
Abstract
Bali, the first province to report a case of HIV in 1987, was placed sixth among Indonesian provinces with the highest cumulative number of HIV cases in 2017. As a popular tourist destination, the spread of genetic variants of HIV through international travel may become a cause for concern in Bali. Tourism is mostly concentrated in south Bali; thus, HIV in less popular regions in north Bali, such as Buleleng Regency, may have viral characteristics different from that in south Bali. Forty-three protease (PR), 40 reverse transcriptase (RT), 27 gag, and 23 env genes were sequenced from 48 samples derived from antiretroviral treatment-experienced individuals. Subtyping revealed CRF01_AE as the dominant circulating recombinant form of HIV-1 in north Bali. Although no major mutation was detected in PR genes, several major mutations were identified in 4 out of the 40 RT genes (10%), indicating the emergence of HIV-1 drug resistance in this region.
The Joint United Nations Program on HIV/AIDS (UNAIDS) estimated that 36.9 million individuals were living with HIV globally in 2017. 1 In December 2017, Indonesia reported 280,623 cumulative cases of HIV infection. The first case of HIV infection in Indonesia was documented in Bali in 1987. With 17,024 cases of HIV infection, Bali was placed sixth among Indonesian provinces with the highest cumulative number of HIV cases. 2
HIV exhibits large genetic variability due to the high mutation and recombination rates of the reverse transcriptase (RT) enzyme, together with a high rate of virus replication. HIV type 1 (HIV-1), which is responsible for most of the global HIV pandemic, comprises four groups: group M (major), group O (outlier), group N (nonmajor, nonoutlier), and new group P (pending). Group M, the pandemic group of HIV-1, has been further divided into subtypes A to K. Besides these subtypes, circulating recombinant forms (CRFs) and unique recombinant forms, as a result of recombination between subtypes, have also been identified in group M.
3
To date, 98 CRFs have been recorded in the Los Alamos HIV database (
Subtypes and CRFs may differ in the rates of disease progression and viral transmission. HIV diversity also affects diagnostic and viral load measurements, and has an impact on responses to antiretroviral treatment (ART) as well as the emergence of drug resistance-associated mutations 3 ; therefore, it is important to monitor circulating HIV-1 subtypes and CRFs in regions for the prevention and control of HIV.
The Indonesian Ministry of Health reported that 91,369 individuals living with HIV/AIDS were being treated with ART in December 2017, with 88,386 receiving a first-line regimen and 2,983 receiving a second-line regimen. 2 First-line ART regimens comprise two nucleoside RT inhibitors (NRTIs) and a non-nucleoside RT inhibitor, whereas two NRTIs plus a ritonavir-boosted protease (PR) inhibitor are adopted for second-line regimens. 8 ART improves not only the survival rates and quality of life of HIV-infected individuals, but also reduces HIV transmission 9 ; however, acquired and transmitted HIV drug resistance may compromise ART. 10 Drug resistance is associated with suboptimal virological suppression, subsequent immunological decline, and poor clinical outcomes. 10
Travel and tourism are associated not only with HIV-1 dissemination around the world, but also the spread of genetic variants. 11 Bali is a popular tourism destination in Indonesia. Tourism activities in Bali are mostly concentrated in south Bali, including Badung Regency, Denpasar city, and Gianyar Regency, whereas Buleleng Regency located in north Bali is a less popular location for international tourism. 12 Previous studies that focused on Gianyar Regency and Denpasar city in Bali identified CRF01_AE as the major cause of infection, and major drug resistance mutations (DRMs) in the RT gene were detected in 25.8% of ART-experienced individuals. 7 The genotypic characteristics of HIV-1 circulating in tourism-concentrated regions may differ from those in regions less popular for tourism; however, limited information is currently available on HIV-1 subtypes and the prevalence of DRM outside south Bali. Therefore, this study aimed to characterize HIV-1 subtypes/the distribution of CRFs as well as the appearance of DRM among ART-experienced individuals in Buleleng Regency, Bali.
Ethical approval for this study was obtained from the Ethics and Law Committee of Universitas Airlangga Hospital (ethical approval no. 033/KEH/2016) and the Institutional Ethics Committee of Kobe University Graduate School of Medicine (approval no.: 784). Sixty-three HIV-1-infected individuals currently under ART were recruited from the Voluntary Counselling and Testing Clinic of Buleleng Regency General Hospital, Bali. Five milliliters of ethylenediaminetetraacetic acid-anticoagulated peripheral blood was collected from study participants in July and August 2017, with written informed consent being obtained from each participant before the procedure. DNA was then extracted from whole blood samples using the Wizard Genomic DNA Purification Kit (Promega, Madison, WI). Demographic and clinical data on study participants were retrieved from medical records and given in Table 1.
Demographic and Clinical Data of ART-Experienced Individuals in Buleleng Regency, Bali
3TC, lamivudine; ART, antiretroviral treatment; AZT, zidovudine; EFV, efavirenz; NVP, nevirapine; TDF, tenofovir.
Viral pol genes encoding full-length PR and RTC genes and partial fragments of the gag and env genes were amplified from DNA extracted from peripheral blood samples by the nested polymerase chain reaction (PCR) using ExTaq (Takara Bio, Shiga, Japan) and the following primers. The primers DRPRO5, 5′-AGACAGGYTAATTTTTTAGGGA-3′ [corresponding to nucleotides (nt) 2074–2095 of the HIV-1 reference strain, HXB2 (GenBank accession no. K03455)] and DRPRO2L, 5′-TATGGATTTTCAGGCCCAATTTTTGA-3′, (nt 2716 to 2691) were used in first PCR for the amplification of the PR gene, and the primers DRPRO1M, 5′-AGAGCCAACAGCCCCACCAG-3′ (nt 2148 to 2167) and DRPRO6, 5′-ACTTTTGGGCCATCCATTCC-3′ (nt 2611 to 2592) were used for nested PCR. The primers RT1L, 5′-ATGATAGGGGGAATTGGAGGTTT-3′ (nt 2388 to 2410) and GPR2M, 5′-GGACTACAGTCYACTTGTCCATG-3′ (nt 4402 to 4380) were used in first PCR for the amplification of the RT gene, whereas RT7L, 5′-GACCTACACCTGTCAACATAATTGG-3′ (nt 2485 to 2509) and GPR3L, 5′-TTAAAATCACTARCCATTGYTCTCC-3′ (nt 4309 to 4285) were used for nested PCR. The primers H1G777, 5′-TCACCTAGAACTTTGAATGCATGGG-3′ (nt 1231 to 1255), and H1P202, 5′-CTAATACTGTATCATCTGCTCCTGT-3′ (nt 2352 to 2328) were used in first PCR for the amplification of the gag gene encoding Gag p24, whereas H1Gag1584, 5′-AAAGATGGATAATCCTGGG-3′ (nt 1577 to 1595) and G17, 5′-TCCACATTTCCAACAGCCCTTTTT-3′ (nt 2040 to 2017) were used for nested PCR. The primers M5, 5′-CCAATTCCCATACATTATTGTGCCCCAGCTGG-3′ (nt 6858 to 6889), and M10, 5′-CCAATTGTCCCTCATATCTCCTCCTCCAGG-3′ (nt 7661 to 7632), were used in first PCR for the amplification of the C2-V3 regions of the env gene, whereas M3, 5′-GTCAGCACAGTACAATGIACACATGG-3′ (nt 6948 to 6973), and M8, 5′-TCCTTGGATGGGAGGGGCATACATTGC-3′ (nt 7547 to 7521), were used in nested PCR. Successfully amplified viral genes were then subjected to a sequence analysis performed by Macrogen Japan (
The sequencing data of 43 PR genes (297-bp; nt 2253 to 2549), 40 RT genes (1680-bp; nt 2550 to 4229), partial fragments of 27 gag genes encoding Gag p24 (381-bp; nt 1627 to 2007), and partial fragments of 23 env genes spanning the C2-V3 region (390-bp; nt 7020 to 7409) were obtained from 48 blood samples. We failed to amplify viral genes from the remaining 15 samples presumably due to the low quality of DNA samples. The nucleotide sequences of these PR, RT, gag, and env genes have been registered in the GenBank database under accession nos. MK442756-MK442793, MK442795, MK442796, MK442798, MK442800-MK442835, and MK442837-MK442892.
HIV-1 subtyping was conducted using the Recombinant Identification Program (RIP) available on the HIV sequence database website (
Viral subtyping revealed that 47 samples (97.9%, 47/48) were classified as CRF01_AE, whereas one remaining sample was classified as a recombinant of CRF01_AE and CRF02_AG (Fig. 1). The results obtained suggested that CRF01_AE is dominant in Buleleng Regency, Bali, similar to other regions in Indonesia as well as in Southeast Asian countries.
3
–7
The results of a blast search (
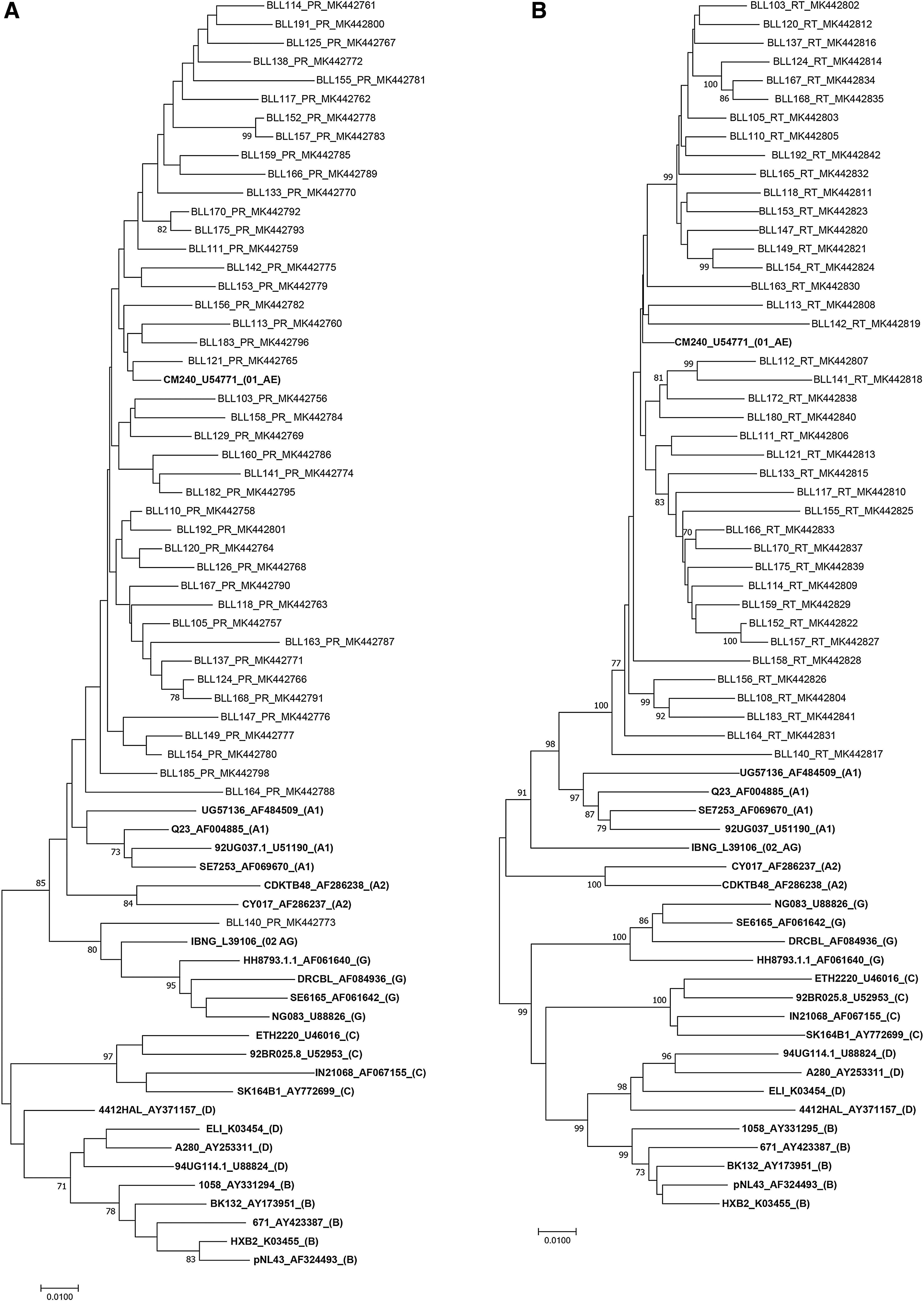
Phylogenetic tree analysis of HIV-1 PR, RT, gag, and env gene sequences collected in Bali, Indonesia. Phylogenetic trees were constructed for the HIV-1 PR

The appearance of DRMs in successfully sequenced PR and RT genes was investigated according to the International Antiviral Society-USA (IAS-USA) panel. 15 No major mutation was detected in PR genes; however, several drug resistance-associated minor mutations were identified. Among 43 PR genes, 6 (14%) contained L10I/V [amino acid substitution from leucine (L) to isoleucine (I) or valine (V) at position 10 in the PR gene], 15 (34.9%) G16E, 21 (48.8%) K20R/I, 1 (2.3%) L33F, 43 (100%) M36I, 1 (2.3%) I62V, 9 (20.9%) L63P, 40 (93%) H69K, 7 (16.3%) V77I, 8 (18.6%) V82I, 39 (90.7%) L89M/I, and 10 (23.3%) I93L. These mutations potentially affect viral susceptibility to ritonavir-boosted atazanavir (ATV/r), ritonavir-boosted darunavir (DRV/r), ritonavir-boosted fosamprenavir (FPV/r), ritonavir-boosted indinavir (IDV/r), ritonavir-boosted lopinavir (LVP/r), nelfinavir (NFV), ritonavir-boosted saquinavir (SQV/r), and ritonavir-boosted tipranavir (TPV/r). 15
Several DRMs were identified in RT genes derived from six patients, four of whom showed major mutations. The demographic characteristics of individuals from whom drug resistance-associated major mutations were detected in RT genes are given in Table 2. The most frequent major mutation found was G190A (7.5%), followed by M184V (5%). Other major mutations with a frequency of 2.5% each were K65R, D67N, K70R, K101E, E138A, Y181C, and Y188L. These mutations were associated with drug resistance to lamivudine (3TC), emtricitabine (FTC), didanosine (ddI), abacavir (ABC), stavudine (d4T), tenofovir (TDF), zidovudine (AZT), rilpivirine (RPV), efavirenz (EFV), etravirine (ETR), and nevirapine (NPV). 15 Minor mutations identified included A98G, V106I, and V179D, with a frequency of 2.5% each. The frequency of drug resistance-associated major mutations in Buleleng Regency in north Bali was lower than that reported previously in Gianyar Regency and Denpasar city of south Bali. 7 Eight out of 31 RT genes (25.8%) isolated in south Bali contained major mutations, 7 in contrast to only 4 out of 40 RT genes (10%) isolated in north Bali.
Demographic Characteristics of and Drug Resistance-Associated Major Mutations in Reverse Transcriptase Genes Derived from ART-Experienced Individuals in Buleleng Regency, Bali
The subtype of the RT gene was assigned based on RIP and phylogenic analyses.
Drug resistance mutations were based on guidelines published by the International Antiviral Society-USA (IAS-USA).
NRTIs, nucleoside RT inhibitors; nNRTI, non-nucleoside RT inhibitor; PR, protease; RT, reverse transcriptase; RIP, recombinant identification program.
In summary, this study identified CRF01_AE as the dominant CRF in Buleleng Regency, Bali, similar to other regions in Indonesia, including south Bali. The presence of major drug resistance-associated mutations in RT genes suggests the emergence of HIV-1 drug resistance among ART-experienced individuals, particularly those receiving first-line therapy. Any major drug resistance-associated mutation in RT genes needs to be taken into consideration because the mutation may have an impact on the effectiveness of ART, and continuous monitoring needs to be performed to address this issue.
Footnotes
Acknowledgments
This study was supported by Kementerian Riset, Teknologi, dan Pendidikan Tinggi Republik Indonesia through the Pendidikan Magister menuju Doktor untuk Sarjana Unggul (PMDSU) scholarship. This study was also supported by the Japan Initiative for the Global Research Network on Infectious Diseases (J-GRID) from the Ministry of Education, Culture, Sport, Science and Technology in Japan, and the Japan Agency for Medical Research and Development (AMED); the Institute of Tropical Disease as the Center of Excellence (COE) program by Kementerian Riset, Teknologi, dan Pendidikan Tinggi Republik Indonesia; and the Tahir Professorship Grant from Dato' Sri Tahir of the Tahir Foundation. We sincerely thank the staff at the Voluntary Counselling and Testing Clinic of Buleleng Regency General Hospital, Bali, for their kind cooperation with this study.
Author Disclosure Statement
No competing financial interests exist.