
Abstract
In Pakistan, HIV has converted from outbreak to concentrated epidemic and has also bridged into the low-risk population. The HIV epidemic in Pakistan mainly comprises subtype A. Here, we present the first case and genetic analysis of a circulating recombinant form 56_cpx in a Pakistani HIV-infected patient. Genetic analysis of the sequence indicated that Pakistani 56_cpx sequence had more drug resistance mutation than the other 56_cpx sequences available in the database.
HIV-1
More recently, HIV infection has bridged from PWIDs and MSM low-risk population, including the female spouses and children of these PWIDs and/or MSM. 4 The HIV epidemic in Pakistan is mainly driven by 13 HIV-1 subtypes, which are A, B, C, D, G, A1D, A1G, 01G, CG, 01_AE, 02A1, 02_AG, and 35_AD, where subtype A has been identified as the major subtype. 2,5
Here we report the first incidence of a unique CRF, CRF56_cpx, in Pakistan. The subtype was sequenced from a 29-year-old male patient, diagnosed with HIV-1 during May 2017, by amplifying the partial pol gene. The patient consented to participate in the study, and the study was approved by the Aga Khan University Ethical Review Committee. The sequence was submitted to GenBank and was assigned acc. no. MH021597. HIV-1 genotyping/subtyping was carried out using the HIV BLAST tool available at the HIV Los Alamos Database (
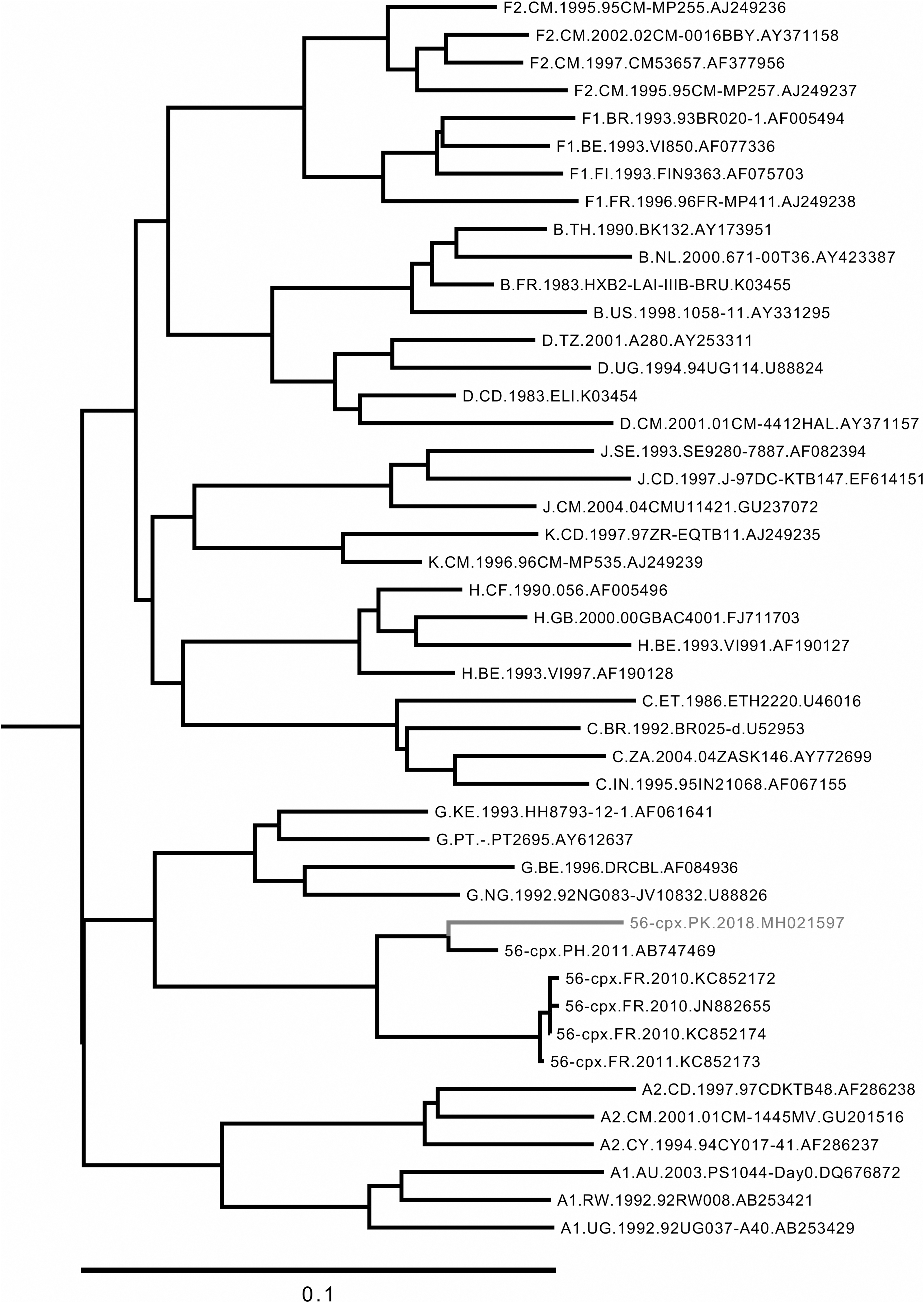
Phylogenetic analysis of HIV sequences: The analysis was performed using the maximum likelihood method. Phylogenetic tree was constructed using HIV partial pol sequence from the Pakistani patient (acc. no. MH021597) and HIV reference sequences belonging to different subtypes and CRFs obtained from HIV Los Alamos Database. A 56-cpx sequence from Pakistan (56-cpx.PK.2018.MH021597) is shown in gray. CRFs, circulating recombinant forms.
CRF56_cpx has evolved from a complex recombinant between HIV-1 subtype B, G, and CRF02, and to-date has only been reported in France and Philippines during the years 2010 to 2012, with only seven sequences available in the database for reference. 2,3
The patient had a history of travel to a Gulf country, where he might have acquired the infection through sexual contact. The baseline CD4 count of the patient was 237, while the viral load was 30,447 copies. The patient was started on the first line antiretroviral therapy (ART), comprising tenofovir/lamivudine (3TC)/efavirenz (EFV). Within 2 months, the CD4 count of the patient dropped to 129, whereas the viral load persisted at 26, 700 copies. The drop in CD4 count encouraged us to analyze the sequence for the presence of drug resistance mutations (DRMs). The drug resistance analysis was performed using the Stanford Drug Resistance database. This analysis revealed the presence of five DRMs in reverse transcriptase region. Out of these, mutations K101P, K103N, and V108I were found to confer resistance against non-nucleoside reverse transcriptase inhibitor (NNRTI), whereas mutations such as L74I and M184V confer resistance against the NRTI.
Drug resistance profile of the patient suggested high-level resistance against abacavir (ABC), didanosine (ddI), emtricitabine (FTC), 3TC, EFV, etravirine, nevirapine, and rilpivirine. In the next step, we performed the drug resistance analysis of other (n = 7) CRF 56_cpx sequences previously submitted to the Los Alamos database, to compare the DRMs observed in the Pakistani strain with DRMs observed in other 56_cpx strains. Interestingly, out of seven sequences, only one sequence had NRTI resistance mutation M184I, which is a variant of DRM M184V and has been reported to be associated with high-level resistance to 3TC and FTC as well as low-level resistance to ABC. This indicated that Pakistani 56_cpx sequence had more DRMs than other 56_cpx sequences available from France and Philippines. In addition, in this Pakistani patient, these DRMs were acquired as the patient had no prior exposure to antiretroviral drugs.
The report of drug-resistant CRF 56_cpx in Pakistan suggests that in addition to subtype A, and other subtypes mentioned earlier, several other CRFs may also be circulating in Pakistan. The findings also highlight the importance of viral sequencing/genotyping and DRM analysis before the start of ART so that the right ART combination can be tailored for the patient and spread of drug-resistant viruses could be prevented.
Footnotes
Acknowledgments
This research was funded by Aga Khan University Seed Money (grant no. PF84/0716) and Higher Education Commission (grant no. HEC-5217).
Author Disclosure Statement
No competing financial interests exist.