
Abstract
Incidence of noncommunicable diseases (NCDs), including cardiovascular disease (CVD), cirrhosis, and non-AIDS-defining cancers (NADCs), have been associated with HIV viremia, CD4 cell counts, and CD4/CD8 ratio in persons living with HIV (PLWH). This study examined the importance of these markers to mortality risk following NCD diagnosis. We examined factors associated with mortality following incident CVD, cirrhosis, or NADCs in a clinical cohort of PLWH between 1998 and 2015. We calculated Kaplan–Meier estimates and used multivariable Cox proportional hazard models. We included 341 patients with NCDs (CVD = 169, cancer = 103, and cirrhosis = 67), of whom 129 died. Median age at NCD diagnosis was 49 years and median proportion of time before NCD with virologic suppression was 64%. Median survival after CVD was longer than for cancer or cirrhosis (11.6 years vs. 4.8 and 3.4 years, respectively; log rank test p < .001). In multivariable Cox proportional hazard models, higher CD4/CD8 ratio preceding NCD (adjusted hazard ratio [aHR] per 0.1 increase = 0.92 [95% confidence interval 0.85–0.99]) and higher CD4 nadir (aHR per 100 cells/μL = 0.84 [0.72–0.97]) were associated with decreased mortality risk. Neither CD4 cell count before NCD nor HIV viremia was statistically associated with mortality in adjusted models. When restricted to 116 patients with virologic suppression for ≥80% of time before NCD, only CD4 nadir was associated with mortality risk. Low CD4/CD8 ratio and CD4 nadir were associated with increased mortality risk after NCD, suggesting that prior immunosuppression or ongoing immune imbalance remain important for outcomes following serious NCDs.
Introduction
With the success of antiretroviral therapy (ART), persons living with HIV (PLWH) are surviving longer and the burden of morbidity and mortality is shifting from infectious to noncommunicable diseases (NCDs). 1 –3 Over time, risk of mortality following certain AIDS-defining illnesses and opportunistic infections has decreased due to the availability of effective HIV therapy. 4 Measures of HIV disease activity and progression, namely CD4 cell count and plasma HIV-1 RNA (viral load), are associated with survival following AIDS-defining illnesses and remain important predictors of overall survival among patients starting ART. 5 –8
Cardiovascular disease (CVD), non-AIDS-defining cancers (NADC), and cirrhosis have become leading causes of death among PLWH who receive ART. 1,3,9 These NCDs occur at increased frequency in PLWH and are associated with immunologic and virologic measures of HIV disease, including low CD4 cell count, low CD4/CD8 ratio, and HIV viremia. 10 –14 While HIV disease markers are associated with the development of CVD, cancer, and cirrhosis in PLWH, less is known of their role in outcomes following the development of these important comorbidities. Given their association with NCD incidence, we aimed to study immunologic and virologic measures associated with mortality following incident CVD, non-AIDS cancers, or cirrhosis diagnoses among PLWH in a clinical cohort. We hypothesized that CD4 cell count, CD4/CD8 ratio, and HIV viremia would be associated with mortality risk in patients following these NCDs.
Materials and Methods
This study included adult (age ≥18 years) PLWH enrolled in care at the Vanderbilt Comprehensive Care Clinic (VCCC) between January 1998 and December 2015. The VCCC provides specialty HIV care and primary care. Patients are routinely seen in clinic every 3–6 months. Research staff systematically abstract demographic, clinical, and laboratory data from the electronic medical record, including NCD diagnoses and dates of onset. Research and medical staff validate all cardiovascular, hepatic, and oncologic NCD diagnoses. Use of these data for research purposes was approved by the Vanderbilt Institutional Review Board.
Patients were included in this study if they had incident CVD, NADC (cancer), or cirrhosis diagnoses after clinic entry and in the period between 1998 and 2015. Patients with diagnoses recorded within the first 10 days of clinic entry were excluded as entered diagnoses were mostly likely to reflect prevalent disease. The earliest date of incident CVD, cancer, or cirrhosis was used as the baseline time point for analysis and beginning of observation follow-up time. The major NCDs of CVD, cancer, and cirrhosis were selected as they reflect end-organ disease with significant morbidity and mortality and are leading causes of death among adults living with HIV on ART. 3,9 CVD diagnoses included coronary artery disease events (myocardial infarctions, incident coronary artery atherosclerosis diagnosed by angiography or revascularization surgery, or diagnosed ischemic cardiomyopathy), cerebrovascular events, and peripheral vascular disease. Cancers excluded AIDS-defining cancers, in addition to nonmelanoma skin cancers (the latter due to their lower risk of mortality and major morbidity). Cirrhosis of any cause was included. Patients with prevalent CVD, non-AIDS cancers (excluding nonmelanoma skin cancer), or cirrhosis at the time of clinic entry were excluded. Patients contributed observation time until death; December 31, 2015; or the 365 days after their last clinic visit if their last visit was before January 1, 2015, and at which point the patient was considered lost to follow-up.
The primary outcome of interest was all-cause mortality. Mortality data are collected in the clinic from the medical record or as recorded by reports received from patient families, friends, partners, hospice services, or other health care services in the area. In addition, clinic patient lists are cross-matched with the National Death Index periodically to validate vital status.
We examined the following immunologic and virologic measures before NCD (baseline): CD4 cell count (cells/μL), CD4 cell count nadir (cells/μL), CD4/CD8 ratio, and HIV-1 RNA (copies/mL). Baseline CD4, CD8, and HIV-1 RNA were defined as the closest value within 365–60 days before the NCD event. We used laboratory results that were a minimum of 60 days before the NCD to reduce the likelihood that values were affected by the NCD event itself. CD4 cell nadir was the lowest recorded value before NCD. HIV-1 RNA was examined as both a continuous variable (log10) and dichotomized into detectable and undetectable using a cutoff value of 400 copies/mL to account for temporal changes in measurement during the observation period. We additionally calculated the proportion of documented person-time since clinic entry with HIV-1 RNA <400 copies/mL at the time of NCD to account for differences in sustained virologic suppression, which would affect CD4 cell count and CD4/CD8 ratio.
We examined demographic and clinical covariates of patients at the time of NCD, stratified by NCD category. Demographic data included age at NCD, sex, race, and HIV transmission risk factor. Clinical data included chronic hepatitis B or hepatitis C viral infections, prevalent diabetes and advanced chronic kidney disease, prevalent mood disorders (including major depression and bipolar disorders), history of substance abuse at any time during clinic follow-up (including illicit drugs, alcohol, and tobacco use), anemia at NCD (defined as hemoglobin <11.8 g/dL for females and <14 g/dL for males), years duration of ART before NCD, years in clinic at time of NCD, and calendar year of NCD. Differences in demographic and baseline clinical covariates were compared by NCD category (CVD, cancer, and cirrhosis) using Kruskal–Wallis test for continuous variables and chi-square test for categorical measures.
We first examined differences in mortality following NCD by Kaplan–Meier curves and log-rank tests. We used multiple imputation, using five multiplications, to account for missing laboratory data preceding NCD diagnosis in survival analyses, including CD4 nadir (3.2% missing), CD4 cell count (10.9% missing), CD4/CD8 ratio (15.0% missing), HIV-1 RNA (11.1% missing), and hemoglobin (15.0% missing). Mortality differences by NCD category, immunologic measures (categorized), and virologic measures were examined by Kaplan–Meier curves and log-rank tests. Median survival time following CVD, cancer, and cirrhosis were calculated. As marked differences in mortality following CVD compared with cancer and cirrhosis were observed, examination of the association of demographics, laboratory, and clinical covariates and mortality in univariate and multivariable Cox proportional hazard models were stratified by NCD category in our primary analyses (i.e., a separate baseline hazard was fit for each NCD category). Variables included in multivariable analyses were immunologic measures of CD4 cell count before NCD diagnosis, CD4 nadir, CD4/CD8 ratio before NCD diagnosis, detectable viral load before NCD diagnosis, proportion of person-time since enrollment in the clinic with HIV-1 RNA <400 copies/mL before NCD, as well as age, sex, race, calendar year, and ART regimen (protease inhibitor-based vs. other) at NCD.
As immunologic measures are often highly dependent upon HIV viral activity, a secondary analysis was performed limited to those with virologic suppression of ≥80% of person-time in clinic before NCD to reexamine the association of immunologic measures and mortality. To explore differences of associations by the NCD categories, univariate Cox proportional hazard models for demographic, laboratory, and clinical variables and mortality by each NCD category were also performed.
Statistical analyses were performed using Stata 12.1 (Stata Corporation, College Station, TX). All p-values are two sided.
Results
Of the 5,454 total patients in care at the VCCC between 1998 and 2015, there were 341 patients with incident CVD, non-AIDS cancer (cancer), or cirrhosis diagnoses. Patient demographic, clinical, and laboratory characteristics at clinic entry of patients included and excluded in the analyses are shown in Supplementary Table S1. Overall, patients with incident CVD, cancer, or cirrhosis were older at clinic entry, had a higher prevalence of previous injection drug use and substance use, had higher prevalence of chronic hepatitis virus C or B, and had lower CD4 cell count, CD4 cell count nadir, and CD4/CD8 ratio at clinic entry. Included patients provided 1,260 person-years of observation time after NCD through December 31, 2015. Of the 341 patients, 169 (49%) had incident CVD, including 115 patients with coronary artery disease (68%), 46 (27%) with cerebrovascular accidents, and eight (5%) with peripheral vascular disease. There were 105 patients (30%) with incident NADCs excluding basal and squamous skin cancers. The most frequent cancer diagnoses included anal (n = 25), lung (n = 13), head and neck (n = 10), prostate (n = 8), and liver (n = 6). There were 67 patients (20%) with incident cirrhosis of any cause.
The demographic, laboratory, and clinical characteristics of the cohort are presented in Table 1. There were notable differences among patients by NCD type. Patients with incident cirrhosis were slightly younger at NCD diagnosis, more likely to have injection drug use as an HIV transmission risk factor, more likely to be coinfected with hepatitis B or hepatitis C viruses, more likely to be anemic, and more likely to not be on ART at baseline compared with those diagnosed with CVD or cancer. There were no statistically significant differences in sex, race, or prior history of diabetes, psychiatric disease, or substance abuse among the groups.
Patient Characteristics Preceding NCD Diagnosis
Data presented as N (%) or median (interquartile range).
p value results of Kruskal–Wallis test for continuous variables and Chi-square test for categorical variables.
Chronic kidney disease includes only stage IV or V disease.
Depression includes major depression disorder and bipolar affective disorder.
Anemia values available for 290 patients (85%).
CD4 cell count nadir available at time of NCD for 330 patients (97%).
CD4 cell count available at time of NCD for 304 patients (89%).
CD4/CD8 ratio available at time of NCD for 283 patients (83%).
HIV-1 RNA available at time of NCD for 303 patients (89%).
NCD, noncommunicable disease; CVD, cardiovascular disease; MSM, men who have sex with men; ART, antiretroviral therapy; PI, protease inhibitor; NRTI, nucleoside reverse transcriptase inhibitor; NNRTI, non-nucleoside reverse transcriptase inhibitor; INSTI, integrase strand transfer inhibitor.
Baseline immunologic and virologic measures by NCD category are also shown in Table 1; compared with those with CVD or cancer, patients with incident cirrhosis had lower CD4 cell count before NCD diagnosis but similar CD4/CD8 ratio and CD4 nadir. Compared with CVD and cancer patients, cirrhosis patients had higher baseline HIV-1 RNA. The median proportion of person-time with HIV-1 RNA <400 copies/mL before NCD was 64% and was similar across NCD groups.
Of the 341 patients included in our analyses, 129 (38%) died during follow-up. This included 45 (27%) of patients diagnosed with CVD, 46 (44%) of patients with cancer, and 38 (57%) of the patients with cirrhosis. We first examined overall survival following NCD using Kaplan–Meier curves. As shown in Figure 1, there were significant differences in survival by diagnosis (log rank test p < .001). The estimated median survival of patients following CVD diagnosis was 11.6 years, much longer than that of patients diagnosed with cancer (4.8 years) or cirrhosis (3.4 years). We also observed significant differences in survival by baseline immunologic and virologic measures (Fig. 2A–D). Including all NCD diagnoses, patients with lower CD4 nadir (Fig. 2A), lower CD4 cell count (Fig. 2B), lower CD4/CD8 ratio (Fig. 2C), and detectable viral load (HIV-1 RNA ≥400 copies/mL) (Fig. 2D) before NCD all had decreased survival.
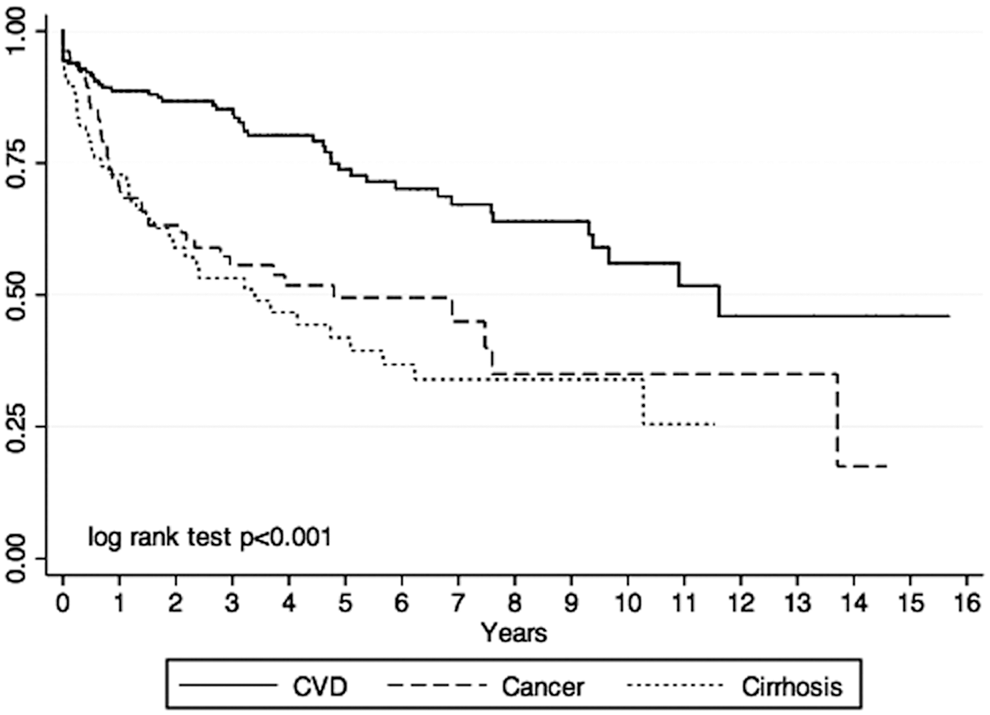
Survival following incident CVD, cancer, or cirrhosis.
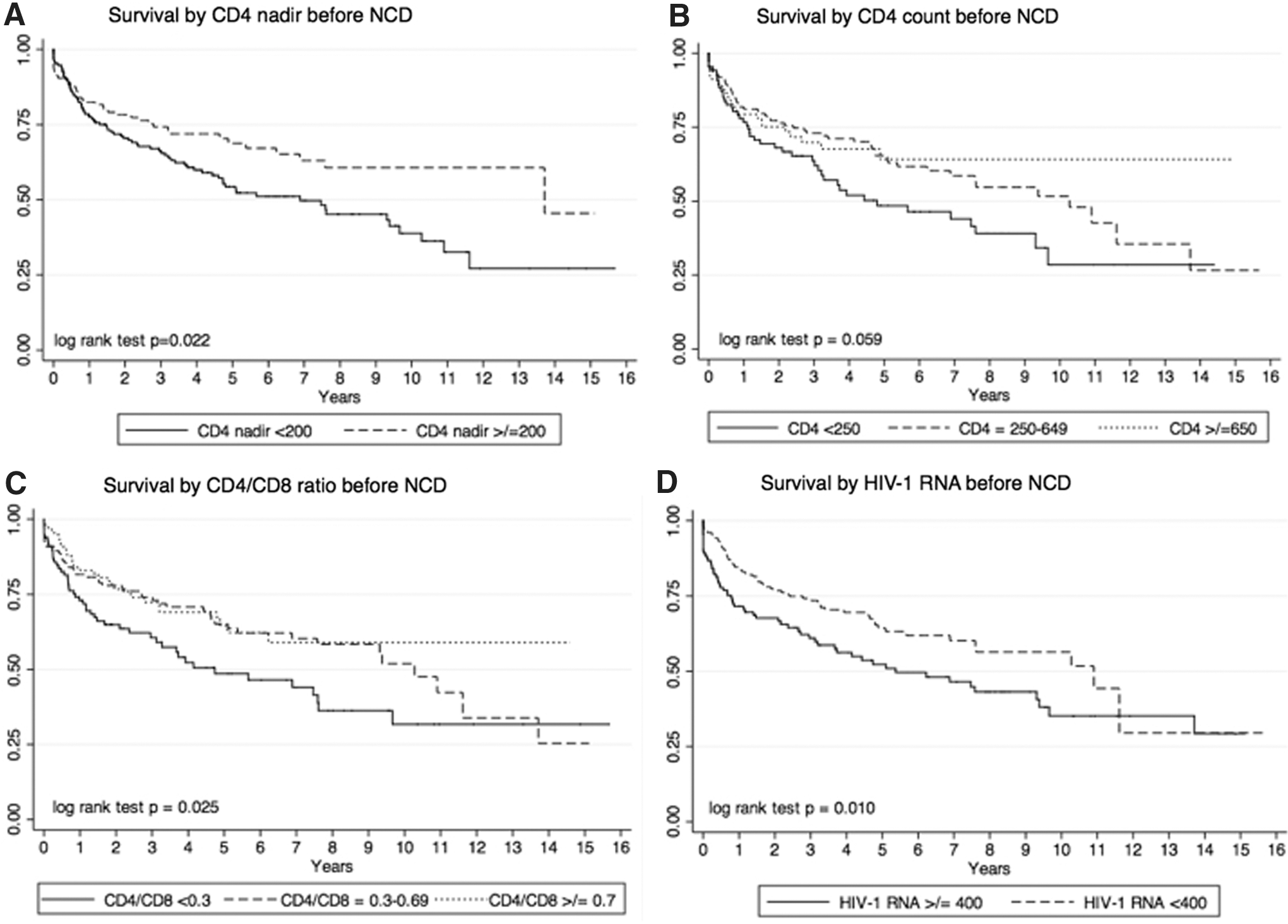
Survival following incident NCD by immunologic and virologic measures.
The results of the univariate and multivariable Cox proportional hazard models are shown in Table 2. In univariate analyses, higher CD4 nadir, absolute CD4 cell count, and CD4/CD8 ratio were all significantly associated with decreased risk of mortality. HIV-1 RNA <400 copies/mL before NCD diagnosis and higher proportion of time before NCD with HIV RNA <400 copies/mL were also associated with decreased mortality risk in unadjusted analyses. In multivariable analyses that also included baseline age, sex, race, presence of anemia, and calendar year, higher CD4/CD8 ratio and CD4 nadir remained significantly associated with decreased risk of mortality. The effects of virologic suppression before NCD were attenuated and no longer statistically significant in adjusted models. Aside from the immunologic and virologic measures, female sex, presence of anemia, and earlier calendar year of NCD diagnosis were statistically associated with increased risk of mortality in the multivariable model. Persons on an ART regimen containing a protease inhibitor had a decreased risk of mortality compared with those on an ART regimen without a protease inhibitor, including those not on ART. There was no meaningful association between age or race and risk of death after inclusion of confounders. Lastly, tests for interactions by HIV-1 RNA <400 copies/mL before NCD and proportion of person-time with virologic suppression before NCD with demographic and clinical variables in adjusted models were all nonsignificant (p > .05).
Univariate and Multivariable Cox Proportional Hazard Models for Patient Characteristics Preceding NCD and Risk of Death
Cox proportional hazard models stratified for NCD category to allow for differing baseline hazards by diagnosis.
HR, hazard ratio; aHR, adjusted hazard ratio; CI, confidence interval.
As immunologic measures are often strongly affected by the duration of virologic suppression, we conducted a secondary analysis that was limited to only those patients (n = 116, 28 deaths) with documented HIV-1 RNA <400 copies/mL for ≥80% of person-time in clinic before NCD (Table 3). When analyses were restricted to only these patients, increasing CD4 nadir remained significantly associated with decreased risk of death. Neither CD4 cell count nor CD4/CD8 ratio were statistically associated with risk of mortality. Female sex remained associated with increased risk of mortality in the secondary analysis, although did not quite reach statistical significance in multivariable models.
Univariate and Multivariable Cox Proportional Hazard Models for Patient Characteristics and Risk of Death, Limited to Only Those Patients with HIV-1 RNA <400 Copies/mL for At Least 80% of Observation Time Before NCD
Cox proportional hazard models stratified for NCD category to allow for differing baseline hazards by diagnosis. Models include 116 persons, 28 deaths.
Lastly, results of an unadjusted analysis of key covariates and risk of death by NCD diagnosis are shown in Supplementary Table S2. CD4 nadir, CD4 cell count before NCD, and CD4/CD8 ratio were inversely associated with risk of mortality for each of the three NCDs, although only reaching statistical significance for cancer and cirrhosis. HIV RNA <400 copies/mL was associated with decreased risk of mortality for CVD and cirrhosis diagnoses, with attenuated association lacking statistical significance in the case of cancer.
Discussion
In this observational cohort study, we found that lower CD4/CD8 ratio and CD4 cell count nadir at the incident CVD, cancer, or cirrhosis diagnosis were independently associated with increased risk of mortality. This association persisted for CD4 nadir among those patients with a documented high proportion of person-time with virologic suppression before NCD event. HIV viremia and CD4 cell count before NCD were not statistically associated with risk of mortality in multivariable models. These findings suggest that the long-term effects of prior immunosuppression or ongoing immune imbalance, as suggested by CD4/CD8 ratio, may be important biomarkers for outcomes following serious NCD events in PLWH.
The importance of HIV disease measures is underscored by persistent disparities in outcomes following CVD events, cancer, and cirrhosis diagnoses in PLWH compared with their uninfected peers, even after adjusting for notable confounders. 15 –18 However, only a limited number of studies have examined HIV laboratory measures as predictors of survival following NCDs. In a recent study examining risk of mortality after acute myocardial infarction or stroke, a prior history of AIDS was associated with higher in-hospital mortality and discharge to nonhospital, inpatient facilities, suggesting that persistent alteration in immune function may be important in CVD outcomes. 19 Studies examining survival following cancer diagnosis in PLWH have demonstrated the importance of immune status (reflected by CD4 cell count), CD4 nadir, and virologic activity as particularly important predictors of survival in both AIDS defining and NADCs. 20 –22 In a study of 650 PLWH with cancer in the Centers for AIDS Research Network of Integrated Clinical System cohort, higher CD4 lymphocyte count and achievement of HIV virologic suppression were associated with decreased risk of mortality in adjusted analyses. 21 Consistently, studies examining survival among PLWH coinfected with HCV with advanced-stage liver disease have also shown higher CD4 lymphocyte count, HIV virologic suppression, and receipt of ART to be associated with improved survival. 17,23
This is the first study to our knowledge to demonstrate the independent association of CD4/CD8 ratio and risk of mortality following NCDs. Our group and others have added to the growing evidence of CD4/CD8 ratio as an independent biomarker for risk of serious NCDs among PLWH. 11,24 –28 Translational studies have demonstrated that low CD4/CD8 ratio is associated with poor immune reconstitution following ART initiation and, in the setting of virologic suppression, persistent T cell activation and senescence. 29 –32 The ongoing immune activation as reflected by a low CD4/CD8 ratio is hypothesized to play a biologic role in the development of NCDs, particularly CVD and cancer. 28,33 In this study, the median CD4/CD8 ratio before diagnoses of CVD, non-AIDS cancer, or cirrhosis was <0.5 and did not meaningfully differ by diagnosis. The causes of low CD4/CD8 ratio in PLWH include not only depletion of CD4 T cells but also persistent expansion and activation of CD8 T cells. Studies have shown that coinfection by cytomegalovirus (CMV) may be an important driver of low CD4/CD8 ratio in both adults with and without HIV infection. 34 –36 In older adults without HIV infection, low or inverted CD4/CD8 ratio and CMV seropositivity have been associated with neurocognitive decline, frailty, functional decline, and death. 37 –39 Our finding of an inverse association between preceding CD4/CD8 ratio and mortality risk following diagnosis of CVD, cancer, or cirrhosis may reflect an “immunologic frailty” status. Just as physical measures of frailty have been associated with risk of death in adults with HIV, our findings show that low CD4/CD8 ratio may be an immunologic biomarker of vulnerability and risk of mortality following a stressor of incident NCD. 40,41 Patients with evidence of heightened T cell activation and senescence, as suggested by a low CD4/CD8 ratio independent of CD4 cell count, thus may be at increased risk not only for incident NCD but also poor clinical outcomes and mortality following those clinical events.
This study is novel in its description of mortality trends following NCDs. Our study demonstrated poor overall survival following cancer and cirrhosis diagnoses, with median survival less than 4 years. Our results are consistent with other studies that have individually examined mortality after these diagnoses. Importantly, survival following NADC diagnosis has been observed to be shorter than following AIDS-defining cancer diagnosis. 20,42 Mortality among HIV/HCV coinfected patients with end-stage liver disease has also been documented to be poor even with ART. 23 These trends were in contrast to what we observed for incident CVD diagnoses, where the median survival was greater than 10 years. Indeed, in a recent observational study from the D:A:D cohort, short-term survival following acute myocardial infarction in HIV-infected adults improved from 1999 to 2014, due to improvements in CVD treatments. 43 Our study also showed improved survival associated with later calendar year, consistent with this trend. In our study, we also observed an increased risk of mortality in adjusted analyses associated with female sex. Importantly, the D:A:D group also separately reported that among PLWH with CVD, women were less likely to receive interventions, such as lipid-lowering therapies and antihypertensives. 44 While CVD diagnoses were the most common incident NCD observed in our cohort, they were associated with improved survival, highlighting the need for additional therapies and interventions to improve patient outcomes following cancer and cirrhosis diagnoses. Work to identify and address additional disparities in NCD outcomes following NCD, such as sex, is also needed.
There are a few important limitations of this study. First, although our clinic population is diverse, results of this single-site study may not be generalizable to other populations of PLWH. CMV serology is not routinely obtained at the VCCC and thus we could not assess confounding by CMV coinfection. Additionally, the small number of patients included in our analysis limited our ability to examine immunologic and virologic predictors of mortality by individual NCD diagnoses using multivariable models. This study focused on immunologic and virologic measures of HIV disease prevention and risk of mortality. It is possible that other disease-specific markers of severity (such as MELD score for cirrhosis or tumor stage for cancer) or global measures of function (such as frailty or functional status) before NCD diagnosis are more strongly associated with mortality risk. 45 Lastly, given the small numbers of our study and limited cause of death data available, we examined all-cause mortality in this analysis and did not evaluate if mortality after NCD was due to the incident NCD, AIDS, or other causes. It is possible that the immunologic and virologic measures associated with HIV disease progression are differentially associated with AIDS-related and AIDS-unrelated deaths, although untangling cause of death data, even when available, is often challenging.
In conclusion, low CD4/CD8 ratio and low CD4 nadir were independently associated with mortality following incident CVD, cancer, or cirrhosis diagnoses in PLWH. CD4 cell count and HIV-1 RNA at the time of NCD were not associated with risk of death after controlling for these other variables. Efforts to identify causes and mediators of low CD4/CD8 ratio, such as understanding the biologic role of CMV and clinical outcomes, early initiation of ART, or particular ART regimens are needed. Our findings highlight the need for translational studies into the mechanisms and downstream biologic effects of low CD4/CD8 ratio and CD4 nadir in PLWH on ART. As PLWH continue to age and accumulate noninfectious, comorbid conditions, identifying patient and biologic factors associated with clinical outcomes is of increasing importance. Identifying patient characteristics associated with risk of mortality following NCD diagnoses, such as CD4/CD8 ratio, sex, and anemia, will also help in the development of secondary prevention and direct resources to those at greatest risk of poor outcomes. Further work to understand the biologic and behavioral factors associated with mortality after NCD and potential interventions to improve patient outcomes are urgently needed.
Footnotes
Acknowledgments
The authors recognize the efforts of Peter Rebeiro, Daniel Rasbach, Paul No, Henry Heaton, James Logan, Asghar Kheshti, and Fernanda Maruri for their contributions toward the collection and validation of noncommunicable disease diagnoses and death data from medical records.
Author Disclosure Statement
All authors of this study declare they have no competing interests.
Funding Information
This study was supported by grant funding by the National Institutes of Health: K23 AI120875 (J.L.C.) and K23 AI00700 (J.R.K.). This work was also supported in part by the NIH-funded Tennessee Center for AIDS Research (P30 AI110527).
Supplementary Material
Supplementary Table S1
Supplementary Table S2
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.