
Abstract
The limiting-antigen avidity (LAg-Avidity) assay with viral load (VL) >1,000 copies/mL is being used to estimate population-level HIV incidence in Africa. However, this has not been validated in East Africa where HIV-1 subtypes A and D circulate. Sera from persons seen in two surveys (2008–2009 and 2012–2013) limited to those who attended the previous round of the Rakai Community Cohort in Uganda were analyzed. The performance of the current LAg-Avidity protocol, with a mean duration of recent infection (MDRI) of 130 days and false recent rate (FRR) of 0%, was compared with subtype-specific MDRI and FRR, adjusted to subtype distributions. The observed incidence was 1.05/100 person years (py) [95% confidence interval (CI) 0.90–1.23] in 2008–2009 and 0.66/100 py (95% CI 0.52–0.83) in 2012–2013. In contrast, the per-protocol LAg-Avidity incidence estimates were 1.63/100 py (95% CI 0.97–2.30) in 2008–2009 and 2.55/100 py (95% CI 1.51–3.59) in 2012–2013 (a significant increase, p < .05.) However, using a subtype-specific MDRI and FRR, the subtype adjusted incidence was 0.88% (95% CI 0.44–1.33) in 2008–2009 and 0.67% (95% CI 0.00–1.68) in 2012–2013, approximating to the observed incidence trends. In this subtype A/D epidemic, the per protocol LAg-Avidity + VL assay overestimated HIV incidence and failed to detect declines in incidence. Adjustment for FRR, MDRI, and subtype distribution provided incidence estimates similar to empirically observed incidence level and trends. Thus, use of the LAg-Avidity assay in an A/D epidemic requires adjustment for subtype.
Introduction
The limiting-antigen avidity (LAg-Avidity) assay is being used to estimate population-level incidence. 1,2 Population-based HIV Impact Assessments (PHIA) is one application, where HIV incidence is being estimated using LAg-Avidity in 20 President's Emergency Plan For AIDS Relief countries (PEPFAR). 3 The PHIA countries are mainly in southern and Eastern Africa, but also includes Cote d'Ivoire, Cameroon, and Haiti. Although the performance characteristics of the LAg-Avidity have been extensively evaluated, 4,5 its ability to accurately estimate population-level incidence and detect incidence trends remains limited. 6,7
Evaluations of the LAg-Avidity assay include the assay developers, 5,8,9 the Consortium for the Evaluation of HIV Incidence Assays, 4 and other researchers. 6,7,10 Most of these studies included estimates of the mean duration of recent infection (MDRI) and the false recent rate (FRR). 11 However, studies show a longer MDRI and higher FRR with subtype D 12 than other subtypes. Few studies have directly compared incidence observed in a longitudinal cohort with that estimated by a testing algorithm using LAg-Avidity. 6,7 We evaluated the current per protocol LAg-Avidity + viral load (VL) algorithm with an MDRI of 130 days and FRR of 0% 13 to estimate the level and change in observed incidence in rural Rakai district, Uganda, where HIV-1 subtypes A and D circulate. 14,15 We also assessed the effects of adjustment for subtype-specific MDRI and FRR.
Materials and Methods
Ethics statement
The study was approved by the National Institute of Allergy and Infectious Diseases, Johns Hopkins Medical Institutions, Western IRB (Olympia, WA), the Research and Ethics Committee of the Uganda Virus Research Institute, and the Uganda National Council for Science and Technology Institutional Review Boards. This study is registered on
Study design and participants
Samples were from the Rakai Community Cohort Study (RCCS), which is an open population cohort study of participants aged 15–49 years in rural Rakai district, Uganda. 15 Samples from surveys in June 2008 to December 2009 and August 2011 to May 2013 were tested by the LAg-Avidity assay. The population was drawn from trading and agrarian villages and only included participants observed in a prior survey round. In 2008–2009 there were 9,973 individuals surveyed who were observed in the previous round (Fig. 1). Among initially HIV-negative participants there was 15,212 person years (py) of observation and 161 seroconverters with an incidence of 1.05/100 py [95% confidence interval (CI) 0.90–1.23]. A total of 1,083 individuals were HIV positive at the previous round and 358 (28.8%) self-reported that they were on antiretroviral therapy (ART). In 2012–2013 survey round, there were 6,751 participants seen in the previous round of whom 914 were HIV positive in both rounds, 73 seroconverted, and 5,764 remained HIV seronegative. Of the 987 HIV-positive subjects, 423 were on ART (42.9%). Among 5,837 initially HIV-negative participants, 73 seroconverted for 11,006 years follow-up with an observed incidence of 0.66/100 py (95% CI 0.52–0.83).
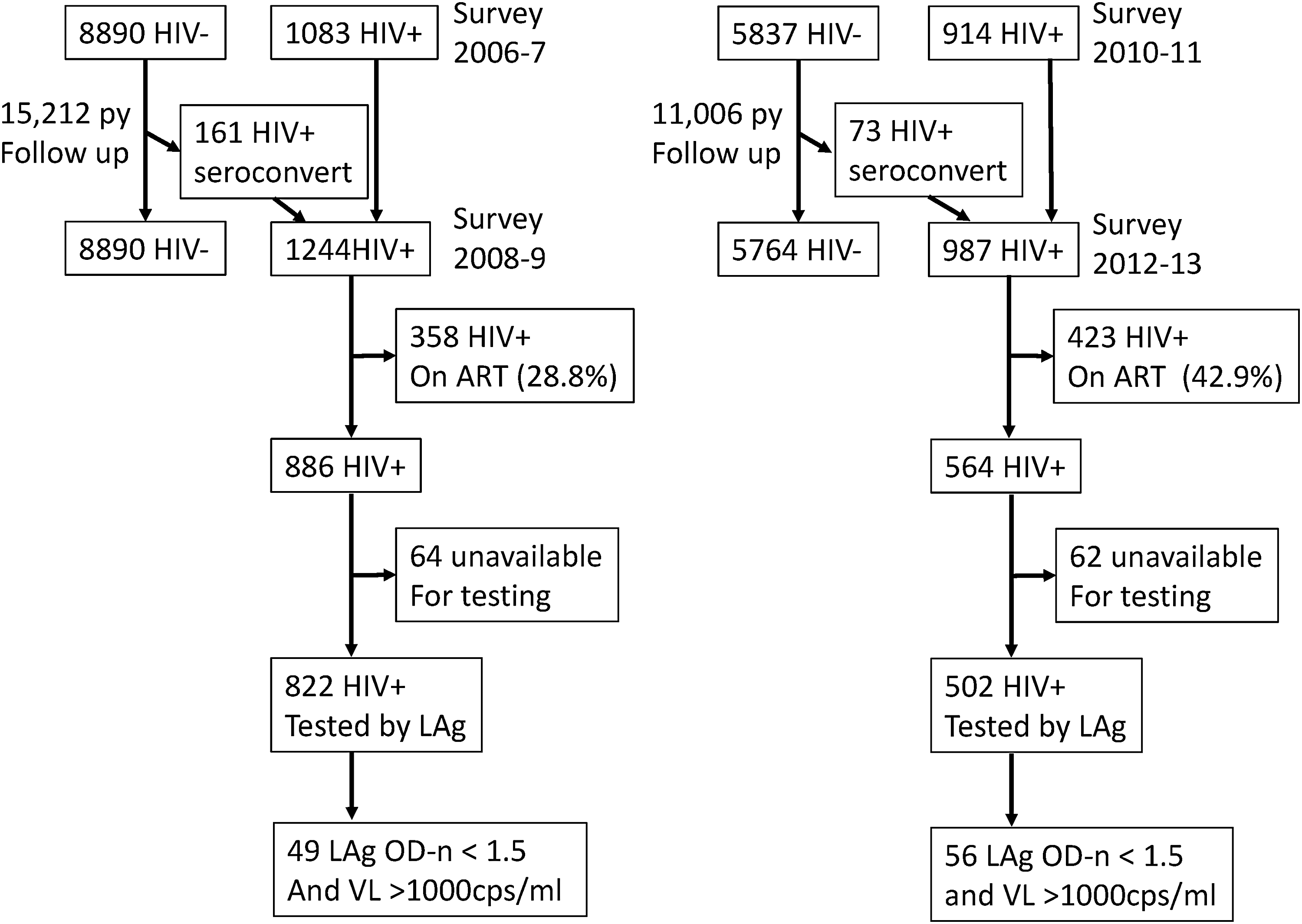
Flowchart of cohorts tested. py, person years; LAg-Avidity, limiting-antigen avidity; OD-n, normalized optical density; cps, copies.
Sample testing and incidence estimation
LAg-Avidity testing was performed according to the manufacturer's instruction
13
on all HIV seropositive samples from subjects who were not on self-reported ART. Subjects on ART were considered to be long-term infected given the CD4 criteria for ART initiation pertaining at that time. We estimated cross-sectional incidence from an algorithm based on an LAg-Avidity <1.5 normalized optical density (OD-n) and a VL >1,000 copies/mL, which were classified as recently infected, using an MDRI of 130 days and an FRR of 0%. We also calculated incidence using an MDRI specific for the population subtype distribution of 45% A and 55% D based on sequencing of the gp41 region.
16
This portion of gp41 contains the peptide used in the LAg-Avidity assay.
5
The calculated subtype-specific MDRI was 187 days
17
and the FRR was recalculated for each survey round. Cross-sectional incidence estimates and measures of differences in observed incidence were calculated using the interactive excel workbook ABIE v3.0 incidence calculator available at:
Results
In 2008–2009, 822/886 samples from HIV-positive individuals not on ART were available for testing with LAg-Avidity assay. Sixty-nine had an OD-n <1.5 and 49 of these had a VL >1,000 copies/ml. Of the 544 samples from subjects known to be infected >2 years, 6 had LAg-Avidity <1.5 OD-n and a VL >1,000 copies/mL for a round-specific FRR of 1.1%. The estimated incidence using a per protocol MDRI of 130 days and an FRR of 0% was 1.63/100 py (95% CI 0.97–2.3). Using a subtype adjusted MDRI of 187 days and an FRR of 1.1%, the estimated incidence was 0.88/100 py (95% CI 0.44–1.33), which was similar to the observed incidence of 1.05/100 py (95% CI 0.90–1.23) (Fig. 2).
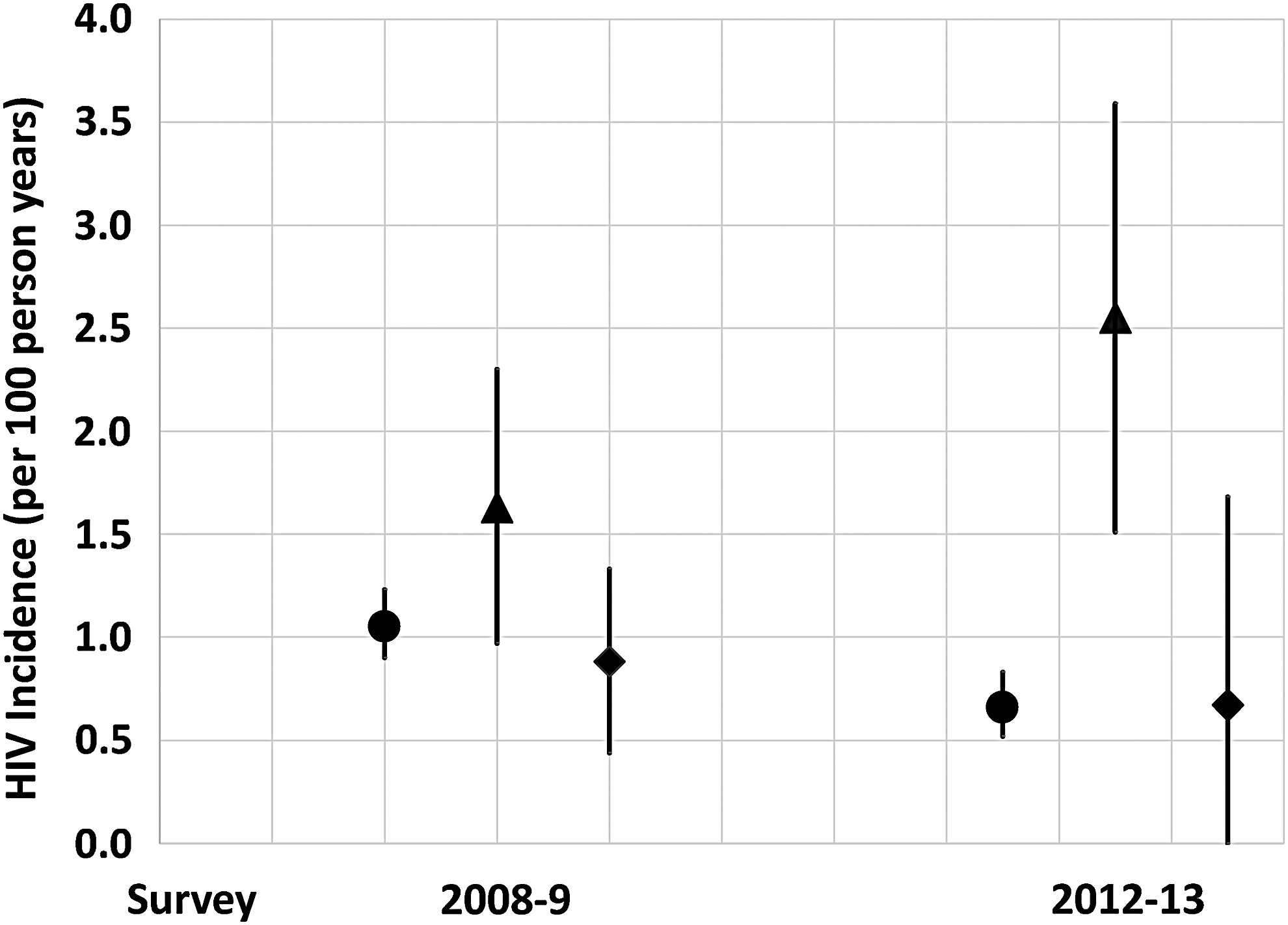
Comparison of observed HIV incidence with that estimated by LAg-Avidity protocols. Observed incidence are marked with circles. The per protocol incidence (mean duration of recent infection of 130 days and an FRR of 0%) estimates are marked with triangles. The estimates generated with a subtype-specific mean duration of recent infection and a round-specific FRR are marked with diamonds. Confidence intervals are shown for all estimates. FRR, false recent rate.
In 2012–2013, 500/562 samples from HIV-positive individuals not on ART were tested by LAg-Avidity. Eighty-four had a <1.5 OD-n, and of those, 56 had a VL >1,000 copies/mL. There were 332 samples from individuals infected >2 years and 16 were misclassified as recent (FRR 4.8%). Of 332, 247 had subtype data available. Misclassification was significantly higher in subtype D (14/138, FRR = 10.1%) than subtype A (0/97) or C (0/12) p < .05. Using the per protocol MDRI and FRR values of 130 days and 0%, respectively, the estimated incidence was 2.55/100 py (95% CI 1.51–3.59). Using the subtype-specific MDRI of 187 days and an FRR of 4.8%, the estimated incidence was 0.67/100 py (95% CI 0.0–1.68), which was nearly identical to the observed incidence of 0.66/100 py (0.52–0.83).
When measuring an incidence difference between the rounds, the per protocol method suggested an increase in incidence of 1.28/100 py (95% CI 2.25–0.31, p < .001). In contrast, using the subtype adjusted MDRI of 187 days and a round-specific FRR, there was a 35% (95% CI −0.68 to 1.37) nonsignificant decrease in incidence, which is close to the 37% decrease in incidence observed in the longitudinal cohort data.
As a sensitivity analysis we compared incidence with only the 40 communities surveyed in both surveys. In 2008–2009, this subset included 5,057 subjects, 710 who were HIV infected, and 454/486 subjects not on ART had samples for testing. Among the initially HIV uninfected individuals there was 7,610 years of follow-up and 93 seroconverters for an estimated incidence of 1.2/100 py (95% CI 0.99–1.5). Among the 486 HIV-positive subjects not on ART, 24 had LAg-Avidity <1.5 and a VL >1,000 copies/mL. Using the per protocol methodology the incidence estimate was 1.6/100 py (95% CI 0.78–2.3) and the subtype adjusted incidence estimate was 0.9/100 py (95% CI 0.35–1.4).
Discussion
This study demonstrated that the per protocol use of LAg-Avidity + VL overestimated HIV incidence in a subtype A and D epidemic, and incorrectly estimated an increase in incidence between the two survey rounds, when the empirically observed incidence decreased in the longitudinal cohort data. In contrast, using a subtype adjusted MDRI and a round-specific FRR, incidence estimates using an LAg-Avidity + VL algorithm produced near identical incidence estimates to those observed longitudinally and showed a decrease in incidence between the survey rounds.
Of greatest concern is the variability in FRR between surveys. In round 2008–2009, 1.1% of the known long-term infected individuals were misclassified as recent, whereas in 2012–2013 the FRR was 4.8%, although the confidence intervals of these point estimates overlap. One possible reason is that there was near a doubling of ART coverage between those two survey rounds in the cohort. 15 We have previously shown that there is under-reporting of ART in the RCCS, particularly among younger people who were more likely to be on ART in the later survey round. 18 Also the observed decrease in HIV incidence would increase the proportion of HIV-positive individuals with long-term infection, which could exacerbate the FRR. More research is necessary to determine an appropriate FRR for declining HIV epidemics in sub-Saharan Africa and what affects the variation of FRR over time. Future work should include studies in other regions with different subtype distributions, ideally in samples from population-level cohorts with observed incidence.
In conclusion, the per protocol use of the LAg-Avidity assay does not accurately estimate HIV incidence in Uganda where subtypes A and D circulate. The per protocol analysis overestimated the observed incidence and suggested an increase in incidence over time, whereas a decline in incidence was observed in the longitudinal data. Our results suggest that population-based cross-sectional surveys of HIV incidence, including PEPFAR's PHIA surveys, will need to use survey-specific FRRs and subtype-specific MDRIs in African HIV epidemics with circulating subtype D infections such as in Uganda.
Footnotes
Acknowledgments
This research was supported by the National Institute of Mental Health (R01MH107275), the National Institute of Allergy and Infectious Diseases (5R01 AI095068, 1R01AI128779-01, R01AI110324, K01AI125086), and Division of Intramural Research of the National Institute for Allergy and Infectious Diseases, the World Bank, and the Johns Hopkins University Center for AIDS Research (P30AI094189). This work was also supported (in part) by the HIV Prevention Trials Network (HPTN) sponsored by the National Institute of Allergy and Infectious Diseases (NIAID), National Institutes of Child Health and Human Development (NICH/HD), National Institute on Drug Abuse, National Institute of Mental Health, and Office of Aids Research, of the NIH, DHHS (UM1 AI068613). We also thank the Rakai Community Cohort Study participants and study team.
Author Disclosure Statement
No competing financial interests exist.