
Abstract
A rise in new HIV diagnoses among older adults is characterized by poor prognosis and reduced survival times. Although heterosexual transmission remains the main route of infection in women, little is known regarding immune functions in the genital tract of postmenopausal women, especially those who are HIV positive. Furthermore, effects of hormone replacement therapy (HRT) on the genital tract immune system are unclear. Using the Women's Interagency HIV Study repository, we obtained cervical–vaginal lavage (CVL) samples from premenopausal and postmenopausal HIV-positive and HIV-negative women, some of whom were on HRT. Samples were assayed for interleukin (IL)-6, IL-8, tumor necrosis factor (TNF)-α, secretory leukocyte protease inhibitor (SLPI), Elafin, human beta defensin-2 (HBD2), and macrophage inflammatory protein (MIP)-3α using ELISA. Anti-HIV activity in CVL was measured using TZM-bl indicator cells. Among HIV-positive women, the plasma viral load was significantly higher and CD4 count was significantly lower in postmenopausal compared with premenopausal women. Postmenopausal women, irrespective of HIV status, had significantly lower levels of HBD2 compared with premenopausal women. Among the HIV-negative individuals, postmenopausal women had significantly lower levels of MIP-3α, IL-6, and SLPI compared with premenopausal women. In contrast, HIV-positive postmenopausal women had significantly higher levels of TNF-α compared with HIV-positive premenopausal women. In most cases, HRT groups resembled the postmenopausal groups. No significant differences in anti-HIV activity by menopausal or by HIV status were noted. Our findings indicate that the female genital tract immune microenvironment is distinct by menopausal status and HIV status. Further studies are needed to assess the risk of HIV acquisition/transmission in this population.
Introduction
Rates of new HIV
The HIV/AIDS epidemic affects women disproportionately. 7 As HIV/AIDS is often perceived as a condition impacting reproductive-age women, most epidemiological studies do not focus on older women. Therefore, little is known regarding the immunological mechanisms of HIV susceptibility in postmenopausal women and even less so in the HIV-positive population.
It is known that aging is associated with a gradual weakening of immune responses, along with a systemic increase in inflammation (reviewed 8 –10 ). In postmenopausal women, chronic systemic inflammation, characterized by higher levels of proinflammatory cytokines and reduced ability to respond to pathogenic stimuli, has been described. 11 –13 Less is known regarding immune functions in the female genital tract (FGT), which are critical to consider to prevent sexual acquisition/transmission of HIV. Ex vivo infection studies using cervical hysterectomy or biopsy samples have reported greater inflammation/immune activation, 14,15 along with higher production of HIV p24 upon infection. 14,16 We and others have previously shown reduced levels of soluble immune mediators in genital secretions among postmenopausal women compared with premenopausal women. 16 –18 As many of these immune mediators are reported to be regulated by estradiol, 19,20 reduction following menopause is not surprising. However, it is less clear as to what extent this reduction affects overall functional immunity in the FGT.
Little is known regarding the immune microenvironment of postmenopausal women who are HIV positive. We have previously demonstrated increased inflammatory response, decreased levels of endogenous antimicrobials, and decreased functional anti-HIV activity in the FGT of HIV-positive premenopausal women. 21,22 Rodriguez-Garcia et al. reported increased CCR5+ expression in Th17 cells in the FGT of postmenopausal women, along with a trend toward higher HIV infectivity. 23 Clinically, the data are conflicting on whether HIV-positive women undergo premature menopause and whether effectiveness of HAART is reduced in this population. 24
Hormone replacement therapy (HRT) (either estrogen or estrogen/progestin combination) is currently used by women to relieve menopausal symptoms, mostly as a topical treatment. 25 Studies have demonstrated that HRT can be useful in partially reversing the deleterious aging-associated effects on systemic immune responses (reviewed 8 ). In particular, a recent longitudinal study where postmenopausal women used topical HRT (vaginal estradiol cream) demonstrated improvement in FGT immune parameters after 1 month of use. 16 However, the impact of systemic HRT on FGT immune responses is unknown.
To address the gaps in knowledge described above, our study investigated levels of soluble immune mediators and functional anti-HIV activity in cervical–vaginal lavage (CVL) samples from HIV-negative and HIV-positive premenopausal, postmenopausal, and postmenopausal women on HRT. We hypothesized that postmenopausal women will have an altered FGT immune microenvironment, which will be further distinct in the HIV-positive group. Furthermore, we hypothesized that levels of some of the critical immune mediators will be similar among women in the premenopausal group and the postmenopausal women using HRT.
As the population of HIV-positive postmenopausal women and HIV-negative at-risk postmenopausal women is on the rise, understanding immune responses in the FGT is of critical importance so that specific prevention/intervention strategies can be designed for this emerging high-risk population.
Materials and Methods
Ethical statement
The Women's Interagency HIV Study (WIHS) protocol and this study were conducted according to the principles expressed in the Declaration of Helsinki. After approval by the participating institution's review board, study staff obtained written informed consent for collection and use of data and specimens from each research participant. George Washington University only had access to deidentified information.
Cohort characteristics and demographics
WIHS is an ongoing, prospective, observational cohort study of HIV-infected and sociodemographically similar uninfected women in the United States. Study methods, baseline cohort characteristics, and long-term retention have been previously described. 26 –28 Briefly, semiannual visits included an interview for collection of demographic, behavioral, and clinical factors and a physical and gynecologic examination with specimen collection for the repository. For this cross-sectional study, samples were provided by the Washington DC site. In the premenopausal category, we identified 30 HIV-negative and 30 HIV-positive women who were <45 years of age at visit and experiencing regular menstrual cycles. The cycle stage was determined based on self-reported timing of the last menstrual period (LMP). In the postmenopausal category, we identified 29 women in both HIV-negative and HIV-positive groups who were >45 years of age at visit and had no menstrual cycle for at least 1 year. Women on HRT (5 HIV-negative and 7 HIV-positive women) were on estrogen, progesterone, or combination therapy for at least the past 6 months. To characterize FGT immune condition in the absence of antiretroviral therapy (which can act as a confounder), we selected only those HIV-positive women who were not using any antiretroviral drugs for at least the past 6 months. Women were excluded if currently pregnant, breastfeeding, or lacking a cervix as a result of hysterectomy. Information on race/ethnicity, menstrual cycle staging, birth control usage (for premenopausal women), presence of reproductive tract infections (RTIs) or dysbiosis (Trichomonas vaginalis, herpes simplex virus, bacterial vaginosis, Candida albicans, Neisseria gonorrhea, or Chlamydia trachomatis), plasma viral loads (PVLs), and CD4 counts was obtained for all women from the WIHS database. CVL viral load data were also collected, but as almost 100% of the women had undetectable values, this parameter was not used in any analyses.
CVL processing
Previously frozen whole CVL was shipped on dry ice from the WIHS repository, thawed on ice, and processed immediately. The CVL was spun at 1,500 × g for 10 min, supernatant removed, and respun at 2,200 × g for 10 min. Supernatants were aliquoted and frozen at −80°C.
HIV viral stocks
HIV strains, IIIB (CXCR4 tropic) and BaL (CCR5 tropic), were obtained from Dr. P. Gupta (University of Pittsburgh, PA). Virus stocks were propagated in phytohemagglutinin (PHA)-stimulated human peripheral blood mononuclear cells (PBMCs) and stored frozen at −80°C. Virus titers were determined on TZM-bl cells.
Measurement of cytokines, chemokines, and antimicrobials in CVL
CVL supernatants were stored at −80°C until assayed for tumor necrosis factor (TNF)-α, interleukin (IL)-6, IL-8, macrophage inflammatory protein (MIP)-3α, secretory leukocyte protease inhibitor (SLPI), Elafin ELISA (R&D Systems, Minneapolis, MN), and HBD2 ELISA (PeproTech, Rocky Hill, NJ). Quantification was based on standard curves obtained using a microplate reader (Biotek, Winooski, VT). Concentrations below the lower limit of detection were set to the midpoint between 0 and the lowest detected value for that particular target and adjusted for dilution.
Determination of total protein concentration in CVL
Total protein concentration in each CVL sample was determined using the Pierce BCA Protein Assay kit (Thermo Fisher Scientific), according to the manufacturer's instructions. Concentrations of immune mediators were normalized to total protein content of the CVL.
Measurement of anti-HIV activity in CVL
Anti-HIV activity in the CVL was determined using the TZM-bl indicator cell line (AIDS Reagent Repository, NIH) essentially as previously described. 18,29 Samples (tested in triplicates) were incubated with HIV IIIB and BaL at 250 tissue culture infectious dose (TCID50) for 1 h at 37°C and added to TZM-bl cells. Luciferase activity was measured in 48 h upon application of substrate beta-Glo (Promega, Madison, WI).
Viability of cells upon treatment with CVL was quantified using the CellTiter 96® AQueous One Solution Cell Proliferation Assay (Promega), as previously described. 18
Statistical analyses
Possible covariates that can affect immune biomarkers in the context of our study of interest were compared across the six groups, separately by HIV status. The median values of each biomarker were compared by group using Kruskal–Wallis tests. For biomarkers with significant differences in medians, graphs were created using GraphPad Prism with Mann–Whitney U tests comparing each group with the control.
Heat maps for each group were constructed to assess the direction and strength of associations between individual biomarkers and other functional and clinical variables such as HIV inhibition, CD4, and PVL data by performing Spearman's rank-order correlation tests using R Studio, version 1.0.136.
Results
Higher PVL and lower CD4 counts in postmenopausal women
Study participants did not differ significantly in terms of race, RTIs, contraceptive use, and menstrual cycle stage (Table 1). However, HIV-positive postmenopausal women and postmenopausal women on HRT had significantly higher PVLs compared with HIV-positive premenopausal women (Fig. 1A and Table 1). Postmenopausal women also had significantly lower CD4 counts compared with premenopausal women (Fig. 1B and Table 1).
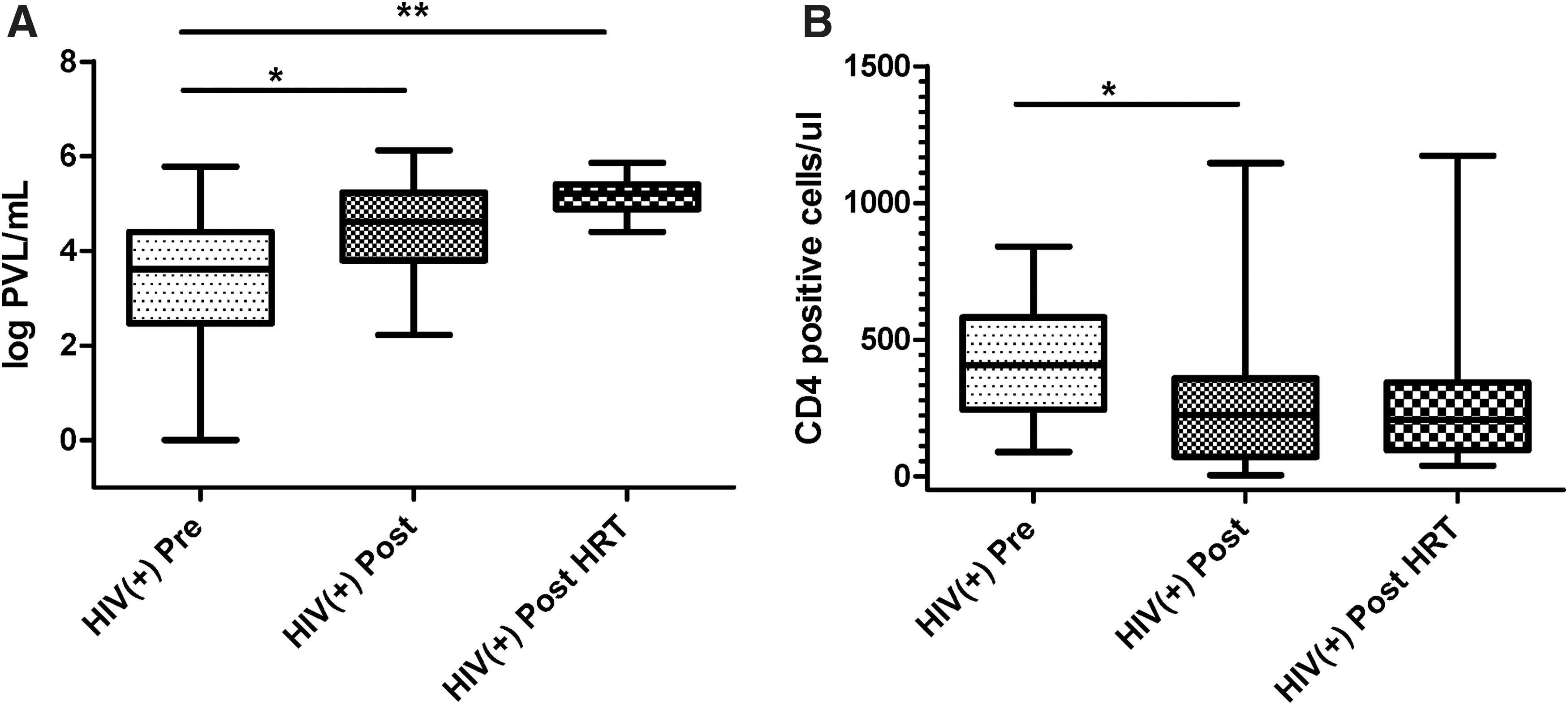
Higher PVLs and lower CD4 counts in HIV-positive postmenopausal women. Data on PVLs
Participant Characteristics Among HIV-Negative and HIV-Positive Premenopausal, Postmenopausal, and Postmenopausal Women on Hormone Replacement Therapy
All values are “at visit.” None of the HIV-positive women were on ARV for at least the past 6 months.
Data presented as mean ± SEM.
Data presented as N (%).
Hormonal contraceptive in past 6 months.
ARV, antiretroviral; N/A, not applicable; ns, nonsignificant; Pre, premenopausal; Post, postmenopausal; Post+HRT, postmenopausal women on hormone replacement therapy.
Distinct levels of soluble immune mediators in CVL by menopausal status and HIV status
To determine whether levels of immune mediators were distinct in genital tract secretions by menopausal or by HIV status, we analyzed CVL samples for proinflammatory mediators IL-6, IL-8, and TNF-α and anti-HIV/protective mediators MIP-3α, SLPI, Elafin, and human beta defensin-2 (HBD2).
When analyzed by menopausal status, HIV-negative postmenopausal women had significantly lower levels of IL-6, MIP-3α, HBD2, and SLPI compared with HIV-negative premenopausal women (Fig. 2A, C–E and Table 2). For MIP-3α, postmenopausal women on HRT also had significantly lower levels compared with premenopausal women. Within the HIV-positive groups, postmenopausal women had significantly lower HBD2 compared with premenopausal women (Fig. 2D and Table 2) and postmenopausal women on HRT had significantly lower MIP-3α compared with premenopausal women (Fig. 2C and Table 2). In contrast, postmenopausal women had significantly higher levels of TNF-α compared with both premenopausal women and postmenopausal women on HRT (Fig. 2B and Table 2).

Differences in cervico–vaginal immune mediators by menopausal status in HIV-negative and HIV-positive women. CVL from HIV-negative and HIV-positive premenopausal, postmenopausal, and postmenopausal women on HRT were tested for
Immune Parameters in Cervical–Vaginal Lavage from HIV-Negative and HIV-Positive Premenopausal, Postmenopausal, and Postmenopausal Women on Hormone Replacement Therapy
Significant p-values are denoted in bold.
All values are “at visit.” None of the HIV-positive women were on ARVs for at least the past 6 months. p value adjusted: normalized to total protein levels for a given sample and a given mediator.
CVL, cervical–vaginal lavage; HBD2, human beta defensin-2; IL, interleukin; IQR, interquartile range; MIP-3α, macrophage inflammatory protein-3 alpha; SLPI, secretory leukocyte protease inhibitor; TNF, tumor necrosis factor.
When analyzed by HIV status, IL-6 levels were significantly higher in premenopausal HIV-negative women compared with premenopausal HIV-positive women (Fig. 2A and Table 2). However, TNF-α and MIP-3α were at significantly higher levels in postmenopausal HIV-positive women compared with postmenopausal HIV-negative women (Fig. 2B, C and Table 2).
IL-8 levels were measurable, but did not vary significantly among groups by menopausal or HIV status (Table 2).
Total protein concentration in CVL did change significantly between the groups with a trend toward higher values in HIV-positive samples (Table 1). All mediators that were significantly different among groups before protein adjustment remained so following protein adjustment. The one exception was Elafin, which was nonsignificant before adjustment, but became significant after adjustment, with significantly higher levels in samples from HIV-negative premenopausal and postmenopausal women compared with those from HIV-positive premenopausal and postmenopausal women (Table 2).
Anti-HIV activity in CVL
Intrinsic anti-HIV activity in CVL samples from HIV-positive and HIV-negative women has been previously demonstrated. 21,30,31 To determine whether women have differential anti-HIV activity based on menopausal and/or HIV status, we tested the CVL against HIV-1 IIIB and BaL using the TZM-bl indicator cell line. All HIV-positive women were not on HAART for at least 6 months before sampling visit, thereby giving us the opportunity to characterize anti-HIV activity in the absence of drugs. A wide range of anti-HIV activities were detected in all groups, but no significant differences were present (Table 2).
Correlations among immune mediators, anti-HIV activity, and clinical parameters
Whereas ELISA-based assays determine levels of mediators, associations between immune mediators and clinical parameters are also critical for understanding underlying mechanisms. Distinct associations and clustering of immune mediators have been described previously in the context of HIV infection and susceptibility. 32 We and others have previously reported distinct immune clustering in adolescent cohorts as well as premenopausal versus postmenopausal women. 18,33 In the current study, we observed distinct immune clustering patterns among the six groups (Fig. 3). In particular, HIV-positive groups showed greater numbers of significant interactions. CD4 counts showed significant positive interactions with the proinflammatory cytokine TNF-α in premenopausal and postmenopausal groups. However, this interaction was not observed in the HIV-positive HRT group, which is suggestive of a nonimmune-activated phenotype. In fact, in this group, TNF-α showed significant negative associations with anti-inflammatory mediators, Elafin and HBD2. HRT groups in both HIV-positive and HIV-negative categories showed the least number of significant interactions.

Heat map showing distinct correlations between cervico-vaginal immune mediators, clinical parameters, and anti-HIV activity against HIV IIIB and BaL for
Discussion
Our study evaluated the presence of soluble immune mediators and anti-HIV activity in genital tract secretions of HIV-negative and HIV-positive premenopausal and postmenopausal women. Our results indicate significant alterations in immune mediators in CVL both by menopausal status and HIV status.
We and others have previously shown lower levels of several critical immune mediators in CVL samples from healthy, HIV-negative postmenopausal women compared with premenopausal women. 16 –18 Our current data extend these findings and confirm similar patterns for most mediators that we tested in HIV-positive women who have not been on antiretroviral therapy at least for the past 6 months. Two of these immune mediators, SLPI and HBD2, have in vitro anti-HIV functions. 34 –36 Therefore, their reduction can potentially result in decreased immune protection in the FGT. Another mediator, MIP-3α, has also been shown to have anti-HIV activity in vitro and therefore reduced levels in postmenopausal women might be detrimental. 37 However, MIP-3α has also been shown to enhance HIV infection in genital mucosa by attracting target cells 38 and its precise in vivo role in these women cannot be determined from the current study.
Our data showing significant reduction of IL-6 in CVL samples of HIV-negative postmenopausal women compared with premenopausal women confirm our findings in previous publications. 18 In HIV-positive women, TNF-α levels were higher in postmenopausal compared with premenopausal women. This suggests that specific inflammatory pathways are upregulated in postmenopausal HIV-positive women not currently on antiretroviral therapy and this effect is not observed in premenopausal HIV-positive women. This observation, combined with significantly higher PVLs and lower CD4 counts in the HIV-positive postmenopausal group, indicates inflammatory immune dysregulation in the FGT.
HRT is used by postmenopausal women to relieve menopausal symptoms, both systemically and more frequently as a topical cream or gel. We hypothesized that postmenopausal women using HRT will have an improved outcome of FGT mucosal variables compared with those not using HRT. However, in our study, the HRT groups looked very similar to non-HRT postmenopausal groups in terms of levels of immune mediators and PVL/CD4 values. The exception was TNF-α for HIV-positive women, where levels in postmenopausal women were significantly higher compared with levels in premenopausal and postmenopausal women on HRT. Interestingly, by heat map analysis, we did see few significant associations between immune mediators and clinical parameters in the two HRT groups, with samples from HIV-negative women receiving HRT demonstrating the least number of associations. This pattern points toward an immune nonreactive phenotype. Thurman et al. recently reported 16 improvement of mucosal outcomes upon treatment with vaginal estradiol. It is possible we did not see any effects because HRT usage in our cohort differed in terms of route (oral vs. topical) and regimen (estradiol, progesterone, or combination of both) and the sample sizes were particularly small.
Our data from this study showed significant differences in CVL protein concentration among groups. We have previously reported no significant changes in this parameter between premenopausal and postmenopausal HIV-negative women. 18 Upon closer examination, it was revealed that CVL protein concentration was not significantly different within the HIV-negative groups, confirming our previous findings. The driver for the observed significant changes was the presence of higher levels of protein in HIV-positive postmenopausal samples compared with HIV-negative postmenopausal samples.
We observed a range of anti-HIV activities in all samples, but no significant differences between groups. This is consistent with previous findings in HIV-negative premenopausal and postmenopausal women. 16,18 One study 39 did report lower CVL anti-HIV activity in postmenopausal women compared with premenopausal women. However, this differs from our findings likely because different cell lines and experimental conditions were used in that study. We have previously demonstrated a range of anti-HIV activities in CVL samples from HIV-positive women who were not on HAART. 21
There were several limitations to our study. One was our inability to define menopause by measuring estradiol/progesterone levels in blood. However, we used clinical criteria for defining menopause: at least 1 year of no menses, 40 and it is likely that our postmenopausal women were categorized correctly. However, from this study, we cannot be certain whether our findings in postmenopausal women are attributable to chronological aging or biological aging (i.e., menopause). Similarly, we were unable to accurately determine the cycle stage in premenopausal women and were limited by a rough analysis of self-reported LMP. Other critical mucosal parameters that can affect HIV acquisition/transmission risks are the presence of RTI and contraceptive usage. 41 Our cohort had a very small number of women with RTIs in all the groups and only 4 (of total 60 premenopausal women) were on contraceptives (all on progestin-only Depo-provera regimen). Therefore, with such small numbers, we were unable to adjust for these parameters and decided to not exclude them so as to not reduce the sample size further. Future studies with larger sample sizes should take these factors into account.
To our knowledge, this is the first study to characterize FGT immune mediators in HIV-negative and HIV-positive premenopausal and postmenopausal women. Our data suggest that immune alterations occur in the FGT based on both menopausal status and HIV status. Additional studies with larger sample sizes are warranted to understand the mechanisms underlying these changes.
Footnotes
Acknowledgments
The authors would like to thank Dr. Charles Wira and his group at Geisel School of Medicine at Dartmouth for advice on data analysis and manuscript writing. Data in this article were collected by the Metropolitan Washington Women's Interagency HIV Study (WIHS) (Principal Investigator, Dr. Seble Kassaye), U01-AI-034994. The WIHS is funded primarily by the National Institute of Allergy and Infectious Diseases (NIAID), with additional cofunding from the Eunice Kennedy Shriver National Institute of Child Health and Human Development (NICHD), the National Cancer Institute (NCI), the National Institute on Drug Abuse (NIDA), and the National Institute on Mental Health (NIMH). This research was funded, in part, by a microgrant award from the District of Columbia Center for AIDS Research, an NIH-funded program (AI117970), which is supported by the following NIH Co-Funding and Participating Institutes and Centers: NIAID, NCI, NICHD, NHLBI, NIDA, NIMH, NIA, FIC, NIGMS, NIDDK, and OAR. This study was funded by GWU start-up funds (M.G.) and a DC-CFAR microgrant (M.G.).
Preliminary data were reported at the HIV Research for Prevention Conference, Cape Town, South Africa, November 2014 (Poster).
Disclaimer
The contents of this publication are solely the responsibility of the authors and do not represent the official views of the National Institutes of Health (NIH).
Author Disclosure Statement
No competing financial interests exist.