
Abstract
To explore reasons for the disproportionate metabolic and cardiovascular disease burdens among older HIV-infected persons, we investigated whether associations of CD4 count and HIV viral load (VL) with non-high-density lipoprotein cholesterol (non-HDL-C) and high-density lipoprotein cholesterol [HDL-C] differed by age. Longitudinal clinical and laboratory data were collected between 2011 and 2016 for HIV-infected outpatients in the DC Cohort study. Using data for patients aged ≥21 years with ≥1 cholesterol result and contemporaneous CD4/VL results, we created multivariable linear regression models with generalized estimating equations. Among 3,912 patients, the median age was 50 years, 78% were male, 76% were non-Hispanic black, 93% were using antiretroviral therapy, 8% had a CD4 count <200 cells/μL, and 18% had an HIV VL ≥200 copies/mL. Overall, CD4 count <200 (vs. >500) cells/μL and VL ≥200 copies/mL were associated with lower non-HDL-C concentrations (p < .01), but associations were more positive with increasing age (CD4–age/VL–age interactions, p < .01). CD4 count <200 cells/μL was associated with lower non-HDL-C among patients aged <50 years [β = −7.8 mg/dL (95% confidence interval, CI: −13.2 to −2.4)] but higher non-HDL-C among patients aged 60–69 years [β = +8.1 mg/dL (95% CI: 0.02–16.2)]. VL ≥200 copies/mL was associated with lower non-HDL-C among patients aged <50 years [β = −3.3 mg/dL (95% CI: −6.7 to 0.1)] but higher non-HDL-C among patients aged ≥70 years [β = +16.0 mg/dL (95% CI: −1.4 to 33.3)], although precision was reduced in age-stratified analyses. Although no age differences were detected for HDL-C, VL ≥200 copies/mL was more strongly associated with lower HDL-C concentrations when CD4 count was <200 cells/μL [β = −7.0 mg/dL (95% CI: −9.7 to −4.3)] versus 200–500 cells/μL [β = −4.2 (95% CI: −5.9 to −2.6)] or >500 cells/μL [β = −2.2 (95% CI: −3.7 to −0.8)] (CD4–VL interaction, p < .01). We detected a novel age-modified relationship between immunosuppression and viremia and atherogenic cholesterol patterns. These findings may contribute to our understanding of the high risk of dyslipidemia observed among persons aging with HIV.
Introduction
S
Dyslipidemia is a common metabolic comorbidity affecting HIV-infected persons. Based on various definitions, its prevalence in large HIV cohort studies has ranged from 31% to 81%. 5 –10 In the setting of untreated HIV infection, serum triglyceride concentrations are typically higher and total cholesterol, low-density lipoprotein cholesterol (LDL-C), and particularly high-density lipoprotein cholesterol (HDL-C) concentrations are generally lower than in uninfected persons. 11 Although the use of antiretroviral therapy can normalize serum lipid concentrations to an extent, specific antiretroviral drugs have also been implicated in causing lipid imbalances including high concentrations of atherogenic cholesterol. Ultimately, one's lipid profile depends on the interactions of his/her specific antiretroviral regimen, gender, race, genomic traits, and lifestyle factors. 11,12 Among HIV-infected persons, associations have also been observed between markers of HIV disease progression and antiretroviral treatment responses and serum lipid concentrations. Lower CD4 T lymphocyte cell count and/or higher HIV RNA viral load (VL) have been associated with increased concentrations of triglycerides and decreased concentrations of total cholesterol, LDL-C, and HDL-C. 13 –18
One epidemiologic study explored whether associations between CD4 cell count and HIV VL and markers of metabolic function, including lipid concentrations, might differ by age group, categorized in that study as <30, 30–50, and >50 years. 13 A statistically significant synergistic interaction between CD4 count and age was detected when modeling serum albumin and hemoglobin concentrations, whereby stronger positive associations between CD4 count and albumin or hemoglobin concentrations were observed among patients older than 50 years. However, age did not significantly modify associations between CD4 count or VL and lipid concentrations. The null findings could have been a consequence of inadequate statistical power, with only 8% of the study sample having been >50 years old and the subsequent lack of the use of finer age group subdivisions beyond 50 years, as well as due to there having been limited data points available for lipid levels.
To explore potential reasons for the disproportionate metabolic disease and CVD burdens among older HIV-infected persons, we investigated whether associations between CD4 cell count and HIV VL and serum concentrations of non-HDL-C and HDL-C varied by age. We hypothesized that immunosuppression and HIV viremia would be more strongly associated with atherogenic cholesterol patterns among older patients. Knowledge of the collective impact of CD4 count, VL, and age on cholesterol concentrations could inform the need for more frequent cholesterol monitoring for HIV-infected patients aging in the context of immunosuppression and/or viremia, particularly since the natural aging process is associated with a decline in CD4 count. 19 This knowledge might also contribute to a greater use of interventions to control dyslipidemia and prevent CVD, such as lipid-lowering therapy, among HIV-infected persons.
Materials and Methods
Study population
We analyzed data from the DC Cohort study, an ongoing prospective multicenter observational study of HIV-infected outpatients at 13 major community, academic, and government clinical sites in Washington, DC; the methods of this study have been described previously. 20 In brief, HIV-infected patients were enrolled on an ongoing basis beginning in January 2011 and prospectively followed from the visit at which written informed consent was provided. Sociodemographic, clinical, and laboratory data documented in outpatient electronic medical record (EMR) systems were routinely monitored and abstracted into the DC Cohort database. The protocol was approved by multiple Institutional Review Boards including the George Washington University Institutional Review Board.
This analysis included DC Cohort study participants ≥21 years of age who were enrolled by September 2015. In addition, the analytic sample was restricted to patients who had at least one test result available for non-HDL-C and/or HDL-C, and also had documented test results for both CD4 count and HIV RNA VL within ±14 days of cholesterol testing. This inclusion criterion ensured that contemporaneous measurements for key variables of interest were available. Data collected between January 2011 and January 2016 contributed to this analysis.
Measures
The two outcome variables were serum concentrations of non-HDL-C and HDL-C, representing, respectively, the cholesterol fractions known to be positively and negatively associated with increased risk of CVD. 21,22 Non-HDL-C, calculated as total cholesterol minus HDL-C, was selected over LDL-C as a primary measure for atherogenic cholesterol as non-HDL-C is a stronger predictor of CVD morbidity and mortality and constitutes the cholesterol carried by all potentially atherogenic particles, including LDL, intermediate density lipoproteins, very low-density lipoproteins, chylomicron remnants, and lipoprotein(a). 23 Data on whether patients had been fasting were not available in the DC Cohort database, so we opted to focus on non-HDL-C and HDL-C for this analysis, as their measurements are generally more valid in a nonfasting state than those of triglycerides. 24
The two key exposure variables of interest were laboratory results for CD4 cell count and HIV RNA VL. CD4 cell count was categorized as <200, 200–500, or >500 cells/μL, and HIV RNA VL was dichotomized as ≥200 versus <200 copies/mL.
Demographic covariates included age, sex at birth, and race/ethnicity. Smoking history at time of enrollment was categorized as current, previous, or never. Time-updated comorbidities of interest included depression diagnosis, anxiety/stress disorder diagnosis, hypertension (defined by a diagnosis, an antihypertensive medication prescription, or two most recent blood pressure results ≥140/90 mmHg within the last year), diabetes (defined by a diagnosis, an antidiabetes medication prescription, or either two most recent serum glucose results ≥200 mg/dL or two most recent hemoglobin A1c results ≥6.5% within the last year), body mass index (BMI) category, hepatitis C virus (HCV) infection (defined by a diagnosis, reactive HCV antibody test result, positive qualitative RNA test result, or a detectable quantitative RNA VL test result), and chronic kidney disease diagnosis. HIV-specific covariates included HIV transmission category, length of time since HIV diagnosis, history of AIDS diagnosis, and time-updated antiretroviral regimen class, defined using three indicator variables for whether patients were using a protease inhibitor (PI), non-nucleoside reverse transcriptase inhibitor (NNRTI), and/or integrase inhibitor (INSTI). Other time-updated covariates included serum albumin test result and whether patients had a prescription for a lipid-lowering agent (i.e., statin, cholestyramine, fenofibrate, colestipol, ezetimibe, gemfibrozil, or niacin).
Statistical analysis
We used two complementary longitudinal analytic approaches to assess four pairwise associations between HIV measures (CD4 count and HIV VL) and serum lipoprotein concentrations (non-HDL-C and HDL-C).
Primary approach
For the primary analytic approach, repeated cross-sectional measurements of HIV measures and serum lipoprotein concentrations (±14 days of one another) were used to create univariable and multivariable linear regression models using generalized estimating equations (GEE) with robust standard errors, assuming an autoregressive correlation matrix.
Secondary approach
For the secondary analytic approach, area under the curve (AUC) was calculated, based on the trapezoidal rule, 25 for indicator variables for CD4 count and VL categories using all available results during the 3 months preceding each cholesterol test result, serving as cumulative summary measures of the estimated number of days that values were within the aforementioned CD4 count and VL categories during that time period. All cholesterol test results with ≥1 CD4 count test result and ≥1 VL test result available at least 3 months, but no more than 6 months, before the date of cholesterol testing were included in this analysis, so that reasonably accurate weighted starting values for CD4 count and VL could be calculated for the time point exactly 3 months, or 91 days, before the date of cholesterol testing. Each calculated AUC was divided by 91 days so that parameter estimates, also obtained from linear regression modeling with GEE, would be comparable with those obtained from the primary analytic approach. For this analysis, the number of CD4/VL results that contributed to each AUC calculation was 2 for 83.0% of the AUC measures calculated, 3 for 14.4% of the AUC measures, 4 for 2.0% of the AUC measures, and 5–8 for 0.5% of the AUC measures.
Covariate adjustment, interaction terms, and statistical significance
In multivariable models, we adjusted for all covariates identified a priori as potential confounding variables: age, sex, race/ethnicity, HIV transmission group, smoking, depression, anxiety/stress disorder, hypertension, diabetes, BMI, HCV infection, chronic kidney disease, serum albumin, use of a lipid-lowering agent, length of time since HIV diagnosis, history of AIDS diagnosis, and use of PI-based, NNRTI-based, and/or INSTI-based antiretroviral regimens. Results for CD4 count were adjusted for VL, and vice versa. We implemented a Bonferroni correction to account for multiple comparisons, whereby the cutoff for statistical significance was set at p < .0125 for each of the four associations of interest. We also assessed two-way interactions among CD4 count, VL, and age; interaction terms with p < .0125 were retained in multivariable models and subsequent stratified analyses were conducted. If interaction terms were retained in the models created using repeated cross-sectional measurements of CD4 count and HIV VL, then they were also retained in the models created using AUC measures of CD4 count and HIV VL, for comparative purposes, regardless of statistical significance.
Missing data
Missing data, which often resulted from specific fields not having been discretely captured in the EMR, were multiply imputed (10 times) for the HIV transmission group (3% missing), smoking (14% missing), BMI (2% missing), and serum albumin concentration (11% missing). We implemented the fully conditional specification method of multiple imputation, which included the use of the discriminant function method for imputing categorical variables, the logistic regression method for ordinal variables, and the regression method for continuous variables. 26 All statistical analyses were conducted using SAS, Version 9.4 (Cary, NC).
Sensitivity analyses
We conducted several sensitivity analyses. First, all analyses were conducted again with CD4 count and HIV VL defined as continuous variables. For those analyses, HIV VL was transformed to a logarithmic scale and undetectable VL results were coded as a numeric value equal to one unit less than the lower limit of detection. Second, we conducted all analyses that were completed for non-HDL-C again for LDL-C as an outcome variable, as LDL-C is more commonly used in clinical practice as a measure of atherogenic cholesterol and marker of CVD risk. Lastly, to explore the possibility that nonadherence to lipid lowering therapy, which was more commonly prescribed among older patients, might explain age-related differences in associations between CD4 count/HIV VL and non-HDL-C, we also conducted analyses for non-HDL-C only among patients who had no current prescription for any lipid-lowering therapy.
Results
Participant characteristics
Of 6,891 HIV-infected patients aged ≥21 years in the DC Cohort study, 4,467 had at least one non-HDL-C or HDL-C result available; of those patients, 3,912 also had test results available for CD4 count and HIV VL within ±14 days of cholesterol testing. Sociodemographic and clinical characteristics, as of the date of patients' first cholesterol test, are presented in Table 1 for DC Cohort study participants included in this analysis. Characteristics of participants excluded from this analysis are presented in Supplementary Table S1 (Supplementary Data are available online at
Sociodemographic and Clinical Characteristics of Adult HIV-Infected Patients with At Least One Cholesterol Result Available in the DC Cohort Study (n = 3,912)
Values for these time-dependent variables are provided as of the date of patients' first cholesterol test.
Based on the data available in electronic medical records, 10 patients were missing a value for race/ethnicity, 107 patients for mode of HIV transmission, 544 patients for smoking history, 2 patients for recent CD4 cell count, 2 patients for recent HIV viral load, and 67 patients for body mass index.
Antiretroviral regimen categories are not mutually exclusive.
Among patients with hypertension, uncontrolled hypertension was defined as having their two most recent blood pressure results within the last year ≥140/90 mmHg.
IQR, interquartile range; MSM, men who have sex with men; IDU, injection drug use; NNRTI, non-nucleoside reverse transcriptase inhibitor; PI, protease inhibitor; INSTI, integrase inhibitor; HDL-C, high-density lipoprotein cholesterol.
Unadjusted analysis of non-HDL-C
In the unadjusted analysis based on the primary analytic approach (i.e., repeated cross-sectional measurements used for CD4 count and HIV VL), having a CD4 count <200 (vs. >500) cells/μL was associated with a non-HDL-C reduction of −10.8 mg/dL [95% confidence interval (CI): −14.4 to −7.2] (Table 2). Having an HIV VL ≥200 copies/mL was associated with a non-HDL-C reduction of −4.5 mg/dL (95% CI: −6.6 to −2.3). Similar associations were found using the secondary analytic approach (i.e., AUC calculations based on CD4 count and VL results in the 3 months before non-HDL-C testing).
Associations of CD4 Cell Count, HIV Viral Load, Age, and Their Interaction Terms with Non-High-Density Lipoprotein Cholesterol Concentration
Repeated cross-sectional measurements of CD4 count and HIV viral load with non-HDL-C were used in linear regression with generalized estimating equations.
Area under the curve of indicator variables for whether CD4 count results were <200 cells/μL or 200–500 cells/μL and whether HIV viral load results were <200 copies/mL (i.e., 1 for yes, 0 for no) in the 91 days preceding each non-HDL-C result (to estimate the number of days that values were within these categories) was used in linear regression with generalized estimating equations. Each area under the curve was divided by 91, the total number of days, so that the magnitude of each β could be directly compared with the corresponding β obtained based on the primary analytic approach using repeated cross-sectional measurements.
The multivariable model adjusted for CD4 count, HIV viral load, age, the interactions of both CD4 count and HIV viral load with age, sex, race/ethnicity, HIV transmission group, history of smoking, depression, anxiety/stress disorder, hypertension, diabetes, body mass index category, hepatitis C infection, chronic kidney disease, serum albumin, length of time since HIV diagnosis, history of AIDS, current antiretroviral regimen class, and the current use of a lipid-lowering agent.
The interaction term between CD4 count and HIV viral load was removed from the multivariable models due to a lack of statistical significance (data not shown).
CI, confidence interval.
Multivariable analysis of non-HDL-C
After adjusting for potential confounding variables in the two sets of analyses based on primary and secondary analytic approaches, having a CD4 count <200 (vs. >500) cells/μL (p = .0024 and p = .0006, respectively) and an HIV VL ≥200 copies/mL (both p < .0001) remained associated with lower non-HDL-C concentrations (Table 2 and Supplementary Table S2 for results for all covariates). Interaction terms between age and having a CD4 count <200 cells/μL (p = .0030 and p = .0006) and between age and having an HIV VL ≥200 copies/mL (p < .0001 and p = .0001) were also significant based on primary and secondary approaches, respectively; estimated regression coefficients for interaction terms were positive, indicating that associations between CD4 count <200 cells/μL or HIV VL ≥200 copies/mL and non-HDL-C concentration were more positive with increasing age. Interaction terms between having a CD4 count <200 cells/μL (p = .79) or 200–500 cells/μL (p = .65) and having an HIV VL ≥200 copies/mL were not significant based on either approach (these p values are based on the primary approach).
Age-stratified multivariable analysis of non-HDL-C
In subsequent age-stratified analyses based on repeated cross-sectional measurements, the average difference in non-HDL-C associated with having a CD4 count <200 (vs. >500) cells/μL was −7.8 mg/dL (95% CI: −13.2 to −2.4) among patients aged <50 years, +1.4 mg/dL (95% CI: −3.9 to 6.7) among patients aged 50–59 years, +8.1 mg/dL (95% CI: 0.02–16.2) among patients aged 60–69 years, and −14.8 mg/dL (95% CI: −32.6 to 3.1) among patients aged ≥70 years (Fig. 1 and Supplementary Table S3). The average difference in non-HDL-C associated with having an HIV VL ≥200 copies/mL was −3.3 mg/dL (95% CI: −6.7 to 0.1) among patients aged <50 years, −3.3 mg/dL (95% CI: −7.2 to 0.6) among patients aged 50–59 years, +1.4 mg/dL (95% CI: −4.8 to 7.6) among patients aged 60–69 years, and +16.0 mg/dL (95% CI: −1.4 to 33.3) among patients aged ≥70 years. Approximately similar associations by age group were observed in analyses based on AUC measures.
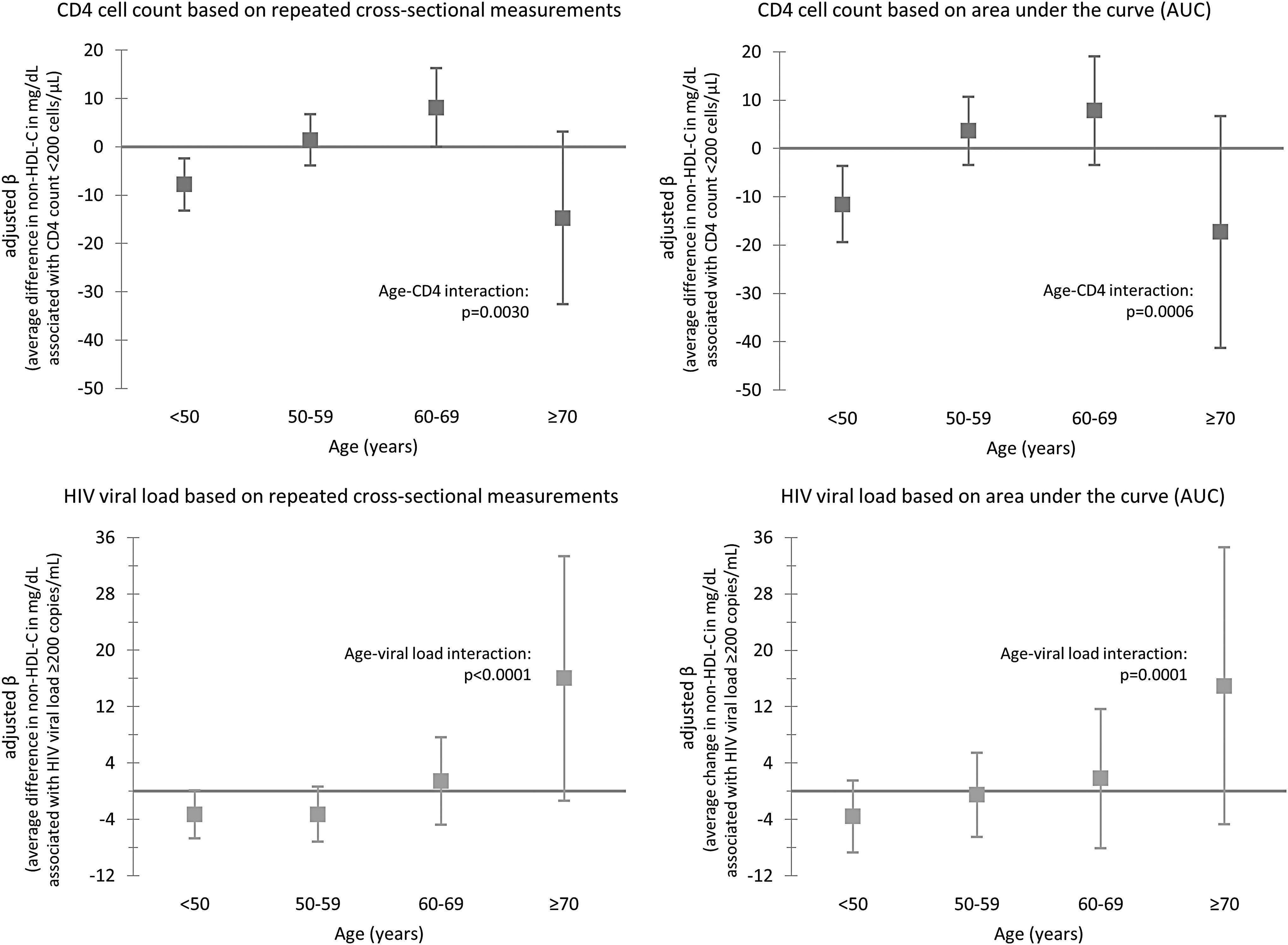
Associations of CD4 cell count and HIV viral load with non-HDL-C concentration by age group. Using multivariable linear regression with generalized estimating equations, all results were adjusted for CD4 cell count, HIV viral load, sex, race/ethnicity, HIV transmission group, history of smoking, depression, anxiety/stress disorder, hypertension, diabetes, body mass index category, hepatitis C infection, chronic kidney disease, serum albumin, length of time since HIV diagnosis, history of AIDS diagnosis, current antiretroviral regimen class, and the current use of a lipid-lowering agent. HDL-C, high-density lipoprotein cholesterol.
Unadjusted analysis of HDL-C
In unadjusted analysis based on the primary analytic approach, having a CD4 count <200 (vs. >500) cells/μL was associated with a reduction in HDL-C of −3.2 mg/dL (95% CI: −4.7 to −1.7) (Table 3). Having an HIV VL ≥200 copies/mL was associated with a reduction in HDL-C of −3.5 mg/dL (95% CI: −4.3 to −2.6). Based on the secondary analytic approach, only having an HIV VL ≥200 copies/mL was significantly associated with a lower HDL-C concentration.
Associations of CD4 Cell Count, HIV Viral Load, Age, and Their Interaction Terms with High-Density Lipoprotein Cholesterol Concentration
Repeated cross-sectional measurements of CD4 count and HIV viral load with HDL-C were used in linear regression with generalized estimating equations.
Area under the curve of indicator variables for whether CD4 count results were <200 cells/μL or 200–500 cells/μL and whether HIV viral load results were <200 copies/mL (i.e., 1 for yes, 0 for no) in the 91 days preceding each HDL-C result (to estimate the number of days that values were within these categories) was used in linear regression with generalized estimating equations. Each area under the curve was divided by 91, the total number of days, so that the magnitude of each β could be directly compared with the corresponding β obtained based on the primary analytic approach using repeated cross-sectional measurements.
The multivariable model adjusted for CD4 count, HIV viral load, age, the interaction between CD4 count and HIV viral load, sex, race/ethnicity, HIV transmission group, history of smoking, depression, anxiety/stress disorder, hypertension, diabetes, body mass index category, hepatitis C infection, chronic kidney disease, serum albumin, length of time since HIV diagnosis, history of AIDS, current antiretroviral regimen class, and the current use of a lipid-lowering agent.
The interaction terms between CD4 count and age and between HIV viral load and age were removed from the multivariable models due to a lack of statistical significance (data not shown).
Multivariable analysis of HDL-C
In adjusted analyses, having an HIV VL ≥200 copies/mL remained associated with lower non-HDL-C concentration based on the primary cross-sectional approach, but not based on the secondary AUC approach (p = .0036 and p = .13, respectively) (Table 3 and Supplementary Table S4 for results for all covariates). Interaction terms between age and having a CD4 count <200 cells/μL (p = .77) or 200–500 cells/μL (p = .35) and between age and having an HIV VL ≥200 copies/mL (p = .43) were not significant based on either approach (these p values are based on the primary approach). The interaction term between having a CD4 count <200 cells/μL and having an HIV VL ≥200 copies/mL was significant based on the primary approach (p = .0013), but not based on the secondary approach (p = .30); the estimated regression coefficient for the interaction term was negative, indicating that simultaneously having a CD4 count <200 cells/μL and HIV VL ≥200 copies/mL was associated with an even lower HDL-C concentration.
Multivariable analysis of HDL-C stratified by CD4 count
In subsequent analyses stratified by CD4 count, the average difference in HDL-C associated with having an HIV VL ≥200 copies/mL was −7.0 mg/dL (95% CI: −9.7 to −4.3) among patients with a CD4 count <200 cells/μL, −4.2 mg/dL (95% CI: −5.9 to −2.6) among patients with a CD4 count between 200 and 500 cells/μL, and −2.2 mg/dL (95% CI: −3.7 to −0.8) among patients with a CD4 count >500 cells/μL, based on repeated cross-sectional measurements (Fig. 2 and Supplementary Table S5).

Association between HIV viral load and HDL-C concentration by CD4 cell count. Using multivariable linear regression with generalized estimating equations, all results were adjusted for age, sex, race/ethnicity, HIV transmission group, history of smoking, depression, anxiety/stress disorder, hypertension, diabetes, body mass index category, hepatitis C infection, chronic kidney disease, serum albumin, length of time since HIV diagnosis, history of AIDS diagnosis, current antiretroviral regimen class, and the current use of a lipid-lowering agent.
Sensitivity analyses
Results did not meaningfully differ when CD4 count and HIV VL were defined as continuous variables (Supplementary Tables S6–S9), when LDL-C instead of non-HDL-C was defined as the outcome variable (Supplementary Tables S10–S13), or when patients who had a current prescription for lipid-lowering therapy were excluded (Supplementary Tables S14 and 15).
Discussion
This epidemiologic study provides novel evidence that associations between CD4 cell count and HIV VL and concentrations of atherogenic cholesterol are modified by one's age. Although immunosuppression and HIV viremia were each independently associated with lower concentrations of non-HDL-C among the full sample of HIV-infected patients, the statistical significance and direction of the interactive effects of both CD4 count and HIV VL with age revealed that the magnitude of these associations was attenuated, and the direction possibly reversed, among older patients. Although the subsequent estimation of age-stratified associations had lower precision as a result of the reduced sample sizes within each age category and the relatively small proportions of patients with a low CD4 count and/or high HIV VL, stratified analyses also largely suggested that the non-HDL-C concentration associated with having a low CD4 count or high HIV VL was higher with increasing age.
Among HIV-infected patients aged <50 years, a low CD4 count was associated with a lower non-HDL-C concentration, whereas there was no association among patients aged 50–59 years; conversely, a low CD4 count was associated with a higher non-HDL-C concentration among patients aged 60–69 years. Results for patients aged ≥70 years did not support a continuation of this trend of CD4 count being associated with higher non-HDL-C concentrations with increasing age, although those results were inconclusive due to a lack of precision. Furthermore, despite a signal that having a high VL was inversely associated with non-HDL-C among patients aged <50 years (and potentially those aged 50–59 years), there was no association among patients aged 60–69 years, and there was a strong positive association among patients aged ≥70 years, although results for HIV VL within each age stratum were not significant. True age-related differences might have been masked in previous studies investigating associations between CD4 count and HIV VL and lipid concentrations. 13,16 –18 In general, similar prior studies included a relatively small number of participants aged ≥60 years, did not report age-stratified results, and/or categorized all patients older than 50 years in the same age group.
Our results might have implications for the risk and progression of dyslipidemia among persons aging with HIV. In our study, older patients with a low CD4 count and especially those with a high VL had higher non-HDL-C concentrations, which is the primary target of lipid-lowering therapy and a strong risk factor for CVD. 23 This finding is concerning because older HIV-infected individuals can face unique barriers to adherence to antiretroviral therapy and non-HIV medications including lipid lowering therapy (e.g., neurocognitive dysfunction and polypharmacy), 27,28 and even modest nonadherence to antiretroviral therapy can cause new cycles of HIV replication. 29
The reasons for observed associations between immunosuppression and viremia and increased concentrations of atherogenic cholesterol among older HIV-infected patients should be further explored. HIV-related pathways such as chronic inflammation and immune system activation may have more strongly altered lipid metabolism in older patients, as uncontrolled viremia is known to promote elevated levels of circulating immune and inflammatory markers associated with atherosclerosis, such as monocyte activation markers and proinflammatory cytokines, and these markers are also associated with aging and age-related disease. 30 –33 In one study, changes to monocyte phenotype and function among young HIV-infected men resembled those found in elderly uninfected adults, suggesting an acceleration of age-related monocyte changes in people with HIV. 34 Age-dependent cholesterol changes might also be explained by a potential cohort effect, as older HIV-infected patients disproportionately included individuals who were infected earlier in the HIV epidemic and have, therefore, experienced greater long-term cumulative exposure to antiretroviral regimens, particularly those with worse metabolic side effect profiles such as PIs. 35 Although data on lifetime exposure to antiretroviral therapy were not available in the DC Cohort database, we did adjust for current antiretroviral regimen and time since HIV diagnosis in our analysis.
We also found that certain covariates predicted one's non-HDL-C concentration. The current use of a PI-based regimen was associated with higher concentrations of non-HDL-C. The association between PI-based regimens and adverse lipid profiles has been well described in the literature. 36 –38 The current use of a lipid-lowering agent was also associated with higher concentrations of non-HDL-C, which was likely due to reverse causality. HCV infection was associated with lower concentrations of non-HDL-C. This finding is consistent with the previously described “protective effect” of HCV coinfection against risk of dyslipidemia in HIV-infected persons, as HIV/HCV-coinfected patients were found to have lower rates of dyslipidemia than HIV-monoinfected individuals in numerous studies. 39 –42
In addition, we found that a high VL was associated with lower concentrations of HDL-C, the type of cholesterol known to protect against CVD. Although that finding is consistent with those of previous studies, 14,17,43 we also detected a significant interactive effect between VL and CD4 count, which has not been reported previously. More specifically, the association between a high VL and decreased HDL-C concentrations was stronger among patients with low CD4 counts. Thus, the potential adverse effect of having uncontrolled viremia on HDL-C concentrations might be more pronounced in the setting of immunosuppression.
This study has several limitations. First, results could have been affected by selection bias as we were only able to include study participants with available cholesterol results and contemporaneous CD4/VL results. Since cholesterol testing is more common in older age groups, patients included in this analysis might have been more likely to have abnormal cholesterol concentrations than those excluded from this analysis. Compared with patients excluded, patients included had a higher median age (3 years older); a greater proportion who were ≥60 years old (3% higher), male (11% higher), and non-Hispanic white (7% higher); and a higher prevalence of diabetes (4% higher). Conversely, patients excluded had a higher prevalence of current smoking (6% higher), hypertension (8% higher), and BMI ≥30 kg/m2 (1% higher). Since differences in age and other major CVD risk factors between patients included and patients excluded were relatively small, we do not expect that our key findings could be primarily attributed to selection bias.
Second, data on fasting status were not available; thus, if any nonfasting samples were used for cholesterol testing, non-HDL-C and HDL-C results may have been affected by measurement error. Future studies, particularly those with lipid measurements based on fasting samples only, should further explore whether similar age-modified associations between CD4 count and VL and triglycerides exist. Third, this analysis included only 89 patients ≥70 years of age and, as a result, our estimates for associations of interest among that age group were imprecise.
Fourth, estimates for associations were based on repeated cross-sectional measurements, which limited our ability to ensure correct temporality of measurements. However, we also used a second analytic approach based on AUC measures, which were calculated using CD4/VL results in the 3 months preceding each cholesterol result. Although limited by a smaller sample size and subsequent reduced precision of estimates, this approach resulted in approximately similar associations, providing some robustness to results. Finally, this study was observational and was, therefore, unable to establish causality. Additional research is needed to confirm our findings and explore potential mechanisms that might explain age-related differences in cholesterol patterns.
This study contributes to our understanding of dyslipidemia among HIV-infected persons, particularly among older individuals. We detected what we believe to be a novel finding, that is, an age-modified relationship between CD4 cell count and HIV VL and concentrations of atherogenic cholesterol. Immunosuppression and viremia were each independently associated with higher atherogenic cholesterol concentrations among older HIV-infected patients, but not among younger patients. We also found that the association between uncontrolled viremia and having lower HDL-C concentrations was stronger when patients had low CD4 cell counts. Taken together, these findings suggest that immunosuppression and viremia might be implicated in the development and progression of dyslipidemia among individuals aging with HIV.
Footnotes
Acknowledgments
We would like to thank the site principal investigators, research assistants, the community advisory board, the patients themselves, the DC Department of Health, and the National Institutes of Health for their contributions to the DC Cohort. This work was supported by the National Institute of Allergy and Infectious Diseases at the National Institutes of Health (NIH) (grant number UM1AI069503). This work was facilitated, in part, by the infrastructure and services provided by the District of Columbia Center for AIDS Research, an NIH-funded program (grant number P30AI117970), which is supported by the following NIH Co-Funding and Participating Institutes and Centers: National Institute of Allergy and Infectious Diseases; National Cancer Institute; Eunice Kennedy Shriver National Institute of Child Health and Human Development; National Heart, Lung, and Blood Institute; National Institute on Drug Abuse; National Institute of Mental Health; National Institute on Aging; Fogarty International Center; National Institute of General Medical Sciences; National Institute of Diabetes and Digestive and Kidney Diseases; and Office of AIDS Research. The content is solely the responsibility of the authors and does not necessarily represent the official views of the NIH.
Data in this article were collected by the DC Cohort Executive Committee with investigators and research staff located at Cerner Corporation (Thilakavathy Subramanian, Jeffery Binkley, Rob Taylor, Nabil Rayeed, Qingjiang Hou, Cheryl Akridge, Stacey Purinton, Jeff Naughton); Children's National Medical Center Adolescent (Lawrence D'Angelo) and Pediatric (Natella Rakhmanina) clinics; The Senior Deputy Director of the DC Department of Health HIV/AIDS, Hepatitis, STD, and TB Administration (Michael Kharfen); Family and Medical Counseling Service (Michael Serlin); Georgetown University (Princy Kumar); George Washington University Medical Faculty Associates (David Parenti); George Washington University Department of Epidemiology and Biostatistics (Anne Monroe, Lindsey Powers Happ, Maria Jaurretche, James Peterson); Howard University Adult Infectious Disease Clinic (Ronald Wilcox), and Pediatric Clinic (Sohail Rana); Kaiser Permanente Mid-Atlantic (Michael Horberg); La Clinica Del Pueblo (Ricardo Fernandez); MetroHealth (Annick Hebou); National Institutes of Health (Carl Dieffenbach, Henry Masur); Providence Hospital (Jose Bordon); Unity Health Care (Gebeyehu Teferi); Veterans Affairs Medical Center (Debra Benator); Washington Hospital Center (Maria Elena Ruiz); and Whitman-Walker Health (Deborah Goldstein, David Hardy).
Author Disclosure Statement
No competing financial interests exist.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.