
Abstract
Mucosal-associated invariant T (MAIT) cell populations are reduced in frequency in HIV-1+ patients, and this disruption is associated with systemic immune activation. Reconstitution of MAIT frequency may benefit HIV-1-infected individuals; however, only recently has in vivo work been endeavored. Treatment with interleukin (IL)-2, granulocyte-macrophage colony-stimulating factor (GM-CSF), and recombinant human growth hormone (rhGH) immunotherapy combined with an HIV-1 vaccine in the context of antiretroviral therapy (ART) has shown to reconstitute CD4 T cell population numbers and function. In this study cryopreserved peripheral blood mononuclear cells (PBMCs) from 12 HIV-1+ patients who were undergoing a combination of HIV-1 vaccine and/or IL-2, GM-CSF and rhGH immunotherapy in conjunction with ART were analyzed to assess the potential of this treatment to promote MAIT cell proliferation. PBMCs were thawed from study baseline, weeks 2 and 48 time points, fluorescently stained for MAIT cell markers, and assessed by flow cytometric analysis. Matched pairs and intergroup results were statistically compared using appropriate methods. MAIT cell frequency was increased from baseline at 48 weeks in participants who received vaccine only, whereas individuals receiving IL-2, GM-CSF, and rhGH immunotherapy with or without vaccine did not show additional benefit. Although IL-2, GM-CSF, and rhGH treatment promotes CD4 T cell reconstitution and HIV-1-specific T cell function, it does not support MAIT cell recovery in patients on suppressive ART. Therapeutic immunization however has a positive effect, highlighting the importance of aiming for balanced promotion of T cell population reconstitution to impact on HIV-1 transmission and pathogenesis.
T
Work exploring MAIT cells in HIV-1 infection before and after antiretroviral therapy (ART) initiation has shown that their frequency is reduced in untreated individuals and demonstrates recovery in the colon but not the periphery under ART. 5,6 Furthermore, remaining peripheral MAIT cells are functionally impaired, with reduced CD69 upregulation, CD107a expression, interferon-γ, tumor necrosis factor, granzyme A and perforin secretion, and increased granzyme B release. 7,8 This impairment and the initial loss of MAIT cells may well contribute to systemic chronic immune activation that often accompanies HIV-1 status. 5
In vitro and in vivo work focusing on reconstitution of MAIT cell frequency and function has shown that interleukin (IL)-7 promotes both recovery and effector function, demonstrating these cells may benefit from immunotherapy. 8,9 Immunization with GTU-MultiHIV clade B DNA vaccine with IL-2, granulocyte-macrophage colony-stimulating factor (GM-CSF), and recombinant human growth hormone (rhGH) has been shown to increase CD4 T cell count, improve HIV-1-specific memory T cell responses, and reduce immune activation in ART-treated HIV-1+ individuals. 10 Here, the potential of this regimen to also reconstitute peripheral MAIT cells is assessed.
Chronically infected HIV-1+ patients older than 18 years of age, maintaining the same ART regimen for ≥6 months with CD4 T cell count >400 cells/μL blood, and plasma HIV-1 RNA <50 copies/mL were recruited from the Chelsea and Westminster Hospital cohort. Participants consented onto the study were not receiving or had received immunomodulatory drugs or therapeutic immunization (
Flow cytometry was performed and MAIT cells were identified as described previously. 5 In brief, monoclonal antibodies to CD3 (Alexa Fluor 700), CD8 (FITC), CD4 (APC-H7), CD38 (APC), CD45RO (BV650), CD161 (PE), and TCR Vα7.2 (BV421) (all Beckton Dickinson, Oxford, United Kingdom), and Aqua live/dead (Amcyan; Thermo-Fisher, Fisher Scientific UK Ltd., Loughborough, United Kingdom) were used for fluorescent staining. CD4 and CD8 memory T cell expression of CD38 was used as a marker of T cell activation. MAIT cell counts were extrapolated from CD3 absolute counts (Supplementary Table S1). Analysis of data was completed using FlowJo V.10.4.1 (FlowJo LLC, Ashland, OR) using unstained and isotype-matched controls to validate gating. Wilcoxon matched-pairs signed rank test, and random intercept model using MIXED procedure in SAS with 95% confidence interval were used to evaluate changes from baseline to weeks 2 and 48 of the study. Correlations were performed using Spearman's rho.
Baseline characteristics of the 12 patients recruited to the study have been described previously. 10 MAIT cells were identified as live CD3+CD45RO+ T cells coexpressing the invariant TCR Vα7.2 together with the C-type lectin CD161 (Fig. 1A). The majority of MAIT cells were CD8 positive (Fig. 1A), and median MAIT frequency of T cells at baseline was 1.49% (range = 0.49%–2.96%). No correlation between MAIT cell frequency and T cell activation, nadir CD4 T cell count or length of time on ART was observed (Fig. 1B).
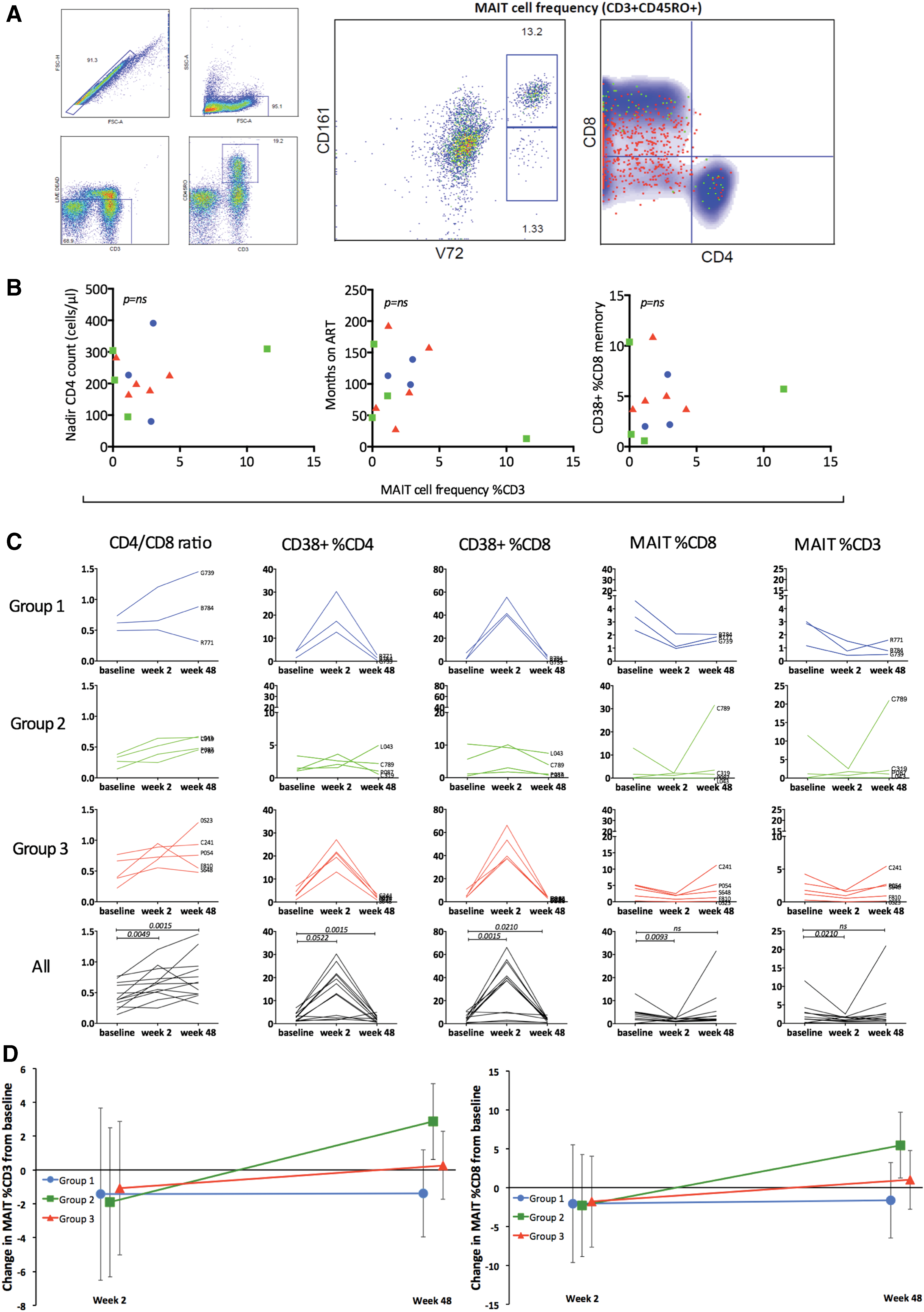
Dynamics of MAIT cells following IL-2, GM-CSF, rhGH, and therapeutic immunization therapy in HIV-1+ participants on ART.
CD4 to CD8 T cell ratio rose significantly at week 2 (p = .002) and was maintained at week 48 (p = .005) compared with baseline in the combined group of patients (Fig. 1C). CD4 and CD8 T cell activation (CD38+) also significantly rose at week 2 from baseline, trailed by a significant decrease in CD8 T cell activation at week 48 (p = .021) in the combined group (Fig. 1C). MAIT cell frequency fell to 0.85% (range = 0.46–1.71, p = .021) at week 2 before rising to 1.32% (range = 0.57–2.64) at week 48 in the combined group (Fig. 1C).
At week 48 only patients randomized to receive IL-2, GM-CSF, and rhGH with vaccine achieved significantly elevated CD4 T cell counts compared with baseline. 10 CD4 T cell CD38 expression was significantly reduced in group 1 (p = .019) and group 3 (p = .025) at week 48 compared with baseline, whereas only group 3 had significantly reduced CD8 T cell activation by week 48 (p = .014). 10 No significant change in CD3 or CD8 MAIT cell frequency was observed at week 48 in patients treated with IL-2, GM-CSF, and rhGH, either with (group 1), or without (group 3) vaccine; however, patients treated with only vaccine (group 2) demonstrated a significant increase (Fig. 1D) with derived MAIT cell counts similarly increasing (Supplementary Table S1 and Supplementary Fig. S1).
Therapeutic administration of IL-2, GM-CSF, and rhGH aids CD4 T cell reconstitution in HIV-1+ patients on ART, 10 although individual participant observations described herein indicate such immunotherapy lacks potency to restore MAIT cell populations. Nevertheless, the significant increase in MAIT cell frequency in the therapeutic vaccine-only individuals and not patients treated with IL-2, GM-CSF, and rhGH indicates this latter strategy of immune stimulation may discriminate against MAIT cell promotion. Theoretically the vaccine response may promote MAIT cell revival through stimulating mechanisms that promote and sustain memory CD8 T cells, whereas adding IL-2, GM-CSF, and rhGH may dampen this process through preferential stimulation of CD4 T cell subsets, potentially regulatory populations, disadvantaging MAIT cell reconstitution. 11
IL-7 therapy has been shown to promote MAIT and other T cell memory subset generation, whereas IL-2, GM-CSF, and rhGH to promote CD4 T cell count and anti-HIV-1 responses. 8 –10 The results of this study suggest that IL-2, GM-CSF, and rhGH therapy boosts CD4 T cell populations, promoting their support of CD8 type-1 T cell function in the absence of proliferation, whereas a vaccine response enables the development of the memory-like MAIT cell populations similar to IL-7. 8 This was reflected in the overall rise of CD4-to-CD8 T cell ratio that was sustained over the course of the study, and the significant decrease in CD8 T cell activation. 10 Being a phase I clinical trial the participant numbers are limited, tissue-resident MAIT cells were not explored, and although MAIT cell frequencies were not restored their function was not assessed. Future immunotherapeutic approaches need to consider balancing promotion of CD4 and CD8 T cell subsets for optimal immunological reconstitution to fully recover unique cell types such as MAIT cells with important roles in HIV-1 pathogenesis and transmission.
Footnotes
Acknowledgments
The immunotherapy trial was funded by the MRC (grant number G0501957), the Westminster Medical School Research Trust, and St. Stephen's AIDS Trust. The authors are grateful to all the patients who took part in the study and to the staff at Chelsea and Westminster Hospital.
The abstract was previously presented at 24th Annual Conference on Retroviruses and Opportunistic Infection, February 13–16, 2017, Seattle, WA.
Author Disclosure Statement
No competing financial interests exist.
Supplementary Material
Supplementary Figure S1
Supplementary Table S1
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.