
Abstract
A cross-sectional study was undertaken to examine the prevalence and pattern of HIV drug resistance mutations (DRMs) among recently HIV-1-infected and antiretroviral therapy (ART)-naive individuals from Chennai, South India. The HIV-1 pol gene encompassing the protease and reverse transcriptase (RT) regions were analyzed from 53 ART-naive HIV-1-infected individuals using an in-house method for identifying DRMs by genotyping. The overall prevalence of transmitted drug resistance (TDR) was found to be 11.3% (6/53), which is categorized as moderate level (5.0%–15.0%) of TDR according to the World Health Organization (WHO) survey guidelines. Surveillance drug resistance mutations to non-nucleoside reverse transcriptase inhibitors (NNRTI) were observed in 8.3% (n = 4) of the 48 RT sequences analyzed. No major DRMs related to the protease and nucleoside reverse transcriptase inhibitor (NRTIs) class of drugs were identified.
Introduction
In resource limited countries such as India, the transmission of drug-resistant HIV-1 presents a serious public health concern, as it can potentially reduce the number of antiretroviral (ARV) drugs available to treat infected persons. 1 Periodic surveillance of transmitted drug resistance (TDR) is, therefore, essential to inform public health prevention and treatment strategies. 2 Such surveillance necessitates HIV-1 drug resistance testing at baseline among recently infected or newly diagnosed ARV-naive individuals. There is evidence to show that drug resistance testing before the initiation of antiretroviral therapy (ART) in treatment-naive individuals is cost-effective when the prevalence rates of TDR is something like 8%–10%. 3
According to the latest report of the Joint United Nations Programme on HIV/AIDS (UNAIDS), the prevalence of HIV in India is estimated to be 0.31%, which translates to about 2.1 million HIV-1-infected individuals in the country. 4 As on September 9, 2016, 42,263 adults were alive and receiving ART through the free ART program offered by the National AIDS Control Organization (NACO), which was started in 2004 in the country. 5 The standard first-line regimen of the National ART program includes two nucleoside reverse transcriptase inhibitors (NRTIs), that is, zidovudine or stavudine plus lamivudine, and one non-nucleoside reverse transcriptase inhibitor (NNRTI), nevirapine (NVP) or efavirenz (EFV). Protease inhibitors (PIs) are provided as a second-line treatment option when the first-line regimen fails. Emergence of drug resistance is a major obstacle to the success of ART.
The success of therapeutic strategies and prevention programs would be greatly hindered if the rates of transmission of HIV-1 strains with drug resistance mutations (DRMs) are high. As rapid scale-up of ART is known to be associated with an increase in rates of transmission of DRMs, this study was undertaken keeping in mind the public health benefits that could be obtained from the findings of the study particularly in resource-limited settings such as India where routine drug resistance testing is not a standard practice.
This study is an attempt to determine the prevalence and pattern of primary DRMs in a cohort of therapy-naive HIV-1-infected individuals from a representative population from Chennai, South India. The study was undertaken with the approval of the Institutional Ethics Committee of NIRT (NIRT-IEC 2011001), and was carried out as a retrospective cross-sectional study using archived remnant plasma samples that were collected from HIV-1-infected individuals who attended the ART Centre at the Kilpauk Medical College and Hospital, Chennai, India, during the period April 2011 to September 2012. All study subjects were asymptomatic, naive to ART, and were within 3 years of diagnosis of HIV infection at the time of sample collection. The HIV infection status was determined as per NACO guidelines. 6 Detailed treatment history was obtained from all individuals, and those subjects, who reported no prior exposure to ARV drugs, were considered to be ART naive. Criteria that are used to define recently infected populations such as women with no previous pregnancy, 7 BED capture enzyme immunoassay analysis 8 and serial HIV testing to document seroconversion 9 were not considered in this study. However, to rule out late stages of disease among the study population and ensure recent infection fairly accurately, the study took into account the CD4 cell count (Mean: 427 cells/μL) and the time period between diagnosis and HIV drug resistance (HIVDR) testing (mean: 3.06 years). A study by Lodi et al. reported that the median time from seroconversion to a CD4 count of <350 cells/mm3 was 4.19 years. 10 The clinical and demographic details of the subjects are summarized in Table 1. For all study subjects HIV-1 viral load (VL) testing was performed using the COBAS Ampliprep and COBAS Taqman version 2.0 (Roche Molecular Systems, Inc., Branchburg, NJ) and CD4+ T cell count was estimated by flow cytometry using the BD FACS Count flow cytometer (BD Biosciences).
Characteristics of the Study Population
HIV-1 RNA was extracted from plasma of 62 HIV-1-infected ART-naive individuals using the QIAamp viral RNA extraction kit (Qiagen, Valencia, CA). Polymerase chain reaction (PCR) amplification and sequencing of the partial HIV-1 pol gene that spans the entire protease and approximately two-thirds of the reverse transcriptase (RT) genes was performed using the primers previously published.
11
PCR products were purified and sequenced using an ABI PRISM 3100 Genetic Analyzer (Applied Biosystems, Foster City, CA). Sequences were assembled and analyzed using Seqscape software V 2.5 (Applied Biosystems). For this survey, the sequences were analyzed using the calibrated population resistance (CPR) tool of the Stanford University HIV Drug Resistance Database.
12
Analyses were conducted using the 2009 World Health Organization (WHO) Surveillance Drug Resistance Mutations (SDRMs) list included in the tool. Subtype of the HIV-1 isolates was identified using the Stanford University's HIV drug resistance database, REGA HIV-1 subtyping tool version 3.0, and by phylogenetic analysis with reference sequences. Phylogenetic analysis for determining HIV-1 subtype was performed by aligning the study viral sequences with the reference sequences obtained from HIV Los Alamos Database using muscle alignment tool in the
A total of 62 HIV-1 pol gene sequences were amplified. Sequences of 53 (85%) out of the 62 amplified products were taken for analysis; 9 sequences could not be aligned fully due to poor quality of the sequences and were excluded from analysis. Out of the 53 samples, 19 (35.84%) were from men and 34 (64.1%) were from women. The mean age of the study population was 35 years [median: 35; 95% confidence interval (CI): 33.32–37.05]. The mean duration between the time of diagnosis of HIV infection and the time of HIVDR testing was 3.06 years (median: 3; 95% CI: 2.58–3.55). The median CD4 count was 378 cells/μL (mean: 427; 95% CI: 356–498) and the median HIV VL was 55,600 copies/mL (mean: 1, 56,869; 95% CI: 94,964–2, 18,773). Forty-one individuals (77.35%) had VL >10,000 copies/mL and 10 (18.86%) had VL between 1,000 and 10,000 copies/mL, a value considered as detectable viremia according to WHO recommendations; for one sample, there was no VL test result available and another study participant had a HIV-1 VL of 400 copies/mL. According to CPR, SDRM was detected in 6/53 (11.3%) sequences (Table 2); all isolates belonged to subtype C. Mutations to NNRTIs were the most frequent, seen in 8.3% (4/48) of sequences, with K101E mutation seen in 4.1% (2/48) of individuals. K101E mutation reduces susceptibility to NVP by 3- to 10-fold, to Effavirenz (EFV) by 1- to 5-fold, and to Etravirine (ETR) and Rilpivirine (RPV) by about 2-fold. One sequence had K103N mutation that imparts resistance to the NNRTI drugs, EFV and Nevirapine (NVP). Another sequence had the Y188C/Y, a major NNRTI DRM that is known to confer high-level resistance to the same class of drugs. The prevalence of TDRM to the PI class was 4.1% (2/49). Characteristics of the samples presenting SDRMs are shown in Table 3. No NRTI SDRM was identified in this study. The WHO 2009 mutation list option was chosen to identify SDRMs in the CPR program.
Sequence and Surveillance Drug Resistance Mutation Quality Assessment Table
The proportion of sequences with SDRMs generated by the CPR tool has been mentioned in Table 2. Fifty-three input sequences were fed into the CPR tool for SDRM evaluation; two RT and one PR sequences were filtered by the QA according to the SDRM quality assessment exclusion criteria by the CPR tool.
CPR, calibrated population resistance; NNRTIs, non-nucleoside reverse transcriptase inhibitors; NRTI, nucleoside reverse transcriptase inhibitor; PI, protease inhibitor; PRRT, protease, reverse transcriptase; QA, quality assessed; RT, reverse transcriptase; SDRMs, surveillance drug resistance mutations.
Characteristics of the Samples Presenting Surveillance Drug Resistance Mutations
The varying levels of resistance rendered by the resistance mutations have been ear-marked with a greater number of stars implying high-level resistance as to only one star indicating potential low level of resistance.
Intermediate resistance.
Low-level resistance.
Potential low-level resistance.
High-level resistance.
ATV/r, Atazanavir/ritonavir; EFV, efavirenz; FPV/r, Fosamprenavir/ritonavir; IDV/r, Indinavir/ritonavir; LPV/r, Lopinavir/ritonavir; NFV, Nelfinavir; NVP, nevirapine; SQV/r, Saquinavir/ritonavir; TPV/r, tipranavir.
In addition, several polymorphic amino acid substitutions were observed in >50% of the protease and reverse transcriptase (RT) sequences. The common polymorphisms seen were at codon positions 12 (92%), 15 (82%), 19 (100%), 36 (100%), 41 (86%), 63 (92%), 69 (98%), and 89 (75.5%) in the Protease (PR) gene, and at codon positions 35 (100%), 36 (85.7%), 39 (100%), 48 (91%), 60 (97.9%), 121 (83%), 122 (95%), 135 (84.7%), 162 (59%), 173 (100%), 177 (94%), 200 (100%), 207 (95.9%), 211 (67%), and 245 (91%) in the RT gene. A comparative analysis was done between the rate of polymorphisms in the PR and RT sequences of our study isolates with the universally established subtype C specific polymorphisms. The rate of polymorphisms was found to be significantly different (p < .0001) from universally established subtype “C”-specific polymorphisms at the 19th position of the PR region and 60th, 121st, and 122nd positions in the RT gene of the study sequences. The differences observed in the polymorphisms seen in this study as compared to the universally defined polymorphisms could be attributed to the host genetic differences and the differences in host immune responses between different ethnic populations.
The sequence that had the K103N NNRTI DRM was from a 26-year-old woman. Previous pregnancy status could not be verified in this individual, hence it may be presumed that DR might have emerged as a result of previous exposure to NNRTIs during prevention of mother-to-child transmission (PMTCT) prophylaxis. V82LV, a PI mutation that confers intermediate resistance to Tipranavir (TPV), was also observed in one study participant. The CD4 count of this patient was 68 cells/μL and VL was 7,87,443 copies/mL, suggesting the possibility of a chronic infection and undisclosed/unknown ARV exposure sometime between seroconversion and HIVDR testing.
All the study subjects were found to be infected with HIV-1 subtype C virus, based on subtype analysis performed using the Stanford and REGA subtyping tool. Sequences with gaps and missing regions were removed before the alignment process and among the 46 HIV-1 partial pol gene sequences included in the phylogenetic analysis, all samples clustered phylogenetically with HIV-1 subtype C (Fig. 1), the predominantly circulating subtype in India. Primary HIVDR is clearly associated with the risk of early virologic failure. Although the study identified a moderate level of major HIVDR, it should be assumed that there could be an increase in the HIVDR transmission at the population level, as the vast majority of the study participants reported heterosexual sex as the main factor for HIV acquisition. Balakrishnan et al., 13 had earlier reported 20% major PI DRMs, 6% NRTI DRMs, and 14% NNRTI DRMs among drug-naive South Indian patients receiving medical care in Chennai, India, in 2002–2003. The results of the survey conducted among newly diagnosed VCTC clients in Mumbai showed <5% prevalence of transmitted HIVDR to all ARV drug classes. 14 Another study conducted in an ART-naive North Indian population published in the year 2008 15 identified PI, NRTI, and NNRTI DRMs in 14.29%, 6.12%, and 32.65% of the sequences, respectively. Studies conducted in western India have reported 10% drug-associated mutations. 16 Several limitations of the study do exist. We do not have the information about the exact time of infection for the patients and, therefore, we could not rule out the possibility of reversion of mutant strains back to the wild type before analysis. Another limitation is that the samples used for the drug resistance testing for the study were collected in the year 2011–2012; therefore, the isolates may not reflect the current circulating strains in the country. The use of population-based sequencing method for drug resistance genotyping in the study is also one of the limitations as this methodology is known to miss the minority variants that might affect the treatment outcome.
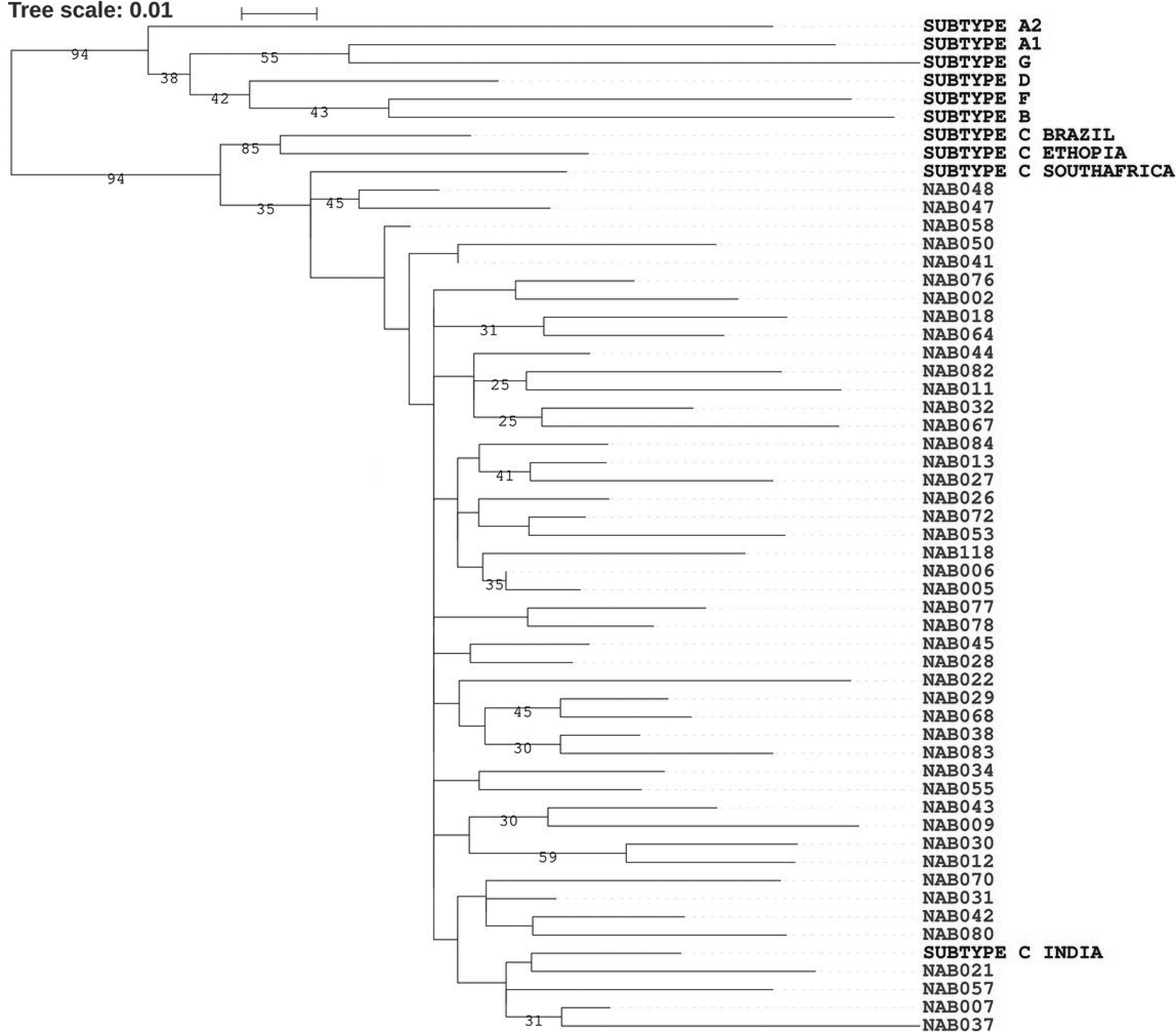
Phylogenetic analysis of HIV-1 pol gene (partial) sequences isolated from Chennai, South India.
In conclusion, our study found an overall prevalence of 11.3% of any SDRMs in the local population. In addition, our study found that 4 out of 48 patients eligible for first-line ART, harbored strains that were resistant to drugs belonging to the NNRTI regimen. However, the good news is that there were no major DRMs to both the NRTI and PI drug classes in this cohort. Overall, we observed a moderate level of TDR in our population according to WHO survey guidelines. With the scale-up of ART in the country, emergence of HIVDR is inevitable. Population-based HIVDR surveillance combined with local small surveys along with ART program monitoring and evaluation activities are critical for the effectiveness of the current ART program and to identify factors requiring optimization to minimize the emergence and transmission of HIVDR.
Sequence Data
Fifty-two nucleotide sequences of RT and PR genes were submitted to GenBank (accession nos. MK330780–MK330831).
Footnotes
Acknowledgments
The authors wish to acknowledge the Indian Council of Medical Research (ICMR) and the individuals who participated in the study.
Author Disclosure Statement
No competing financial interests exist.