
Abstract
The association between human immunodeficiency virus (HIV) infection and tuberculosis (TB) mortality has been studied extensively, but the impact of HIV on other clinically relevant aspects of TB care such as TB drug-related adverse events (AEs), hospital readmissions, and TB treatment duration is less well characterized. We describe the association of HIV infection with TB clinical complexities and outcomes in a high HIV prevalence cohort in the United States. This is a retrospective cohort study among patients treated for culture-confirmed TB between 2008 and 2015 at an inner-city hospital in Atlanta, GA. Univariate analysis was used to estimate association of HIV with TB treatment interruption due to AEs, hospital readmissions, and treatment duration. Final unfavorable TB treatment outcome was defined as death, loss to follow-up, or recurrent TB. Logistic regression modeling was used to estimate association of HIV with final unfavorable outcomes. Among 274 patients with TB, 96 (35%) had HIV coinfection. HIV-positive patients had more TB treatment interruptions due to AE (34% vs. 15%), were more likely to have a hospital readmission (50% vs. 21%), and received longer TB treatment (9.9 months vs. 8.8 months) compared to HIV-negative patients (p < .01 for all). HIV infection was not associated with final unfavorable outcomes in univariate [odds ratio (OR) = 1.86; confidence interval (95% CI) 0.99–3.49] or multivariate analysis (aOR = 1.13; 95% CI 0.52–2.39) (p ≥ .05 for both). While HIV infection was not associated with final unfavorable TB outcomes, TB/HIV coinfected patients had more complex treatment course underscoring the importance of maintaining resources and expertise to treat coinfected patients in our and similar settings.
Introduction
T
While the number of TB cases has been declining in the United States (US), 13 TB/HIV coinfection remains a public health problem in selected areas of the US. 14 A high proportion of coinfected cases were observed during a recent TB outbreak among people experiencing homelessness in Atlanta. 14,15 Most of these patients sought care at the Grady Memorial Hospital (GMH), an inner-city safety net hospital in Atlanta. 14 –16 We aimed to compare clinical outcomes between those with and without HIV coinfection, including mortality, AEs, hospital readmissions, and treatment duration in this cohort. We hypothesized that coinfected cases would have a higher rate of poor outcomes and a more complex treatment course.
Methods
Study design and setting
A retrospective cohort study design was utilized. Adults (≥18 years) with culture-confirmed pulmonary or extrapulmonary TB treated at GMH between January 2008 and October 2015 were eligible for inclusion. 15 Patients with missing baseline drug susceptibility test (DST) or final outcomes were excluded. Following hospital discharge, all patients were referred to a county public health clinic for further management.
All patients had ≥1 respiratory sample submitted for acid-fast bacilli smear microscopy and culture. Extrapulmonary sample was submitted at clinicians' discretion. Between 2008 and 2014, nucleic acid amplification testing with Mycobacterium tuberculosis (MTB) direct assay (Gen-Probe Incorporated, San Diego, CA) was performed for respiratory smear-positive samples; subsequently, the Xpert MTB/RIF assay (Cepheid, Sunnyvale, CA) was performed on respiratory smear-positive samples and for others upon request. Baseline MTB isolates were sent to the Georgia Public Health Laboratory where DST for rifampin, isoniazid, and ethambutol was performed using Mycobacterial Growth Indicator Tube 960 (Becton Dickinson, Franklin Lakes, NJ). Genotyping for baseline MTB samples was performed by the Centers for Disease Control and Prevention. 17
Data management
Data were abstracted from medical records at GMH, local health departments, and the Georgia State Electronic Notifiable Surveillance System and were entered into an online REDCap database. 18
Definitions
Disseminated TB disease was defined as having either a blood culture positive for MTB or by miliary TB based on radiology results. Meningeal disease was defined by detection of MTB in cerebrospinal fluid (CSF) by culture or nucleic acid amplification test or by compatible CSF profile and/or imaging. 19 Recurrent TB was defined as having a second TB episode with the same genotype within 2 years of completing treatment. Low albumin and low hemoglobin were defined as <2.5 gm/dL and <10 gm/dL, respectively. Low glomerular filtration rate (GFR) was defined as <60 mL/min by Cockcroft Gault formula. Final radiology reports were abstracted for chest X-ray (CXR) and computed tomography scans. A drug-related AE was defined as any AE requiring treatment interruption for ≥1 day as determined by the treating clinician, and nature of AE (e.g., rash) was abstracted from clinician notes. Hepatotoxicity was defined as alanine aminotransferase (ALT) ≥3 times the upper normal limit in the presence of hepatitis symptoms as determined by the treating clinician or ALT ≥5 times the upper normal limit regardless of symptoms. 20 A favorable treatment outcome for pulmonary TB was defined as treatment completion and with negative cultures, whereas for extrapulmonary TB it was defined as treatment completion and clinical improvement. 20 Unfavorable outcome was defined as death from any cause, loss to follow-up, or recurrent TB. 20 Cause of death and reason for readmission were ascertained from chart review by a board certified infectious disease physician (M.C.S.). Readmissions for complications related to TB disease (e.g., hemoptysis) or treatment (e.g., rash) were classified as TB disease related. Treatment duration was defined as time between first and last medication administration for TB, regardless of treatment interruptions.
Data analysis
For univariate comparisons, differences in nominal variables were tested using either a Fisher's exact or chi-squared test and for continuous variables either a Mann–Whitney or two-sample t-test as appropriate. A two-sided p-value of <.05 was considered statistically significant. Logistic regression models were used to estimate the association between HIV status and unfavorable outcome. Patients who transferred care out of state (n = 7) were excluded from the final model. An alternative model comparing HIV-positive patients stratified by CD4 count (≤50 and >50 cells/mm3) to HIV-negative patients as the main exposure was also created. Missing baseline weight and height data were imputed with study cohort medians based on gender. Missing baseline albumin, creatinine, or hemoglobin was imputed from medians based on HIV status. Covariates were selected for inclusion in the final model based on previous literature, biologic plausibility, and the purposeful selection strategy. 21 The purposeful selection strategy determined initial variables for inclusion in the final model as those having a p-value <0.10 in univariate analysis. Confounding between the primary exposure and covariates was assessed using the all-possible subsets method and the 20% change in estimate approach. The study was approved by the Emory University and the Georgia Department of Public Health Institutional review boards and the GMH Research Oversight Committee.
Results
Cohort characteristics
Among 367 patients treated for active TB at GMH during the study period, 274 met inclusion criteria (Fig. 1). All patients were tested for HIV. Ninety-six (35%) patients were HIV positive, including 73 (76%) with known HIV before TB diagnosis and 23 (24%) with new HIV diagnosis at time of TB diagnosis (Table 1). Among those with HIV/TB coinfection, the median baseline CD4 was 86 cells/mm3 (IQR 30–212), and the median time between baseline CD4 and TB diagnosis was 1 day (IQR −1 to 7 days).
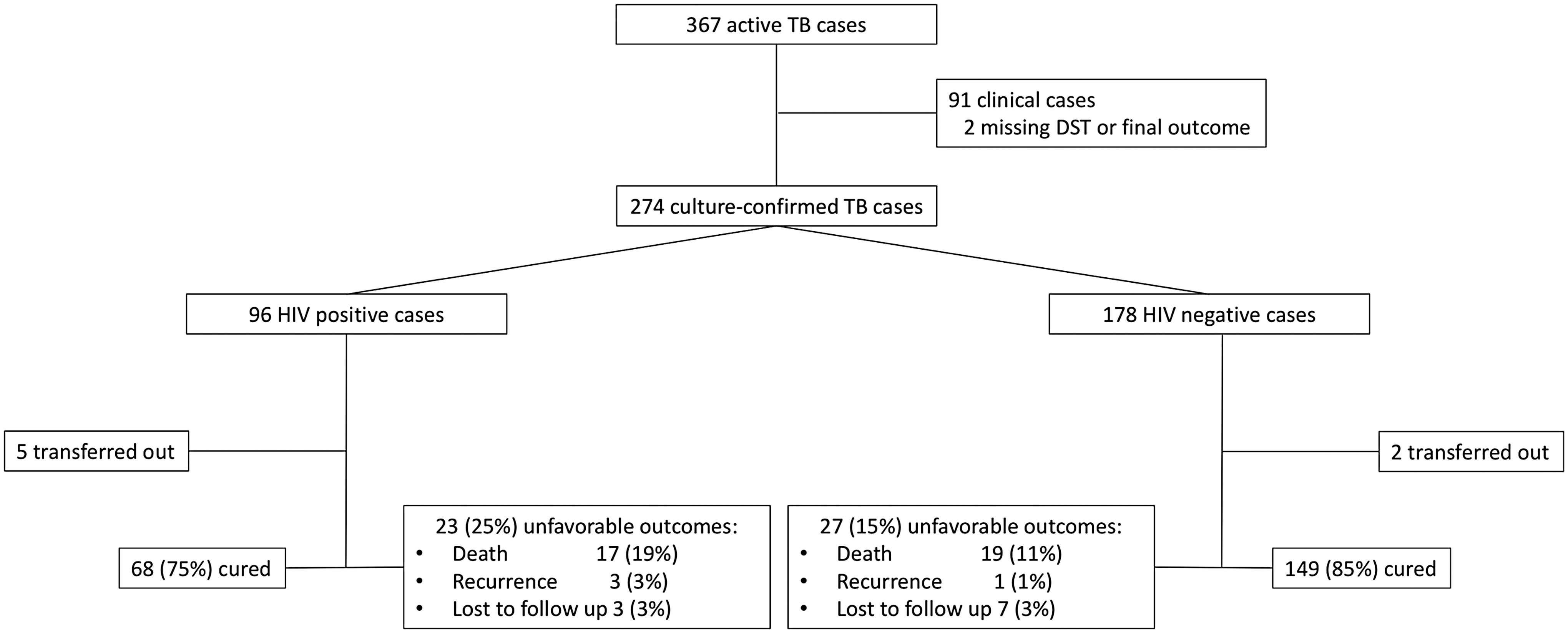
Study flow diagram. DST, drug susceptibility test; HIV, human immunodeficiency virus; TB, tuberculosis.
Index BMI missing (n = 22).
Baseline albumin missing (n = 4).
Baseline hemoglobin missing (n = 5).
Baseline GFR missing (n = 13).
Among patients with pulmonary TB (n = 249).
Among patients with pulmonary and/or pleural TB and CXR available (n = 252; 3 with CXR missing).
Among patients with chest imaging (n = 272).
Lymphatic (n = 31); disseminated (n = 30); pleural (n = 19); meningeal (n = 12); bone (n = 9); genitourinary (n = 7); pericardial (n = 4); soft tissue; splenic (n = 1 each). Some patients have ≥1 site of extrapulmonary disease.
ART, antiretroviral therapy; BMI, body mass index; CXR, chest X-ray; GFR, glomerular filtration rate; HIV, human immunodeficiency virus; IGRA, interferon-gamma release assay; LTBI, latent tuberculosis infection; TB, tuberculosis; TST, tuberculin skin test; US, United States.
The median age was 47 years, and most patients were male (76%), black (81%), and born in the US (72%). Almost half had a history of homelessness (43%), and there were high rates of active tobacco (55%), alcohol (51%), and illicit drug (25%) use. Sixty-four (24%) patients had isoniazid-resistant/rifampin-susceptible TB, and 1 patient had multidrug resistant TB (resistance to isoniazid and rifampin) at baseline. Ninety-four (34%) patients had extrapulmonary TB, including 25 (9%) with only extrapulmonary TB. Thirty (11%) patients had disseminated TB, and 12 (4%) had meningeal TB.
Fifty-six (22%) patients had TB treatment interrupted due to one or more AE (Table 2), hepatotoxicity (7%) being the most common reason for drug interruption. The median TB treatment duration was 9.1 months, and 26 (12%) patients received >12 months of treatment (Table 3). Nine patients had treatment extended beyond 12 months for nonadherence, four patients for AEs, three patients for bone disease, two patients for meningeal disease, and nine due to clinician preference (one patient had both nonadherence and AEs). The median duration of index hospitalization was 8 days, and 13% required intensive care unit admission. Thirty-one percent of patients had ≥1 hospital readmission during TB treatment, and 14% were readmitted ≤30 days after hospital discharge. Forty-eight percent of all readmissions were TB disease related.
Among patients who received any TB drug and data on adverse events available (n = 254).
Numbers between parenthesis denote patients who received drug and data on adverse events available.
Rifampin and/or rifabutin.
Hematologic (n = 7); arthralgia (n = 4); acute interstitial nephritis, neurologic, and ophthalmologic (n = 2 each); gout and hypersensitivity (n = 1 each).
Among patients with pulmonary TB and ≥1 follow-up sputum (n = 243).
Among patients that achieved sputum culture conversion (n = 222).
Among patients without death at index admission (n = 257).
Denominator total readmissions (n = 147).
Among patients who survived >14 days after TB diagnosis (n = 91).
Among patients that completed TB treatment (n = 221).
Excluded patients who were transferred out during tuberculosis treatment (n = 7).
ICU, intensive care unit; MTB, Mycobacterium tuberculosis.
Comparison of characteristics and complexities according to HIV infection
Baseline demographic characteristics were similar between HIV-positive and negative patients, except for illicit drug use which was more common among HIV-positive patients (39% vs. 17%, p ≤ .01) (Table 1). HIV-positive patients were more likely to have isoniazid-resistant/rifampin-susceptible TB (33% vs. 18%, p < .01) than HIV-negative patients. The only case with multidrug resistant TB was also HIV positive. HIV-positive patients were less likely to have abnormal CXR (78% vs. 93%) or cavitary disease (13% vs. 55%) (all with p ≤ .01) than HIV-negative patients. HIV-positive patients were also more likely to have extrapulmonary involvement (50% vs. 26%), including disseminated (21% vs. 6%) and meningeal (8% vs. 2%) TB than HIV-negative patients (all with p < .05). Among 91 HIV-positive patients who survived >14 days after TB diagnosis, 74 (81%) received antiretroviral therapy (ART) during TB treatment and 47 (52%) had viral suppression at end of TB treatment. 16
There were more treatment interruptions due to AE among HIV-positive patients (34% vs. 15%), including of rifamycins (23% vs. 8%), isoniazid (24% vs. 10%), and pyrazinamide (19% vs. 8%) (all with p ≤ .01) compared to HIV-negative patients (Table 2). Similarly, hepatotoxicity was more common among HIV-positive patients compared to HIV-negative patients (13% vs. 3%, p ≤ .01). In addition, HIV-positive patients were more likely to have ≥2 drugs interrupted for AE compared to HIV-negative patients (26% vs. 8%, p ≤ .01). HIV-positive patients received longer median TB treatment compared to HIV-negative patients (9.9 months vs. 8.8 months, p < .01). HIV-positive patients also had longer treatment duration when analysis was restricted to patients without extrapulmonary TB (9.5 months vs. 8.4 months, p < .01) and to patients without isoniazid and/or rifampin TB (9.8 months vs. 9.0 months, p < .01). The median treatment duration was similar among HIV-positive patients that did and did not receive ART during TB treatment (9.9 months vs. 9.8 months, p = .65). Finally, patients that had drug interruptions for AE had longer median treatment duration compared to those without interruption (10.2 months vs. 8.9 months, p < .01).
While the duration of index hospital admission was similar between HIV-positive and negative patients, HIV-positive patients were more likely to be readmitted during TB treatment (50% vs. 21%, p ≤ .01) and had a higher 30-day readmission rate (20% vs. 11%, p = .05). Among HIV-positive patients, overall readmissions were more likely related to TB (55% vs. 39%) and infections other than TB (11% vs. 5%) and less likely unrelated to infections (34% vs. 56%) compared to HIV-negative patients (p = .03). Six of 10 readmissions for infection other than TB among HIV-positive patients were due to opportunistic infections (Pneumocystis pneumonia n = 3, cryptococcal meningitis n = 2, and disseminated histoplasmosis n = 1).
Treatment outcomes
Excluding 7 patients who were transferred out of Georgia during TB treatment, 217 (81%) of 267 were cured, 10 (5%) had loss to follow-up, 4 (1%) had TB recurrence, and 36 (14%) died (Table 3). Seventeen (6%) patients died during index hospital admission, and 3 patients died before starting TB therapy. The median days of treatment among patients that died and were started on TB treatment were 42 (interquartile range 12–188). Most deaths (69%) were TB related.
HIV-positive patients had a lower proportion of cure (75% vs. 85%) and higher proportions of recurrence (3% vs. 1%) and death (19% vs. 11%) compared to HIV-negative patients (p = .08). There was no difference between time of TB diagnosis and death when stratified by HIV status (p = .15 by log-rank test) (Fig. 2), and there was no difference in proportion of deaths related and not related to TB when stratified by HIV infection (p = .15). Among 86 HIV-positive patients that survived >14 days and were not transferred out of Georgia, 70 (81%) received ART during TB treatment. HIV-positive patients that received ART during TB treatment had a higher proportion of cure (84% vs. 56%) and a lower proportion of death (10% vs. 31%) compared to those that did not receive ART during TB treatment (p < .05 for both comparisons).

Survival stratified by HIV status. Survival from date first sample positive for Mycobacterium tuberculosis obtained.
HIV infection did not have a significantly higher odds ratio (OR) for unfavorable outcomes in univariate analysis [OR = 1.86 confidence interval (95% CI 0.99–3.49)] (Supplementary Table S1; Supplementary Data are available online at
Unfavorable treatment outcome was defined as death, recurrence of tuberculosis, or loss to follow-up. Includes patients not transferred-out during TB treatment (n = 267).
Median albumin by HIV status inputted for missing observations (n = 4).
Gender median weight and median creatinine by HIV status inputted for missing observations (n = 13).
CI, confidence interval; OR, odds ratio.
Discussion
In this US-based inner-city cohort, HIV-positive patients experienced a more complex treatment course with more TB treatment interruption due to AE and readmissions, in addition to longer treatment duration. We found a trend for poor TB treatment outcomes (defined as death, loss to follow-up, or recurrent TB) among HIV-positive patients compared to HIV-negative patients, but this was not statistically significant. These results highlight the importance of evaluating outcomes other than mortality.
There were a higher proportion of deaths among HIV-positive patients in this cohort, and the lack of statistical significance could be due to sample size. Renal dysfunction, low albumin, and disseminated/meningeal disease were associated with poor outcomes in this and other cohorts. 4,22 –24 Almost a quarter of the patients had low albumin at presentation, suggesting advanced disease. 4 The lack of effect of HIV on TB treatment outcomes could be due to care in health departments with providers experienced in care for TB/HIV coinfection, individualized treatment for TB and HIV, and use of prophylaxis for opportunistic infections. 7 The observed higher death rate in our cohort compared to overall US rates for HIV-positive (19% vs. 11.3%) and HIV-negative (11% vs. 4.8%) TB cases suggests that advanced TB at presentation among HIV-positive and negative patients could have mitigated the effect of HIV on outcomes. 8
Few studies have examined association of HIV with AE, and most found increased AE among coinfected patients. 9 –11 Our results were similar with treatment interruptions for drug AE occurring more frequently among coinfected patients. Importantly, those with drug interruptions had a longer treatment course in our cohort. Interestingly, while HIV infection is associated with decreased rifampin absorption, 25 immune activation secondary to HIV has been associated with impaired isoniazid and pyrazinamide clearance. 26,27 Impaired drug clearance could explain higher rates of TB drug AEs among patients with HIV coinfection. Management of TB/HIV coinfection requires knowledge of complex drug interactions, and the U.S. Department of Human Health Services guidelines suggest consultation with an expert for patients on ART experiencing TB drug AE, another reason to maintain expertise in the management of TB/HIV coinfection. 28
Prolonged treatment regimens were used in this cohort, with a median TB treatment duration of 8.8 months. Twelve percent of patients were treated for >12 months, most due to physician preference or treatment nonadherence. HIV positive had longer treatment duration compared to HIV-negative patients, even when analysis was restricted to patients without extrapulmonary or drug-resistant TB. Based on limited data, ATS/CDC/IDSA guidelines recommend extending TB therapy for patients with HIV only when ART is not prescribed during TB treatment. 20 However, treatment duration was similar regardless of ART use in our cohort and only 10% of HIV-positive patients completed TB treatment <7 months. This suggests that physician preference and patient adherence, and not only new drugs, are key factors to shorten TB treatment.
Nearly one-third of the patients were readmitted during TB therapy, and HIV-positive patients had more readmissions (50% vs. 21%). Our readmission and death at index admission rates were similar to those reported for community-acquired pneumonia in the US, 29 and a higher rate of readmissions among HIV-positive patients was observed in a study that included patients with and without TB. 30 Almost half of all readmissions in this cohort were TB related. Hospitalized patients with TB in the US tend to be older, have more comorbidities, longer length of stay, and incur higher costs compared to hospitalized patients without TB. 3 The complexity of the patients in this cohort and frequency of readmissions support ATS/CDC/IDSA recommendations for hospitals located in areas where TB is prevalent to provide training and education on TB management to medical staff. 31
Our study has limitations. Clinical cases were excluded. It is likely that there were a higher proportion of HIV-positive patients among clinical cases given reduced sensitivity of TB diagnostics among patients with HIV. 32 Anecdotally, our experience is that HIV-positive clinical cases have increased extrapulmonary involvement compared to HIV-negative cases, and therefore, inclusion of clinical cases could have strengthened the association of HIV with TB treatment complexities and outcomes. There are mixed data on the association of hepatitis C virus (HCV) infection with TB outcomes, 33,34 and the lack of association of HCV infection with TB outcomes in our cohort could be due to small sample size. The lack of data on duration of symptoms before presentation and healthcare encounters before TB diagnosis cohort limits conclusions on measures to improve outcomes. Cause of death and reason for readmissions were determined retrospectively, and drug AE was based on clinical documentation potentially limiting accuracy.
Conclusion
Patients with TB/HIV had a more complex treatment course with higher rates of TB treatment interruption for AE, longer treatment duration, and more hospital readmissions compared to those without HIV. These data support the need to maintain resources and expertise to manage TB/HIV coinfected patients in the US.
Footnotes
Acknowledgments
The study was supported, in part, by grants from the National Institutes of Health (NIH) National Institute of Allergy and Infectious Diseases (K23AI103044 and R21AI122001 to R.R.K.) and National Center for Advancing Translational Science (UL1TR000454 in support of the Atlanta Clinical and Translational Science Institute and UL1TR002378 to the Georgia Clinical and Translational Science Alliance [Georgia CTSA]). The authors are indebted to Ms. Sadie Sellers at the Fulton County Board of Health Department, Dr. Rose Marie F. Sales at the Georgia Department of Public Health, and the nurses providing care for patients living with TB in Georgia for their assistance with data collection.
Author Disclosure Statement
No competing financial interests exist.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.