
Abstract
We developed a detergent-free enzyme-linked immunosorbent assay (ELISA) for HIV-1 viral protein R (Vpr), an accessory protein of human immunodeficiency virus type-1 (HIV), and detected soluble Vpr in ∼22% of HIV patients who were receiving combination antiretroviral therapy and were free of plasma HIV RNA. Notably, the levels of CD8-positive cell count, soluble intercellular adhesion molecule-1 (sICAM-1), and C-C motif chemokine ligand 2 (CCL2), all of which are markers of chronic inflammation in HIV patients, were higher in Vpr-positive patients than in Vpr-negative patients. Because sICAM1 and CCL2 are associated with an increased risk of HIV-associated neurocognitive disorder, we propose that an established Vpr-ELISA would be useful for monitoring the risk of HIV complications during latent HIV infection.
Since the advent of combination antiretroviral therapy (cART) in the mid-1990s, the mortality rate due to human immunodeficiency virus type-1 (HIV) infection has dramatically declined. Although cART effectively inhibits viral replication and can reduce plasma HIV RNA levels to undetectable levels, various lines of evidence indicate that infected reservoir cells are still present in HIV-infected patients and the virus reappears after suspension of the cART regimen. 1 Moreover, cART neither fully restores immune function nor normalizes chronic inflammation and high levels of cytokines and soluble inflammatory proteins remain, although the T cell immunity is restored. 2 This status of chronic immune activation is associated with an increased risk of a variety of diseases, including cardiovascular diseases, tumors, and HIV-associated neurocognitive disorder (HAND). 3
Viral protein R (Vpr) is an auxiliary regulatory protein of HIV that comprised 96 amino acids and has multiple biological functions in infected cells, including cell cycle arrest at the G2/M checkpoint, the induction of apoptosis, the transcriptional activation of HIV long terminal repeat, and the regulation of splicing. 4 Moreover, Vpr is released into peripheral blood and extracellular soluble Vpr has also multiple trans-acting functions, including DNA-damage responses, deregulated lipid metabolism, and retrotransposition of long interspersed element-1. 4 It is plausible that the circulating Vpr is involved in multiple HIV-related complications. To detect soluble Vpr in the blood of HIV-positive patients, we previously performed immunoprecipitation followed by western blot (IP-WB) analysis, and demonstrated that Vpr is present in the peripheral blood, even in those receiving cART. 5 However, due to the lack of a quantitative method, it was difficult to evaluate soluble Vpr in relation to pathogenic indices.
Vpr is encapsulated within viral particles and released when treated with detergents, and thus it is crucial to measure soluble Vpr in peripheral blood under detergent-free conditions. To obtain monoclonal antibodies that react to a native form of Vpr, we first generated a phage-display library that was prepared from mRNA of immunized chicken spleens, and then isolated three different groups of 22 recombinant monoclonal antibodies that reacted with recombinant Vpr protein (rVpr) (Fig. 1A; Supplementary Methods section). We subsequently selected B34 antibody as the best clone as it could detect a wider range of rVpr (Supplementary Fig. S1A, B). Its equilibrium dissociation constant was KD = 2.4 × 10−8 M (Fig. 1B). Combined with a purified anti-Vpr rabbit polyclonal antibody as a capture antibody, blood-circulating Vpr was successfully measured with a limit of quantification of 39 pg/mL [Vpr-enzyme-linked immunosorbent assay (ELISA); Supplementary Fig. S1C and Supplementary Methods section].
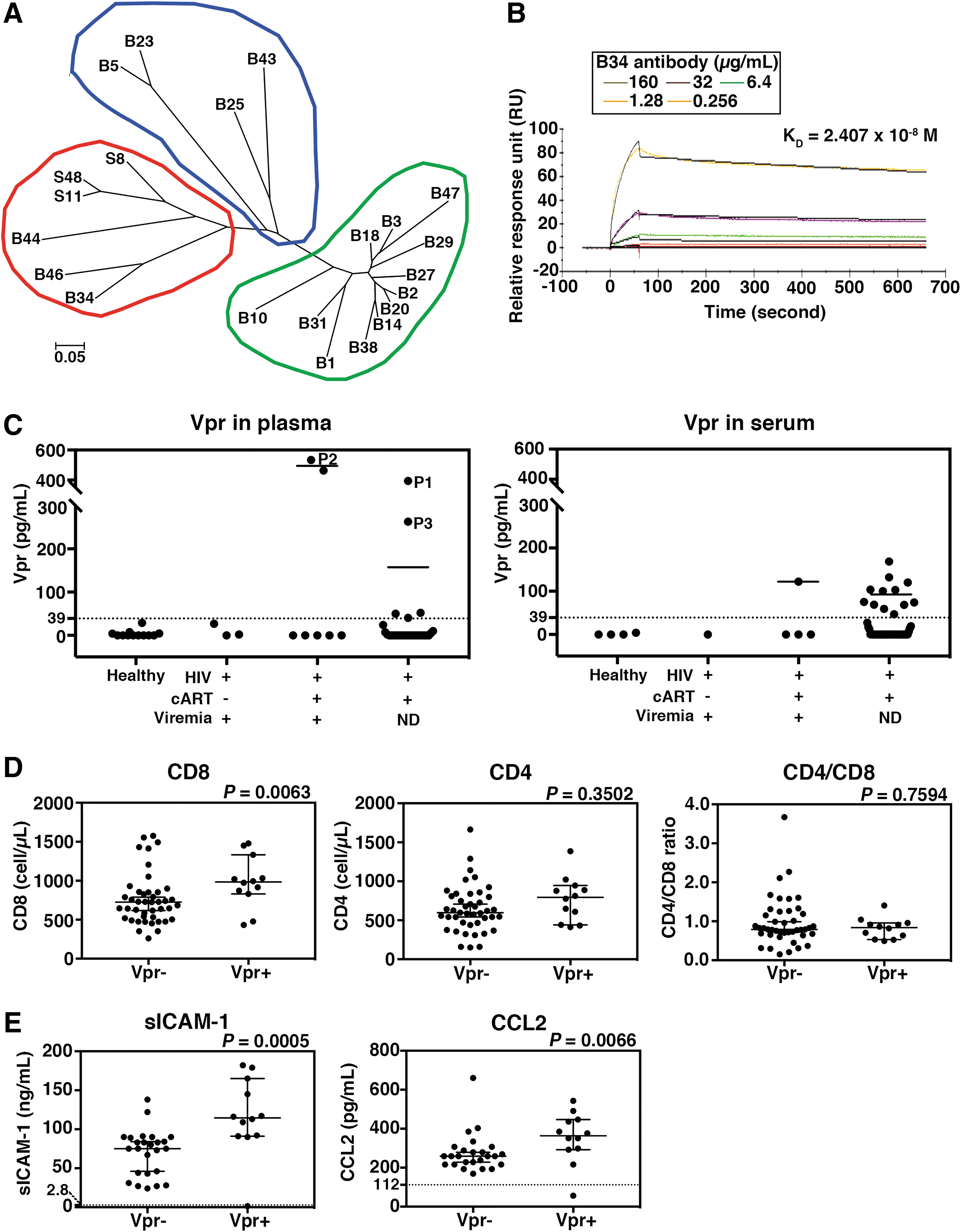
Establishment of a detergent-free Vpr-ELISA system and detection of soluble Vpr in plasma/serum of HIV patients.
To evaluate the efficacy of the established Vpr-ELISA, we examined 40 plasma and 60 serum samples from HIV-positive patients randomly selected from the National Center for Global Health and Medicine (NCGM) Biobank, and their clinical characteristics are summarized in Supplementary Table S1. Most of the patients were undergoing cART regimens. Of the 40 plasma samples, 10 were viremic and 30 were aviremic (HIV RNA <20 copies/mL). Of the 60 serum samples, 5 were viremic and 55 were aviremic. The distribution of CD4+ T cells, CD8+ T cells, CD4+/CD8+ T cell ratio, and hepatitis B and C virus infections were not significantly different between the viremic (n = 15) and aviremic (n = 85) samples. Healthy human plasma (n = 12) and serum (n = 4) samples were used as controls (Supplementary Table S1).
Vpr-ELISA detected Vpr in 2 of the 10 viremic plasma samples at a median concentration of 499.0 pg/mL, whereas 7 of the 30 aviremic samples had a median concentration of 156.6 pg/mL (Fig. 1C, left). We confirmed the presence of Vpr in the three positive samples by IP-WB analysis using B34 (for capture) and anti-Vpr monoclonal 8D1 antibodies (Supplementary Fig. S1D). 5 In addition, Vpr was detected in 1 of the 5 viremic serum samples at a median of 122.0 pg/mL, and in 12 of the 55 aviremic serum samples at a median of 93.5 pg/mL (Fig. 1C, right). Importantly, the positive frequency of Vpr detection was similar in both plasma (17.5%; 7/40 cases) and serum (21.7%; 13/60 cases), and also in both viremic samples (20.0%; 3/15 cases) and aviremic samples (20.0%; 17/85 cases) (Supplementary Table S2). In total, Vpr positivity was detected in 20% of the samples analyzed, irrespective of viral load.
We next examined the possible link between Vpr and clinical indices. For this, we focused on the aviremic samples to avoid bias due to the inflammation that accompanies viral replication. As shown in Figure 1D, we observed that the CD8+ T cell count was significantly higher in Vpr-positive HIV patients (Fig. 1D, left; p = .0063). In contrast, the CD4+ T cell count and CD4+/CD8+ T cell ratio were not statistically different (Fig. 1D, middle and right; p = .3502 and p = .7594, respectively). CD8+ T cells have been shown to play a central role in the control of HIV replication in the early phase of HIV infection, and increased CD8+ T cell counts during cART regimens indicate chronic inflammation and immune activation. It has been proposed that persistently high CD8+ T cell counts after long-term cART are associated with an increased risk of HIV complications, 6 implying that circulating Vpr is related to non-AIDS-related symptoms.
To identify the possible link between Vpr and inflammatory markers, we quantitatively measured inflammation-related factors in the aviremic samples by multiplex immunoassay (Supplementary Methods section). As shown in Figure 1E, soluble intercellular adhesion molecule-1 (sICAM-1) and C-C motif chemokine ligand 2 (CCL2) levels were different between Vpr-positive and -negative samples (sICAM-1, p = .0005; CCL2, p = .0066). sICAM-1 levels were higher in the Vpr-positive group [median, 114.5; 95% confidence interval (CI), 91–165 ng/mL) than in the Vpr-negative group (75.0; 95% CI: 46–84 ng/mL). Moreover, CCL2 levels were higher in the Vpr-positive group (363.5; 95% CI: 292–447 pg/mL) than in the Vpr-negative group (259.0, 95% CI: 228–279 pg/mL). Our observations were consistent with a previous report showing that chronic inflammation markers persist in HIV patients even after CD4+ T cell levels are restored under cART. 2 Of note, however, Vpr showed no correlation with the other inflammatory factors C-reactive protein (p = .2537; Supplementary Fig. S1E) and soluble tumor necrosis factor receptor 2 (p = .1626; Supplementary Fig. S1F). Interestingly, sICAM-1 is a marker of endothelial injury of the blood–brain barrier, whereas CCL2 is upregulated in encephalitis and HAND. 7 Acheampong et al. reported that Vpr induces apoptosis in human brain microvascular endothelial cells, 8 and Zahoor et al. demonstrated by a microarray study that Vpr upregulates CCL2 in human macrophages. 9 These observations imply that the circulating Vpr is positively linked with the upregulation of sICAM-1 and CCL2 through multiple actions of Vpr. The presence of soluble Vpr may be linked with the risk of future complications but does not seem to affect the daily life of the patients, as no apparent clinical manifestations were observed in the Vpr-positive patients.
Increasing lines of evidence suggest the presence of reservoir cells in HIV-infected individuals. 10 These cells do not actively replicate HIV but can produce viral proteins even under effective cART, 5 implying that Vpr-ELISA could be useful for monitoring the activity of reservoir cells and risk assessments of HIV complications associated with Vpr as well.
Footnotes
Acknowledgments
We thank Kanako Takei at the NCGM, Tokyo, Japan, for providing technical assistance. We also thank the NCGM Biobank for providing the study materials, clinical information, and technical supports. This study was supported in parts by grants from the Research Program on HIV/AIDS (17fk0410208h0002) from the Japan Agency for Medical Research and Development (AMED) and the NCGM grant (29A-1003).
Author Disclosure Statement
No competing financial interests exist.
Supplementary Material
Supplementary Data
Supplementary Figure S1
Supplementary Table S1
Supplementary Table S2
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.