
Abstract
Human immunodeficiency virus (HIV) primary drug resistance (PDR) has influenced the long-term therapeutic effects of antiretroviral drugs. However, for the overall PDR prevalence in China, no report was found in published articles. In our study, an extensive cross-sectional investigation based on all newly diagnosed treatment-naive HIV-infected individuals was conducted. The overall prevalence of HIV-1 PDR among newly diagnosed treatment-naive HIV-1 individuals was 8.3% (60/720), obviously beyond the warning line (5.0%) set by WHO. The prevalence of PDR to PIs, nucleoside reverse transcriptase inhibitors, and non-nucleoside reverse transcriptase inhibitors was 4.9% (35/720), 0.4% (3/720), and 2.5% (18/720), respectively. Moreover, the occurrence of HIV-1 PDR strains was random among different prefectures. HIV-1 PDR strains were extensively circulating among the sexual contact population inside and outside the Hebei province, especially between neighboring provinces and Hebei. Hebei province has become the moderate level PDR epidemic area. Enhanced surveillance for PDR is necessary among treatment-naïve individuals in Hebei, and we must take effective measures to cut off the spread of HIV PDR strains.
I
Hebei province, located in North China, is an economically underdeveloped area with more than 74 million people. The first HIV-infected case was observed in 1989 in Hebei. 4 A total of 7303 HIV-infected cases were reported between 1989 and 2015. After 10 years of implementation of the free ART program launched in 2003 in Hebei, HIV-1 transmitted DR strains were ever observed in recently infected treatment-naive men who have sex with men (MSM) at MSM sentinel surveillance points in Hebei. 5 However, the systematic assessment of HIV-1 primary drug resistance (PDR) among treatment-naïve individuals nationwide has never been reported.
In this work, to investigate regional HIV-1 PDR among treatment-naive individuals and its epidemic trend, an extensive cross-sectional investigation based on all newly diagnosed treatment-naive HIV-infected individuals in 2013 was conducted according to the protocol recommended by World Health Organization (WHO). 6
A total of 978 HIV-1-infected individuals were newly reported by the Hebei province in 2013, and never received ART. Seven hundred twenty HIV-1 pol (HXB2:2147–3462) gene sequences were obtained from these newly reported HIV-1 individuals, accounting for 73.6% (720/978). Their epidemiological information was obtained by face-to-face interviews using the questionnaire method during blood samples collection. Seven hundred twenty subjects with pol gene had a 100% coverage of all prefectures of Hebei; furthermore, the cross-sectional investigation on PDR can indeed reflect the prevalence of HIV-1 PDR among treatment-naïve HIV-1 individuals in Hebei. Written ethical approval was obtained from the local Ethics Committee at Hebei Provincial Center for Disease Control and Prevention.
HIV-1 DR gene mutations were detected using in-house method. As described previously,
7
HIV-1 RNA was extracted from 720 study subjects, HIV-1 partial pol gene (HXB2:2147-3462) was amplified, sequenced, edited, and assembled,
8
and HIV-1 genotypes were confirmed using methods reported previously by our study team.
9
Moreover, HIV-1 pol sequences were submitted to the HIV DR database (
The data under study were entered into a database and statistical analysis was conducted using SPSS Version 19.0 (SPSS, Inc., Chicago, IL). Means or frequencies of demographic data (gender, age, CD4 counts, ethnicity, transmission route, marital status, etc.) were calculated. Chi-square test was used for analyzing PDR distribution.
Of 720 subjects with pol, men were predominant, accounting for 88.1%. Subjects aged 19–49 accounted for 83.6%. Nearly 95.0% were of Han ethnicity. About 68.9% were infected with HIV-1 through MSM, however, HIV transmission through blood and mother to child transmission only accounted for 0.4% and 0.6%, respectively. Nearly 78.2% received high school or less education. 11.7% had a venereal infection. Of 12 occupations, farmers accounted for 40.5%, followed by commercial services (25.4%), workers (7.7%), and others. At least 15 sample sources were identified, including voluntary counseling and testing (35.9%), other clients (22.2%), preoperative detection (14.3%), blood donation (7.3%), and so on.
According to methods 9 reported previously by us, a total of nine HIV-1 genotypes were found in 720 newly diagnosed treatment-naïve HIV-1 individuals in this study. Of these nine genotypes, CRF01_AE was the most predominant genotype, accounting for 52.8% (380/720), followed by CRF07_BC (23.9%, 172/720), subtype B(16.3%, 117/720), URFs (4.4%, 32/720), CRF08_BC (1.0%, 7/720), subtype C (1.0%, 7/720), CRF55_01B (1.0%, 7/720), subtype A6 (0.1%, 1/720), and CRF65_cpx (0.1%, 1/720).
The overall prevalence of HIV-1 PDR mutations among newly diagnosed treatment-naive HIV-1 individuals was 8.3% (60/720), causing a low- to high-level DR. Of these PDR mutations, the prevalence (3.1%, 23/720) of gene mutations at position 46 in protease gene coding region was the highest, presenting a low-level DR to NFV/r, followed by E138AE (0.6%, 4/720). The prevalence of each of other mutations resulting in DR to protease inhibitors (PIs) or reverse transcriptase inhibitors (RTIs) was less than 0.5%, respectively. The prevalence of DR to PIs, nucleoside RTIs (NRTIs) and non-nucleoside RTIs (NNRTIs) was 4.9% (35/720), 0.4% (3/720), and 2.5% (18/720), respectively.
Nine of 60 newly diagnosed naïve HIV-1-infected individuals with mutations harbored more than two mutation points, including double mutations (0.7%, 5/720) in two gene coding regions, multiple gene mutations (0.1%, 1/720) in three gene coding regions, and multisite mutations (0.4%, 3/720) in single-gene coding region.
PDR mutations were wholly observed in the sexual contact population and eight of 9 genotypes identified in this study. Moreover, HIV-1 PDR strains were observed in all 11 prefectures of Hebei (Table 1), and showed no significantly different distribution (χ 2 = 7.750, p = .653). The highest PDR prevalence was in Xingtai (15.8%), followed by Hengshui (11.8%), Cangzhou (11.5%), Zhangjiakou (10.0%), and so on. This suggests that the occurrence of HIV-1 PDR strains is random.
Figure 1 revealed the DR level of antiretroviral drugs. A total of 19 drugs are listed in the Stanford HIV Drug Resistance Database. This study revealed that five NRTIs (3TC, ABC, DDI, FTC, and TDF) of 19 drugs showed no HIV-1 DR, however, the remaining 14 drugs occurred the obvious resistance from low to high level. Of them, the resistance rate to NFV/r was the highest, achieving 4.0% (29/720), followed by NVP (1.7%, 12/720), RPV (1.3%, 9/720), EFV (1.1%, 8/720), IDV/r (0.9%, 6/720), TPV/r (0.8%, 6/672), DRV/r (0.7%, 5/720), FPV/r (0.7%, 5/720), LPV/r (0.7%, 5/720), and each of other drugs with 0.6%.
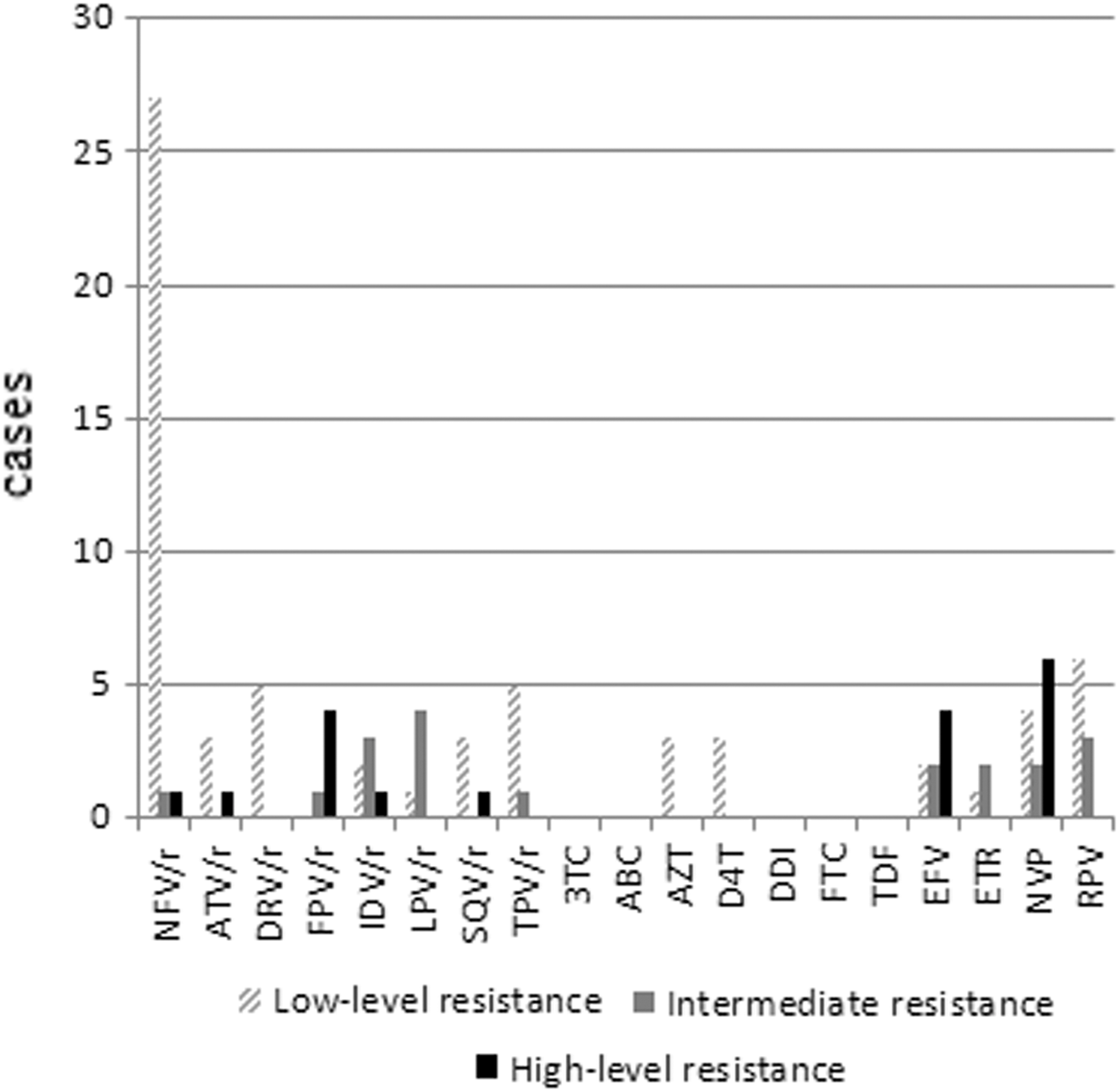
Drug resistance levels of antiretroviral drugs among treatment-naïve HIV-1 individuals in Hebei.
In the CRF01_AE maximum-likelihood (ML) tree (Fig. 2), five clusters containing resistance mutations were observed, including LN/TJ/BJ_Cluster, LN_Cluster, GD/GX_Cluster, SJ/BD_Cluster, and SJ/TS/CZ_Cluster. Within these CRF01_AE clusters related to PDR, HIV-1-resistant strains containing PIs mutations (M46 L, M46I, and V82F) were the most frequent, followed by three NNRTIs mutations (G190E, N348I, and E138AE). Figure 2 indicated that two (LN/TJ/BJ_Cluster and LN_Cluster) of 5 CRF01_AE clusters related to DR proved the circulation of HIV-1-resistant strains between neighboring provinces (Liaoning, Beijing, and Tianjin) and Hebei. As such, SJ/BD_Cluster and SJ/TS/CZ_Cluster indicated the close transmission relationship of HIV-1 resistant CRF01_AE strains among the prefectures (Shijiazhuang and Baoding; Shijiazhuang, Tangshan, and Cangzhou), Hebei. GD/GX_Cluster revealed that HIV-1 resistant CRF01_AE strain containing E138E was introduced into Hebei through sexual contact from Guangdong or Guangxi.

Transmission clusters of HIV-1 PDR strains observed in the CRF01_AE maximum-likelihood tree. The maximum-likelihood tree was constructed using MEGA 6.0 with 1,000 bootstrap replicates. The reference sequences (•) were obtained from the HIV database (
In the CRF07_BC ML tree (Fig. 3), one LN/BJ_Cluster and two SC_Clusters (SC_Cluster 1 and SC_Cluster 2) were indicated among our CRF07_BC sequences. Within LN/BJ_Cluster, HIV-1-resistant strains containing PIs mutations (Q58E, M46 L, and L76LV/I84 V) and NNRTIs mutations (V106 M and V106A) were extensively circulating between neighboring provinces (Liaoning and Beijing) and Hebei. SC_Cluster 1 and SC_Cluster 2 were two transmission clusters closely related to Sichuan, containing E138AE (ZJ12491ID) and K103 N (XT12310H) NNRTIs mutations, respectively. As shown in Figure 3, SC_Cluster 1 was distantly related to SC_Cluster 2, suggesting that HIV-1 resistant CRF07_BC strains were introduced into Hebei at different times through MSM, IDU, or heterosexuals from Sichuan.

Transmission clusters of HIV-1 PDR strains observed in the CRF07_BC maximum-likelihood tree. The maximum-likelihood tree was constructed using MEGA 6.0 with 1,000 bootstrap replicates. The reference sequences (•) were obtained from the HIV database (
Figure 4 indicated that HIV-1 subtype B strains harboring NNRTIs mutations were circulating in two transmission clusters designated B_cluster 1 and B_cluster 2. In B_cluster 1, sequences containing NNRTIs mutations (K101E and V108IV) clustered with the reference sequences from other provinces (Shandong, Henan, Shanxi, Guangdong, Anhui, Yunnan, etc.), of China. B_cluster 2 was one PDR transmission cluster closely associated with Beijing, suggesting that HIV-1 subtype B strain containing E138G was circulating between Beijing and Hebei. Additionally, subtype A6 containing E138A and CRF08_BC containing E138A and T215D closely clustered with the reference sequences.

Transmission clusters of HIV-1 PDR strains observed in the maximum-likelihood tree including subtype B, subtype A6, URFs, and CRF08_BC. The maximum-likelihood tree was constructed using MEGA 6.0 with 1,000 bootstrap replicates. The reference sequences (•) were obtained from the HIV database (
Figures 2 –4 revealed that all sequences harboring low to high level DR mutations except for resistant URFs were included in transmission clusters. Within three main genotype strains, HIV-1 strains resistant to PIs and NNRTIs were extensively circulating among the sexual contact population inside and outside the province of Hebei, especially between neighboring provinces (such as Beijing and Liaoning) and Hebei. No strains resistant to NRTIs were found in three main genotypes. However, URFs harbored only NRTIs mutations (T215AT and K219E). The sexual contact especially MSM became the most predominant driver of HIV-1-resistant strains spread.
Many studies indicated that the probability of HIV virological failure would increase two to three fold among ART-naïve individuals with primary DR, and this will reduce the long-term therapeutic effects of the first-line drugs. 10 Currently, the prevalence of HIV PDR in China was 4.7%, 11 which stayed low, but was also close to the warning line set by WHO. In our study, the prevalence of HIV-1 PDR in Hebei was 8.3%, which was only lower than the prevalence of HIV PDR (9.6%) in Northeast of China, however, obviously higher than that in other areas (less than 7.7%) of China. 11
The previous report indicated that compared with other high risk behaviors, HIV PDR was more likely to occur in the MSM population. 12 In Hebei, 68.9% were infected with HIV-1 through MSM in 2013. Therefore, we infer that the increase of MSM transmission is one of the major drivers of high PDR in Hebei.
A meta-analysis, 11 including 76 articles, proved that the rates of HIV PDR to PIs, NRTIs, and NNRTIs were 1.4%, 1.8%, and 2.3% in China, respectively. For our study, completely different from the above PDR prevalence in China, the prevalence of PDR to PIs was the highest (4.9%), followed by NNRTIs (2.5%) and NRTIs (0.4%), and this PDR distribution in PIs, NRTIs, and NNRTIs among treatment-naïve individuals in our study was in accord with that among MSM in China. 13 Furthermore, the DR prevalence to PIs, NRTIs, and NNRTIs between this study and our earlier study on DR in treatment-failure individuals in Hebei showed the significant difference.
This study indicated that the prevalence (4.9%) of PDR to PIs in Hebei was also close to the intermediate resistance warning line (5.0%) enacted by WHO, and obviously higher than that (1.4%) in China. 11 We infer that factors related to the high prevalence of PDR among treatment-naïve HIV-1individuals are as follows: first, only lopinavir plus ritonavir (LPV/r) among PIs was included in therapeutic regimens used in Hebei. There were a contradiction between the higher PIs PDR prevalence and the lower rate of PIs use, suggesting that drug-selected mutations adapted to PIs might not be the major factor. Second, our study also proved that HIV-1 PDR strains found in Hebei were mainly circulating between Hebei and neighboring provinces such as Beijing, Liaoning, and Tianjin through the sexual contact, especially MSM.
Beijing, Liaoning, and Tianjin are all international metropolises where many unregistered floating population from other countries live. Moreover, in these cities, MSM transmission has been the most predominant route of HIV spread. A meta-analysis 13 indicated that there was a higher PDR prevalence among MSM in North China (8.38%), northeast (4.23%) and east (3.58%) China, higher than in other areas of China. Therefore, the high PDR prevalence in Hebei might be closely associated with the transmission of imported HIV PDR strains from other countries in Beijing, Liaoning, and Tianjin.
In conclusion, the HIV PDR prevalence (8.3%) in Hebei, a moderate level (5.0%–15.0%), has been obviously beyond the warning line (5.0%) set by WHO. Particularly, MSM has become the most predominant transmission route of HIV PDR strains between Hebei and neighboring provinces. Enhanced surveillance for PDR is necessary among treatment-naïve individuals in Hebei, and we must take effective measures to cut off the spread of HIV PDR strains.
Footnotes
Acknowledgments
This study was implemented with the support of the Natural Science Fund of Hebei Province (H2016303006). The sequences reported in this study have been submitted to GenBank with accession numbers KU378038-KU378046, KX198562-KX198564, KX198566, KX198569-KX198575, KX198586, KX198578-KX198584, and MF684019-MF684335.
Authors' Contributions
X.L., Z.C., and K.L. conceived the study project. X.L., Y.L., Y.W., K.L., and C.Z. complicated the whole study and experimental data. X.L. drafted the article. S.C. and K.L. revised this article. H.Z. and Y.Z. investigated HIV-1-infected individuals` epidemiological data. All authors read and approved the final article.
Author Disclosure Statement
No competing financial interests exist.