
Abstract
Infection with human T lymphotropic virus (HTLV), although asymptomatic in most cases, can lead to severe illnesses, such as adult T cell leukemia/lymphoma or myelopathy/tropical spastic paraparesis. HTLV can be transmitted by whole-blood (WB) transfusion. The prevalence of HTLV among blood donor populations has not been characterized in Vietnam, although the screening has been partially implemented on voluntary basis since 2016. To determine the seroprevalence of HTLV-1/2 among blood donors, a total of 14,819 healthy blood donors in northern, central, and southern Vietnam and 1,003 samples from hepatitis B surface antigen (HbsAg), anti-hepatitis C (anti-HCV), or HIV Ag/Ab reactive blood donors were screened for anti-HTLV-1/2 antibodies by a chemiluminescence immunoassay using the Abbott ARCHITECT rHTLV-I/II assay. The anti-HTLV-1/2 repeat reactive (RR) samples were further tested by immunoblot (IB) method using MP Biomedicals HTLV Blot 2.4 for confirmation and differentiation of HTLV-1/2 infection. Proviral HTLV subgenomic amplification of the gag and tax regions was performed on the available WB RR samples (N = 11) by polymerase chain reaction (PCR). Among 14,819 blood donors, 34 samples (0.23%) were RR for anti-HTLV-1/2 antibodies, but only 1 case was confirmed HTLV-2 positive (0.0067%) and 5 cases were classified as indeterminate (0.034%) by IB. The RR rate was 0.39% among HBsAg/anti-HCV/HIV reactive sample groups, but none of them was confirmed by IB. Subgenomic PCR failed to amplify proviral DNA from WB samples of 11 RR samples. HTLV-1/2 prevalence was found to be low among blood donors in the study. Continued vigilance remains essential to maintain a low transfusion-transmitted risk in Vietnam.
Introduction
Human T lymphotropic virus type-1 and -2 (HTLV-1/2) were discovered in the early 1980s 1 as pathogens leading to severe infection in humans. Soon after their discovery, it was realized that blood transfusion was associated with high rates of transmission due to the infusion of infected lymphocytes. Most of the infected people live without any symptoms; however, in a portion of carriers, HTLV-1 causes adult T cell leukemia (ATL), HTLV-1-associated myelopathy (HAM)/tropical spastic paraparesis, and HTLV-1 uveitis/HTLV-1-associated uveitis after a long period of latency. 2 Since HTLV infection is often asymptomatic, clinically recognized reports of patients infected via blood transfusion are rare. However, there are case reports of transfusion-transmitted HTLV-1 infection associated with the accelerated onset of HAM, a debilitating spinal cord condition, while the development of post-transfusion ATL is very rare. 3 –5 Since the virus has a long asymptomatic phase and high rates of seroconversion after transfusion, the risk of transmission from asymptomatic blood donors should be considered and appropriately managed, particularly in high-prevalence areas. As per the World Health Organization recommendations, the decision to screen donations for HTLV-1 infection should be made based on local epidemiological evidence. 6
HTLV-1 is widely disseminated and at least 5–10 million people worldwide are estimated to be infected. 7 Most HTLV-1 infections are found in highly endemic regions, including southwestern Japan, sub-Saharan Africa, South America, the Caribbean, and foci in the Middle East and Australo-Melanesia. In many endemic regions, HTLV-1 coinfections with other transfusion-transmitted infection (TTI) pathogens have also been reported among the high-risk populations. 8 –11 The Southeast Asian region comprises more than half a billion individuals; yet, HTLV-1 prevalence in the most populated countries has been poorly described.
In Vietnam, the epidemiology of HTLV-1 is poorly characterized, although the presence of HTLV-2 has been reported in the past. A seroepidemiologic survey conducted in 1994 found an HTLV-2 seroprevalence of ∼1% (4/500) among blood donors in South Vietnam. 12 All four HTLV-2-positive sera were from male professional blood donors living in Ho Chi Minh City and its neighboring province in South Vietnam, who were retrospectively identified as injection drug users (IDUs). In a cohort of South Vietnamese IDUs, 10 the seroprevalence of HTLV-2 was observed to be 59.5% (119/200) seropositive, while lower prevalence rates were observed in hemodialysis patients (2/30; 6.7%), children (2/200; 1%), and the general population (1/200; 0.5%) in 1995. None of these seroepidemiologic surveys 10,12 reported any HTLV prevalence from North Vietnam or the prevalence of HTLV-1. Nonetheless, transfusion transmission of HTLV remains a risk in Vietnam with 6 HTLV-2 infections identified among 61 Vietnamese thalassemic patients (9.1%) who received multiple transfusions from paid donors in South Vietnam. 13 However, due to the lack of recent large and representative studies, the current prevalence of HTLV-1 and -2 in Vietnam remains unknown. We therefore investigated the seroprevalence of HTLV-1/2 in large Vietnamese blood donor populations.
Materials and Methods
Ethics statement
The study was conducted in accordance with the guidelines of the 1975 Declaration of Helsinki and the principles of good clinical practice. All procedures were approved by the Medical Ethics Committee of National Institute of Hematology and Blood Transfusion (NIHBT), Hanoi, Vietnam. Written informed consent was obtained from all subjects.
Study site and participants
This cross-sectional study was carried out at NIHBT in Hanoi, Vietnam, from January 2016 to August 2017.
A total of 14,819 blood samples from healthy blood donors were randomly selected to be included in this study (Fig. 1). Sample collection was conducted in two stages. Stage 1 was carried out in July 2016 with 8,169 samples collected, which included 2,299 blood samples from the Northern Vietnam provinces (Lang Son, Thai Nguyen, Son La, Hoa Binh, Hanoi), 2,699 blood samples from the Central Vietnam provinces (Thanh Hoa, Lam Dong, Khanh Hoa, Dac Lac, Quang Ngai, Quang Nam), and 2,168 blood samples from the Southern Vietnam provinces (Can Tho, Vinh Long, Kien Giang). Stage 2 was carried out in October 2016 with 7,653 samples from the Northern provinces (Son La and Hanoi). Blood donors were selected by the blood center if they fulfilled all the criteria to be eligible for donation as described by the standard operating procedure of NIHBT. All blood samples from the blood donors enrolled in this study were tested for hepatitis B surface antigen (HBsAg), anti-hepatitis C (anti-HCV), anti-human immunodeficiency virus types 1 and 2 antibodies and antigen (HIV combo Ag/Ab), and syphilis before HTLV-1/2 screening.
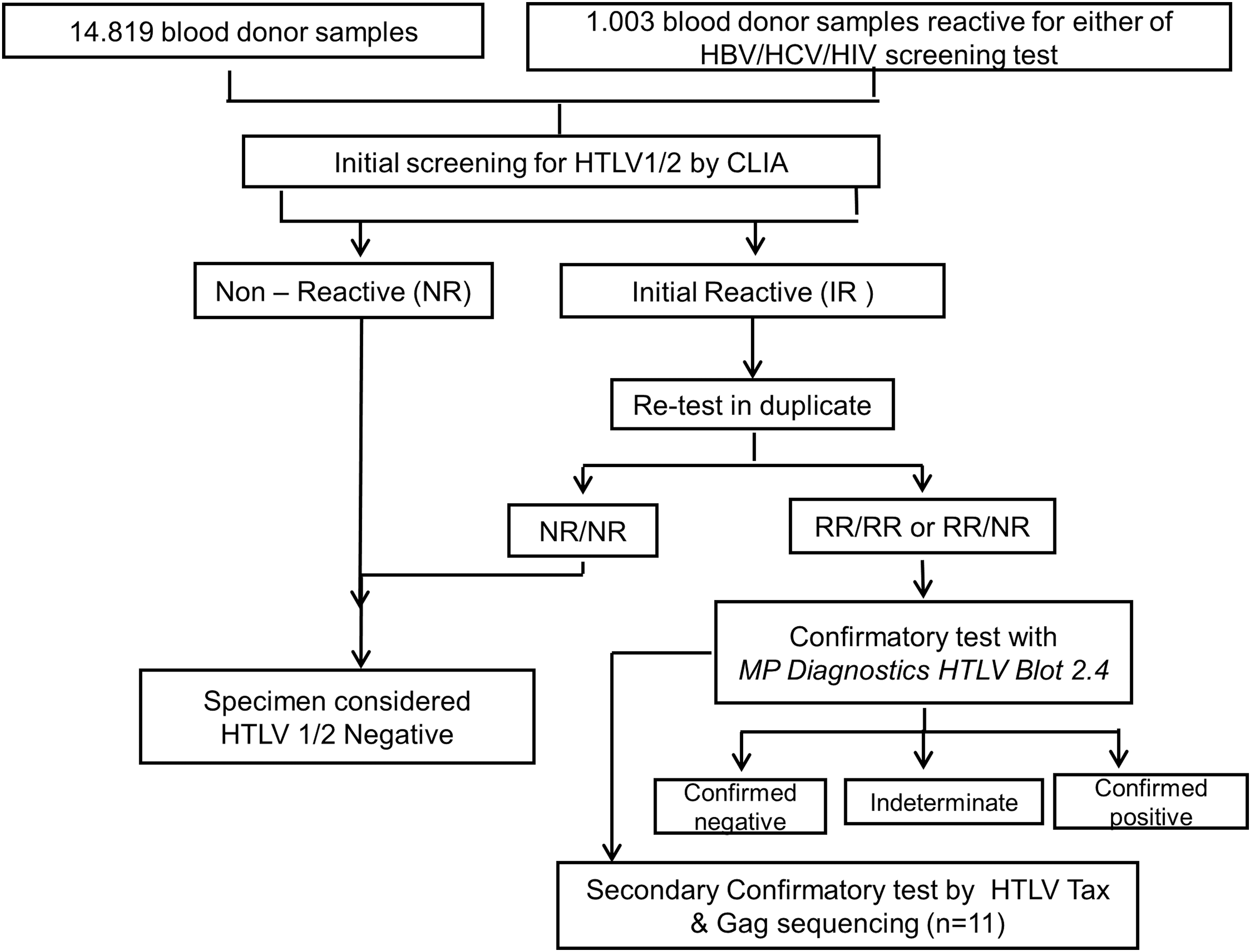
Flow chart of screening and confirmation of HTLV infection.
Besides that, we also included stored samples from previously screened donors from Northern, Central, and Southern Vietnam (839, 134, and 30, respectively), which were found reactive for at least one other TTI (HBsAg, anti-HCV, or HIV combo Ag/Ab). A total of 1,003 screened reactive samples (492, 413, and 95 samples reactive with HBsAg, anti-HCV, and HIV combo Ag/Ab, respectively), which were collected from January 2016 to June 2016 were included in the study. The plasma samples were stored at −25°C until HTLV testing.
The data extraction form was used to collect information regarding sociodemographics and a history of blood donation of each participant. Recorded sociodemographic information included sex, age in years, place of birth, and the participant's (blood donor) residence location. Study participants were anonymized and identified by a study number.
Inclusion and exclusion criteria for blood donors
All donated blood, which screened nonreactive for HBsAg/anti-HCV/HIV combo Ag/Ab and syphilis, was included in the study, except the reactive 1,003 stored samples. Any lipemic and hemolytic blood samples were excluded from the study.
Serological testing
An anti-HTLV-I/II chemiluminescent immunoassay (CLIA) was used for initial screening of the infection. The assay was performed on an Architect i2000SR immunoassay analyzer (Abbott Laboratories, Abbott Park, IL) as per the manufacturer's instructions. All initial reactive (IR) samples in the initial screening were repeated in duplicate (repeat reactive [RR]) using the same assay, followed by a confirmation testing using immunoblot (IB) (HTLV blot 2.4; MP Biomedicals, Singapore), which can also differentiate between HTLV-1 and HTLV-2 infection. An HTLV infection episode was defined as positive in both CLIA and IB testing (Fig. 1).
Molecular characterization of HTLV-1 and -2
Proviral DNA extractions from whole-blood (WB) specimens and amplification of the gag and tax regions by polymerase chain reaction (PCR) were performed as previously described, 14 using primer sets designed and validated for identifying HTLV strains. 15
Statistical analysis
The data were analyzed with software Microsoft (MS) Excel version 16.0 (2016) and SPSS version 22.0.
Results
A total of 14,819 healthy blood donors from Northern (9,952 samples), Central (2,699 samples), and Southern Vietnam (2,168 samples) were included in the study population (Fig. 1). The average age in this group was 29 years, with 91.53% of these donors younger than 50 years (Table 1; Fig. 2). There were more male blood donors (58.3%) than female blood donors (41.7%) and most were first-time donors (FTD; 59.1%). The average age was 32 years in the HIV/HBV/HCV reactive cohort (Table 1). There was a much higher percentage of FTDs (81.0%) in this group as well and a similarly higher proportion of male blood donors (72.9%) than female donors (27.1%).

Age distribution of healthy blood donors included in the study. Age distribution in years (18–30), (31–40), (41–50), and (51–60), in brackets. FTD, first-time donor; RTD, repeat donor. Color images are available online.
Demographic Characteristics of the Blood Donors
FTD, first-time donor; RTD, repeat donor; HbsAg, hepatitis B surface antigen; anti-HCV, anti-hepatitis C.
Of the combined 15,822 samples, serological screening identified 44 samples with IR results for HTLV antibodies and 38 of these were RR (Table 2). The highest RR signal to cutoff (S/CO) value was 14.17 and the mean of negative samples S/CO was 0.101 ± 0.056. Among the healthy donor cohorts, there were 34 RR (0.23%), but only 1 sample (0.0067%) was confirmed by IB and 5 samples (0.034%) were reported indeterminate (Table 3). The confirmed sample showed anti-gag reactivity with a p24 signal stronger than that of p19, favoring an HTLV-2 infection. Two of five indeterminates gave only one unique band (GD21/rgp46-II) on IB, while the remaining three had multiple band patterns different from HGIP (GD21&p19/GD21&rgp46-II/GD21&rgp46-I& rgp46-II). Of the 1,003 HIV/HBV/HCV reactive samples, 4 specimens were RR, but none of them was confirmed by IB (Table 3). The overall prevalence of HTLV infection was 6.3 per 100,000 donations.
HTLV 1/2 Screening and Confirmatory Results, Signal to Cutoff
RR, repeat reactive; IR, initial reactive; S/CO, signal to cutoff; HTLV-1/2, human T lymphotropic virus type-1 and -2.
HTLV 1/2 Screening and Confirmatory Results
The RR specimen that was confirmed by IB was in the highest S/CO bracket among RR specimens, which mostly had S/CO values below 10 (Table 2). This specimen was from a 31-year-old donor living in Khanh Hoa of Central Vietnam. Five samples with indeterminate results included two male and three female donors who were 20–24 years old and resided in Northern Vietnam (Table 4). No further donor follow-up was possible. Further molecular characterization of N = 11 available RR WB samples was performed by proviral HTLV gag and tax region PCR, which failed to produce amplicons for sequencing from any of the 11 specimens. The set of 11 WB specimens for molecular characterization included 4–5 indeterminate specimens but did not include the IB-confirmed infection, which did not have a paired WB specimen available.
Demographic Characteristics of Six Blood Donors Tested Positive/Indeterminate on Immunoblot
VN, Vietnam.
Discussion
This study was carried out using 15,822 blood donor samples to provide seroprevalence data for HTLV-1/2 infections in the Vietnamese blood donor population. Under current National blood transfusion program me guidelines–No 26/2,013, blood donors must be between 18 and 60 years old, healthy, negative for anemia and HBV/HCV/HIV/syphilis. Blood donors are also assessed for their self-reported health status for any acute or chronic disease and risk behaviors for TTI. Because of their large numbers, uniform sampling frame, and availability of testing data with screening immunoassays, blood donors may serve as a convenient sentinel population when attempting to estimate the prevalence of viral infections. One caveat is that the population prevalence will be underestimated because of self-selection by donors and exclusion by blood banks of unhealthy or potentially at-risk candidates. Therefore, the results from this blood donor study cohort might not be representative of HTLV prevalence among the general population of Vietnam.
Of 15,822 blood donor samples, only one sample from south-central Vietnam was confirmed positive for HTLV-2 (the Northern 0/9,952 and the Central—Southern 1/5,870). This is consistent with a previous report in 1994 by Yamamoto et al. which only found HTLV-2 infections in Southern Vietnam (4/500) and none in Northern Vietnam (0/500) among blood donors. 12 Likewise, our sero classification of the confirmed infection as HTLV-2 is consistent with the documented presence of HTLV-2 strains in Vietnam. 10,12–13,16 Future sequencing and classification of HTLV infections may provide epidemiological insight toward the epidemiology of HTLV-2 in Vietnam.
Notably, none of the samples reactive for HBsAg, anti-HCV, or HIV Ag/Ab was found to be HTLV-1/2 positive/indeterminate. This in contrast to a previous study that found a higher prevalence of HTLV among HIV-positive (62.5%), HBV-positive (12.5%), and HCV-positive (100%) cohorts. 16 However, the HIV, HBV, and HCV cohorts in the previous study were all IDUs, who carry a higher risk for HTLV infection. 16
Five IB indeterminate samples, including four samples from blood donors in Hanoi and one from Son La, were identified in the study (Table 3). Although the significance of the reasons for indeterminate blotting patterns remains unclear, several possible explanations have been proposed for the occurrence of HTLV-1/2 seroindeterminates: cross-reactivities to other known retroviruses or a novel virus, antibody responses to a malaria parasite with epitope homology to HTLV-1, a defective HTLV-1/2 antibody response, or low viral load eliciting a weak antibody response. 17 Unfortunately, the negative PCR results for four of the seroindeterminate specimens could not rule out any of these possibilities. Although the seroindeterminate specimens were classified as HTLV antibody negative, they suggest a higher rate of HTLV exposure may exist in the study population.
Although any S/CO ratio of 1 or above is considered reactive in the CLIA HTLV screening test, it has been observed that samples with an S/CO between 1 and 5 have a low likelihood of positive confirmatory testing. 18 Our data also follow this trend with samples having an S/CO value in the [1–5] interval giving the highest false-positive rate among IR specimens. In regions of low HTLV endemicity, high assay specificity is important. Herein, we observed 99.77% CLIA HTLV testing specificity among the healthy donor groups, which is comparable with previous high-specificity reports. 19,20
The HTLV prevalence was found to be low among healthy blood donor populations in Vietnam in this study. However, the finding of HTLV-2-positive sample in Southern Vietnam is in alignment to the past reports of HTLV-2 prevalence among different study groups and highlights the possibility of relatively small foci or clusters with a high prevalence of infection, with nearby quite low endemic areas. This nonhomogenous HTLV distribution has been very well exemplified in southern Japan and in some areas of South America and Australia. Thus, further investigation is warranted to explore the extent of HTLV prevalence in the key population groups and regions to control high-risk transmission for a safe blood transfusion.
The higher prevalence of HTLV in other parts of the world, combined with increased global travel, immigration, and military deployments, continues to put the safety of the blood supply in Vietnam and other low endemicity countries at risk for HTLV TTI. The low seroprevalence of HTLV in a large blood donor cohort presented here is an indicator of the success of previous screening and diagnosis of HTLV infections during the interim period between high-prevalence reports published in the 1990s and today. Continued screening for HTLV will be critical to safeguard the blood supply of Vietnam from future HTLV outbreaks.
Footnotes
Acknowledgments
This research was supported by a grant from Abbott Laboratories. We acknowledge the Abbott Global Viral Surveillance team, Chicago, for the valuable support in conducting molecular confirmatory testing of HTLV-1/2 reactive donor samples.
Author Disclosure Statement
No competing financial interests exist.