
Abstract
Lymphocyte subsets of long-term non-progressor (LPNT) HIV-infected children is a less studied aspect of HIV infection. Evaluation of different lymphocyte subsets was done in HIV-infected children ≥8 years of age. Subjects were divided in two groups—group 1 (LTNP), treatment-naive with CD4 ≥ 500 cells/μL (n = 20); group 2, non-long-term non-progressor (nLTNPs) receiving antiretroviral therapy (ART) with CD4 count ≤500 on at least one occasion (n = 21). Group 3 comprised age-, sex-matched healthy controls (HCs, n = 20). Lymphocyte subsets were acquired with a flow cytometer (Navios; Beckman Coulter), and data were analyzed using Kaluza flow analysis software. The mean ages were 12.1 (±2.4 SD) and 12.5 (±2.7) years with mean duration of follow-up of 6.8 (±3.4) and 5.6 (±1.95) years in LTNP and nLTNP subjects, respectively. The mean duration of ART was 5.17 years for group 2. Absolute count and percentage of CD4+ T cells was lower in nLTNPs than in LTNPs. Cytotoxic T cells were high in both HIV-infected groups compared with HCs. Natural killer (NK) cells were found to be significantly lower in LTNP and nLTNP groups compared with HCs (p ≤ .000003 and p ≤ .00003, respectively). Naïve B cells were more in HIV-infected individuals than in HCs. NK cells were significantly lower in LTNP and nLTNP groups. Immune reconstitution was comparable in children initiated with ART early versus long-term HIV-infected children receiving no ART.
Introduction
In the absence of antiretroviral drugs, 20%–30% of HIV-1-infected children experience rapid progression to AIDS or death in first year of life, while 60%–80% of infected children manifest with less severe symptoms and survive through adolescence. 1,2 A small proportion (<5%) of these infants have very slow progression of disease, maintain stable CD4 counts, do not need antiretroviral therapy (ART) for a long time, and are termed as long-term non-progressors (LTNPs). 3 A subcategory (<1%) among these LTNP population are individuals who maintain a HIV viral load at <50 copies/mL without antiretrovirals for a long period of time and are called as elite controllers (ECs). 4
Cellular immunity [T and B cells, natural killer (NK) cells, monocytes] plays a significant role in HIV control, and there is a state of persistent immune activation during the course of HIV infection. 5 Strong polyfunctional cytotoxic T lymphocyte responses and maintenance of greater proliferative capacity of HIV-specific CD8+ T cells in long-term survivors compared with early progressors are well documented. There are limited data on mechanisms elucidating how LTNP and ECs maintain the HIV control. Defining what enables LTNPs to control viral replication would aid in the development of effective vaccine and treatment regimens. Moreover, alteration in NK cell activation, differentiation, and perforin expression have been found to be associated with perinatally acquired HIV infection, which may also influence the lymphocyte subpopulations.
To the best of our knowledge, characteristics of lymphocyte subsets in perinatally acquired HIV-infected children who are LTNPs and their comparison with age- and sex-matched healthy controls (HCs) have not been systematically performed in Indian settings before. With the provision of revised ART guidelines in the national program of treating all individuals irrespective of their CD4 count, this precious cohort of slow progressors or LTNPs will not be available anymore. This study was planned to analyze T cell, B cell, and NK cell subsets in perinatally acquired LTNP HIV-infected children and compare the proportion of these cells with perinatally infected nLTNP HIV-infected children as well as normal controls in a tertiary care hospital and research institute in India.
Materials and Methods
This cross-sectional observational study was conducted in the Department of Pediatrics, Advanced Pediatrics Centre, Postgraduate Institute of Medical Education and Research (PGIMER, Chandigarh, India). Study subjects were enrolled from the Pediatric Immunodeficiency Clinic, and blood samples were analyzed in the Pediatrics Allergy and Immunology Laboratory, Advanced Pediatrics Centre, and Department of Immunopathology, PGIMER. Ethical clearance for this study was obtained from the Institute's Ethics Committee as well as from the Departmental Review Board.
Patient screening, assessment for eligibility, and enrollment
A total of 840 HIV-infected children were registered at the Pediatric Immunodeficiency Clinic of HIV till December 2015. Of these, 111 (3.8%) were newly identified HIV-infected children who got registered in the clinic (49th Annual Report, PGIMER 2015–2016). These were screened for enrollment to the study as per the inclusion criteria of age ≥8 years with a history of perinatal acquisition of HIV, being treatment-naïve, and with stable CD4 cell count ≥500 cells/μL. These children were then classified as LTNPs (n = 20, group 1). Children with perinatal acquisition of HIV infection with CD4 cell count ≤500 on at least one occasion, receiving antiretrovirals, were classified as non-LTNPs (nLTNPs; n = 21, group 2). Patients with transfusion-acquired HIV, or with unclear mode of transmission, or noted to have fever/diarrhea/active upper respiratory tract infection/rash, or any inter-current illness or history and clinical examination for evidence of tuberculosis based on positive tuberculin skin test and abnormal chest x-ray were excluded from the study. HCs (n = 20, group 3) from routine outpatient department formed the normal control group. Children were enrolled after taking informed consent from parents/primary caregivers. An assent was sought from children in whom the disease was disclosed. Relevant history was recorded in the predesigned proforma from their parents and available case sheet. Demographic information included child's age, age at diagnosis, mode of transmission, previous CD4 counts, socioeconomic background, and clinical manifestations. Blood samples were timed with routine CD4 count sample to avoid extra prick to children. Based on the CD4+ T cell counts (absolute number and percentages), LTNPs and nLTNPs were classified according to the World Health Organization (WHO) immunological classification for established HIV infection. 6
Sample collection
Three milliliters of venous blood was collected from all enrolled children during their visit in the follow-up clinic using aseptic procedure in an ethylenediaminetetraacetic acid vial on a single occasion. This collection was timed to their routine CD4 count evaluation. Blood thus obtained was processed on the day of collection of sample for flow cytometric analysis.
Flow cytometry protocol for the study
Evaluation of different lymphocyte subsets (T cells, B cells, and NK cells), T lymphocyte subsets (helper T cells and cytotoxic T cells), CD45 RA/RO (naïve and memory T cells), and memory B cells (CD19+CD27+)/naïve B cells (CD19+CD27−) was done. All the antibodies were procured from BD Biosciences. Lyse (lysis solution; HIMEDIA cat no. R075), no-wash protocol was performed for lymphocyte subset with multi-test CD45 (PerCP)/CD3 (FITC)/CD19 (APC)/CD56/CD16 (FITC) (cat no. 340500) kit. T cells subset was analyzed with a four-color multi-test CD3 (FITC)/CD4 (APC)/CD8 (PE)/CD45 (PerCP) (cat no. 340499) kit. Memory/naïve T cells analysis was done with multi-test CD3 (PerCP)/CD8 (APC)/CD45RA (FITC)/CD45RO (PE) (cat no. 340574) kit. Evaluation of memory B cells was performed using CD19 (APC) (cat no. 555415) and CD27 (PerCP-Cy™ 5.5) (cat no. 560612) by lyse and wash surface staining protocol. Samples were acquired on a flow cytometer (Navios; Beckman Coulter), and data were analyzed using Kaluza flow analysis software (Beckman Coulter). Lymphocytes were gated for subset analysis on side scatter versus CD45 plot as side scatter low and CD45 bright population.
Statistical analysis
Both percentage and absolute counts of different lymphocyte subsets were taken into consideration for comparison of immunological profiles among the three study groups. Each of the parameters was separately analyzed for normal distribution with the Shapiro Wilk test among the three study groups. As the data were not normally distributed, these are represented as median with interquartile ranges (IQRs) and percentages. The distribution of the above variables was compared among the three groups with the Mann–Whitney U test and Kruskal–Wallis test.
Results
A total of 61 children (n = 21 LTNPs, 21 nLTNPs, and 20 HCs) were enrolled to the study. The mean ages of subjects enrolled were 12.1 (±2.4 SD), 12.5 (±2.7), and 12.7 (±2.6) years for the LTNP, nLTNP, and HC groups, respectively. The older child in the LTNP group of study was 17.1 years. WHO clinical staging was done for all subjects. Sixty-five percent of LTNPs were classified in stage 1 and 35% in stage 2. Among the nLTNPs, 42.9% were in stage 2, 47.6% in stage 3, and the rest (9.5%) in stage 4 of HIV infection. Out of 20 LTNPs, 12 children had no significant HIV-associated immunodeficiency, and 8 children had mild HIV-associated immunodeficiency. Out of 21 nLTNPs, 12 children had advanced HIV-associated immunodeficiency, and remaining had severe immunodeficiency. The median hemoglobin concentration of LTNP, nLTNP, and HC groups was 11.15, 11.5, and 11.95 g/dL, respectively. The median platelet count of the LTNP and nLTNP groups was 250,000 and 275,000, respectively, whereas that of the HC group was 263,000. The total leucocyte counts of LTNP, nLTNP, and HC groups was 7,700, 6,000, and 7,800 cells/μL, respectively. The lymphocyte percentages were 55.5%, 47%, and 44.5%, respectively, among LTNP, nLTNP, and HC groups. The mean duration of follow-up for LTNPs and nLTNPs was 6.8 (±3.4 SD) and 5.6 (±1.9) years, respectively. The median duration of ART in nLTNPs was 5.17 years with Q1, Q2, and IQR of 4.48, 6.9, and 2.42 years, respectively. Out of 21 patients in nLTNP group, 17 received Zidovudine (AZT)/Lamivudine (3TC)/Nevirapine (NVP) (FDC) combination ART, 1 received Efavirenz (EFV)-based ART (AZT/3TC/EFV), and 3 were on Abacavir/Lamivudine/Lopinavir/Ritonavir (ABC/3TC/LPV/r). Figure 1 shows the distribution of T and B lymphocyte subsets, NK, and natural killer T (NKT) cells in a bar diagram. Comparisons of immunological profiles among different study groups are shown in Tables 1 –3, respectively. No significant variation was found among the different lymphocyte subsets between LTNPs and nLTNPs who were on ART for a mean duration of 5.17 years. Absolute count and percentage of CD4+ T cells was lower in nLTNPs than LTNPs. Cytotoxic T cells (both naïve and memory) were high in HIV-infected individuals (LTNPs and nLTNPs) compared with HCs. The percentages and counts of total T cells, memory T cells, and cytotoxic T cells were high in LTNPs compared with controls. Similar to LTNPs, nLTNPs also had higher counts of these cells than controls but not as high as LTNPs. Memory B cells were significantly higher in healthy population compared with HIV-infected individuals. Percentage NK cells and absolute NK cell count was found to be significantly lower in LTNP and nLTNP groups compared with HCs (p ≤ .000003 and p ≤ .00003, respectively). No significant variation was seen in NKT cells among all the three groups. Naïve B cells were more in HIV-infected individuals than the HCs.
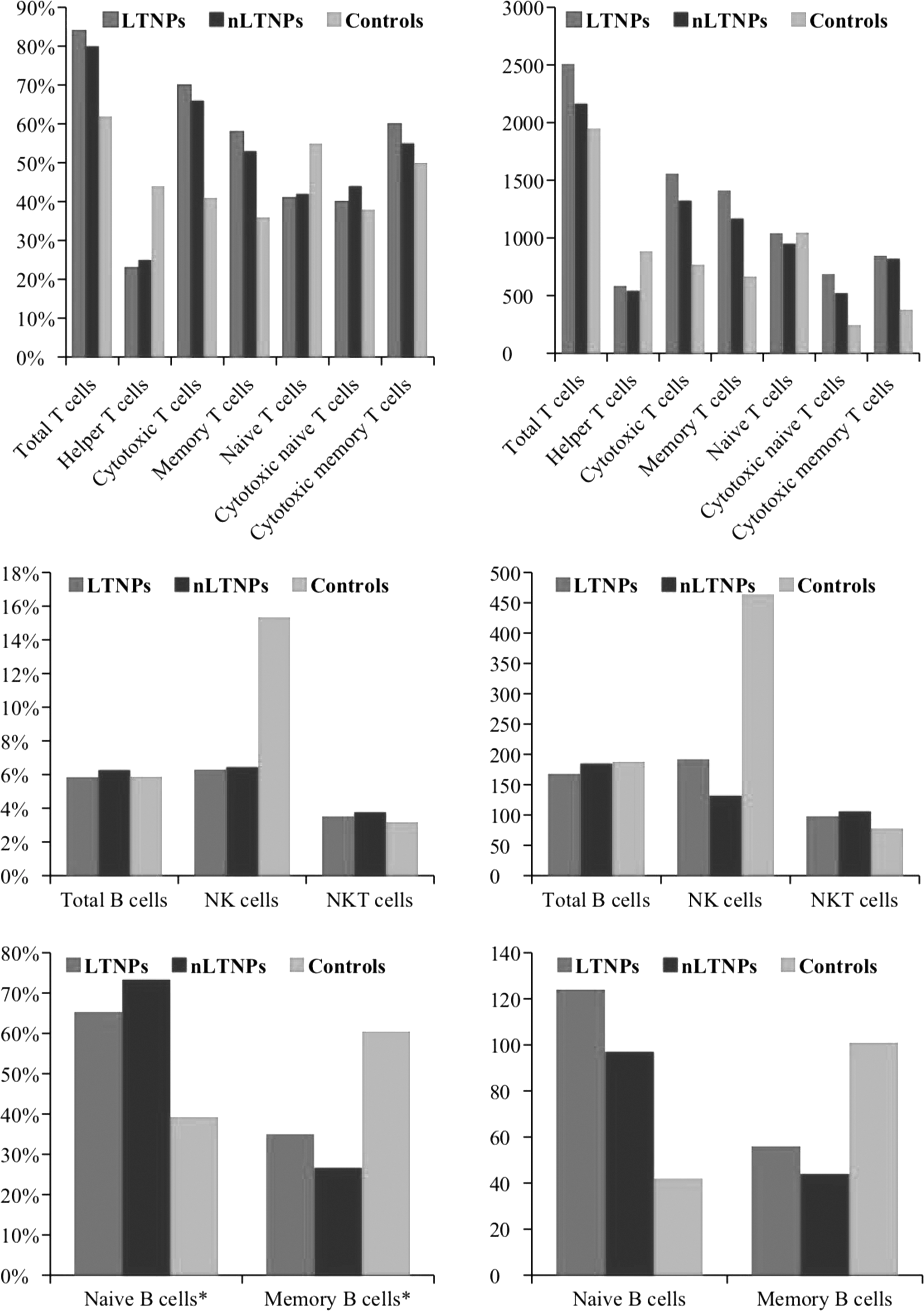
Comparison of different subsets of T, B, NK, and NKT cells among three groups (LTNPs, n = 20; nLTNPs, n = 21; controls, n = 20). For comparisons, median values are taken into account. NK, natural killer; NKT, natural killer T cells; LTNP, long-term non-progressor; nLTNP, non-long-term non-progressor.
Distribution of T Lymphocyte Subsets Among Different Study Groups
All values are expressed as median (IQR); p-value computed using Mann–Whitney U test.
LTNP, long-term non-progressor; nLTNP, non-long-term non-progressor; IQR, interquartile range.
Distribution of B Lymphocyte Subsets Among Different Study Groups
All values are expressed as median (IQR); p-value computed using Mann–Whitney U test.
Distribution of Natural Killer and Natural Killer T Cells Among Different Study Groups
All values are expressed as median (IQR); p-value computed using Mann–Whitney U test.
Discussion
LTNPs have been defined variably in the literature. Some studies define them as HIV-infected children who remained asymptomatic for ≥10 years and maintained CD4+ T cell count >500/mm3 without ART. 7 LTNPs within the Chelsea and Westminster HIV cohort had been defined by a duration of HIV infection >7 years from time of diagnosis, in the absence of ART and clinical symptoms, and by the stable maintenance of CD4+ T cell counts (450–1650 cells/mL). 8 Study by Ananworanich et al. has defined LTNPs in Asian cohort as HIV-infected children who remained asymptomatic for ≥8 years with a stable CD4+ T cell count ≥350 cells/mm3 without any ART. 5 Data on proportion of LTNPs and long-term slow progressors (LTSPs) in Indian HIV-1-infected children are scarce. Long-term studies from Mumbai reported 5%–15% adults with HIV to be LTNPs. 9 Slow progression of the disease in HIV-infected adult in the absence of antiretrovirals for >20 years has been reported earlier by our institute. 10 Radhakrishna et al. published a study with 26 pediatric cases who were followed up for 10–15 years. These children remained asymptomatic for 15 years, and in the final categorization, only six could qualify as LTNPs; the rest developed AIDS. 11 Worldwide, there is limited published data on the immunological profile of HIV-infected LTNP children. 12,13 A systematic flow cytometric analysis of these children has not been performed or reported from the Indian subcontinent. This is probably the first attempt to dissect the lymphocyte subsets in this group of children.
We identified 20 HIV-infected LTNPs and 21 nLTNPs in 2015–2016. Serial CD4+ T cells trends of both LTNPs and nLTNPs were captured from the previous records and it was evident that all LTNPs were having stable CD4+ T cell trends over the course of follow-up and were maintaining CD4+ T cell counts >350 cells/mm3. Majority of the children in nLTNP group had a rapid fall in CD4+ T cell counts to <350 cells/mm3, followed by a gradual recovery after starting ART. At the time of enrollment, the mean CD4+ T cell count was 585 and 542 in LTNPs and nLTNPs, respectively, and there was no statistically significant difference between the two groups (p = .008). This suggests that LTNPs could maintain CD4+ T cell counts at par with those who had been initiated on ART, with a mean duration of 5.17 years of ART.
Ananworanich et al. 5 reported lower cell count per mm3 and percent distribution of helper T cells and higher cytotoxic T cells in LTNPs, with a reduction in populations of naïve helper and cytotoxic T cells. HIV-positive children had high values of activated helper and cytotoxic T cells. 5 We also found higher total T cell counts in children living with HIV than in normal controls. Both LTNPs and nLTNPs had lower helper T cells than the HC population (p = .001). Both total cytotoxic and total memory T cells were significantly higher in LTNPs and nLTNPs than in HCs (p ≤ .0001 and p ≤ .001, respectively). The cytotoxic T lymphocytes (total, naïve, and memory) were significantly higher in LTNPs compared with nLTNPs (p ≤ .0001, p ≤ .00005 and p ≤ .01, respectively). There was no statistically significant difference between the naïve T cells among LTNPs, nLTNPs, and HCs (p = .705, .389, and .389, respectively). The study of activation markers for helper or cytotoxic T cells was not the part of this study.
Slower disease progression of HIV disease has been associated with more efficient and robust functional profile of CD8+ T cells. 14 We did not study the function or activation of these CD8+ T cells; however, the number of CD8+ T cells was much higher in LTNPs than the controls (p ≤ .0001).
We also studied B cell population in our cohort. There was no significant variation in total B cells among the three groups; however, absolute count and percentage of memory B cells was higher in controls. Absolute count and percentage of naïve B cells was found to be higher in HIV-infected children compared with controls although it did not reach statistical significant level. De Milito et al. found untreated HIV-infected patients to have lesser memory B cells compared with controls. 15
The innate immune system, including NK cells, plays an important role in the lysis of HIV-infected cell and is a major defense to eliminate virus much before the establishment of adaptive immune response in various acute viral infections. A role of NK cells in the immune response to HIV infection was highlighted when a correlation between slow progression to AIDS and killer immunoglobulin-like receptors in conjunction with certain HLA alleles was found. 16 HIV-1 infection can lead to the downregulation of HLA A and B proteins on the surface of infected cells, which triggers NK cell activation, whereas HLA-C molecules are not downregulated by HIV, thus aiding in provision of protection by NK cells. 17 Cytotoxicity, as measured by the killing of prototypic NK cell target cell line, and lower antibody-dependent cellular cytotoxicity have been found in various studies. 18,19 However, there is limited literature on NK cell function in HIV-infected children. Vertical HIV infection is also associated with increased NK cell activation, differentiation, and loss of perforin expression, which might impair NK cell function and compromise their role in protecting the organism against HIV, co-infections, and cancer. 20 However, higher number of NK cells has been reported as HIV controller than the chronic progressors. 5,21 Douek et al. has suggested reduced NK cells in HIV-infected children compared with the control population. 22 We also found significantly lower percentage and total NK cells in HIV-infected children in comparison with HCs; however, the LTNPs without antiretroviral exposure were demonstrated to have NK cells at par with nLTNPs receiving ART.
Studies have shown that viremic individuals presented with a reversible decrease in the cytotoxic subset of NK cells and an increase in dysfunctional NK cell subset. Whereas slow progressors were found to have normal or maintained NK cell phenotype. 23,24 Proportions of dysfunctional NK cells change with chronic inflammation, infection, and HIV control. This dysfunctional subset of NK cells was not evaluated in our study. We speculate that the contribution of these cells may have influenced the results. There could be a variation in cell count versus percentages. This being a cross-sectional measurement could give a varied picture over time or in presence of any opportunistic or co-infection.
Several studies have been conducted to know the effect of ART on the immunological profile of HIV-infected children. It has been found that early and prolonged ART in rapid progressors is associated with an HIV-1-specific T cell profile comparable to that of LTNPs. Benito et al. found that ART decreases immune activation in all T cells. 25 Children on ART also had higher memory cytotoxic CD8+ T cells and activated cytotoxic CD8+ T cells than normal HCs, whereas naïve cytotoxic T cells were high in controls in comparison to children on ART. 26 Unlike LTNPs, early progressors even on ART are unable to sustain CD8 responses despite restoration of CD4 proliferation. 27 HIV-infected immunologic responders on prolonged ART have been found to have controlled NK cell activation compared with non-responders, which might play a significant role in blunted CD4 T cell recovery in individuals on ART. 28
From the above discussion, it can be concluded that the immune profile of rapid progressors could improve dramatically after ART and reach a level comparable to that of LTNPs.
The availability of viral load data would have added strength to our study findings. Studies have also shown an association of genetic polymorphism in HLA proteins with slow progession of the disease. Genome-wide genetic association studies would further help to provide insight into LTNPs or LTSPs.
Footnotes
Acknowledgment
We would like to acknowledge the National AIDS Control Organization for providing free-of-cost ART to HIV-infected individuals.
Author Disclosure Statement
No competing financial interests exist.