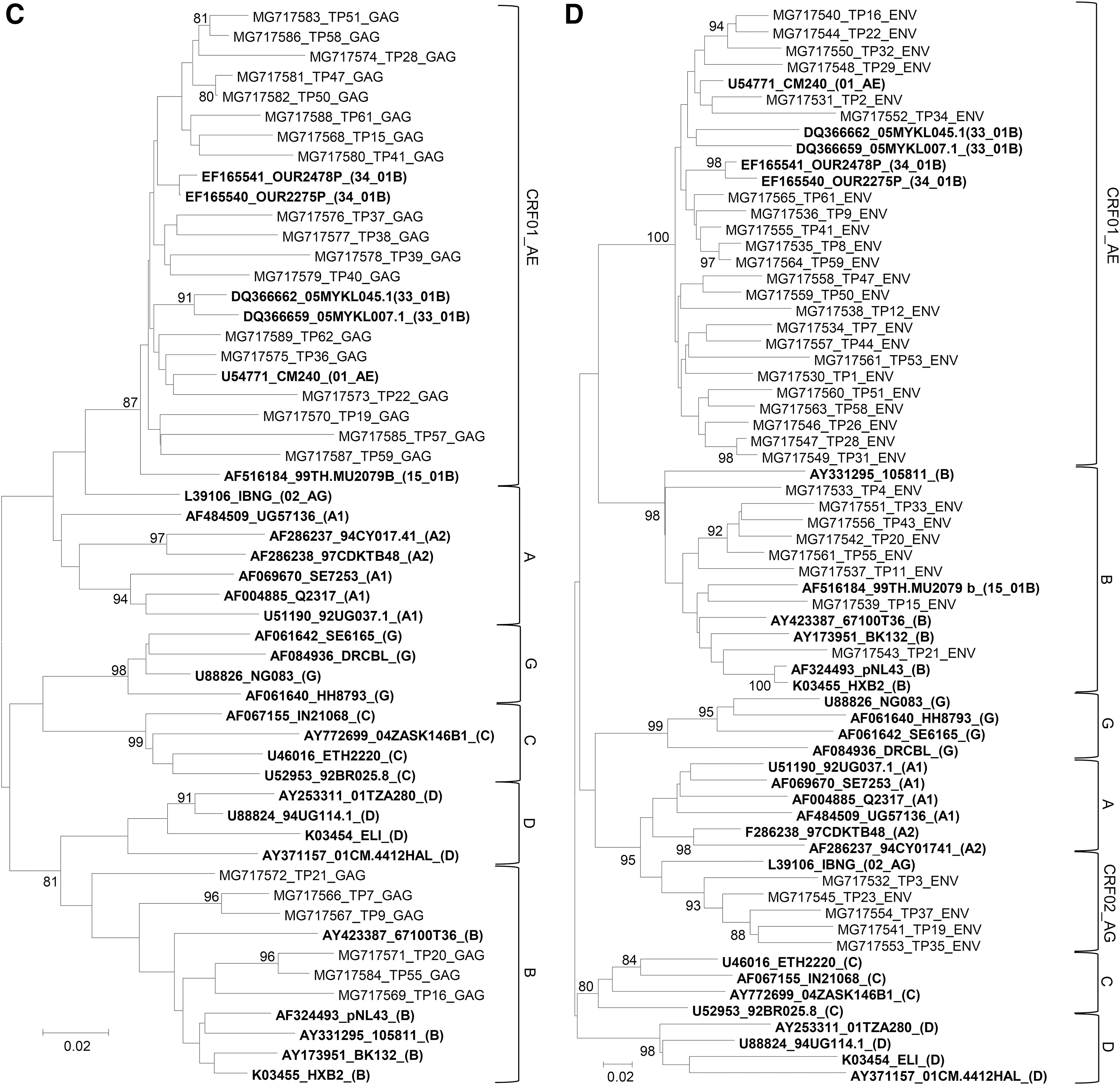
HIV-1 subtyping was then performed by a phylogenetic tree analysis, jumping profile Hidden Markov Model (jpHMM)-HIV tools available on the website (

Phylogenetic tree analysis of HIV-1 PR, RT, gag, and env gene sequences collected in Kepulauan Riau, Indonesia. Phylogenetic trees were constructed for the HIV-1 PR
Drug resistance mutations were detected in the PR and RT genes based on the International Antiviral Society-United States guidelines. 13 No drug resistance-associated major mutations were found in the PR genes (data not shown); however, several minor mutations, such as M36I (an amino acid substitution at position 36 from methionine to isoleucine) (71.8%), L89M (71.8%), I93L (43.6%), L63P (38.5%), K20R (30.8%), and V77I (28.2%), were detected (Table 2). These minor mutations may present as natural polymorphisms, and were detected more frequently in CRF01_AE PR genes than in subtype B PR genes (Table 2), which is consistent with previous findings. 14,15 The high frequency of natural polymorphisms in CRF01_AE PR has been reported previously. 14,15 In contrast, drug resistance-associated major mutations against NRTI and NNRTI, including M184V (2.2%) and Y188L (2.2%), were detected in an RT gene derived from an individual (sample ID: TP8) (Table 3). The individual (sample ID: TP8) had received a combination of TDF, 3TC, and EFV since 2012. The mutation, M184V confers resistance to 3TC, while Y188L confers resistance to EFV. 13 In addition, this individual had opportunistic infections (data not shown); therefore, the prescription of other ART regimens to this individual may be needed to avoid virological failure.
The subtype of PR genes was assigned based on jpHMM, RIP, and phylogenetic analyses.
The identification of drug resistance-associated mutations was based on the guidelines published by the IAS-USA.
jpHMM, jumping profile Hidden Markov Model; RIP, recombinant identification program; IAS-USA, International Antiviral Society-United States; PR gene, pol gene encoding protease.
Mutations associated with high levels of drug resistance are shown according to the guidelines published by the IAS-USA. Drug resistance-associated major mutations are shown in bold.
RT, pol genes encoding reverse transcriptase; NRTI, nucleoside/nucleotide reverse transcriptase inhibitor; NNRTI, non-nucleoside reverse transcriptase inhibitor.
In conclusion, CRF01_AE viruses were the predominant HIV-1 strains in Kepulauan Riau, Indonesia. The predominance of CRF01_AE was consistent with that in other regions in Indonesia. In addition, recombinants between CRF01_AE and subtype B, subtype B, and other recombinants including CRF02_AG gene fragments were detected; therefore, the continuous surveillance of circulating HIV-1 subtypes and CRFs may be required in this country. Moreover, a low prevalence of drug resistance-associated mutations against NRTIs and NNRTIs was noted. Nevertheless, the prescription of first-line ART regimens with two NRTIs and one NNRTI has been expanded in Indonesia, and further large-scale and continuous surveillance studies may be required to monitor the appearance of HIVDR.
Sequence Data
Nucleoside sequences are available under GenBank accession numbers MG717530–MG717657.
Footnotes
Acknowledgments
This work was supported in part by the program of the Japan Initiative for Global Research Network on Infectious Diseases (J-GRID) from the Ministry of Education, Culture, Sport, Science and Technology in Japan, and the Japan Agency for Medical Research and Development (AMED); a grant for the Joint Research Project of the Research Institute for Microbial Diseases, Osaka University; and the Institute of Tropical Disease as the Center of Excellence (COE) program by the Ministry for Research and Technology (RISTEK) of Indonesia. The article was proofread by Medical English Service, Kyoto, Japan.
Author Disclosure Statement
No competing financial interests exist.