
Abstract
We report the case of a patient with a very profound CD4 T cell lymphopenia <20 cells/mm3 in the context of a primary HIV-1 infection, associated with both delayed HIV-specific antibody and CD8 T cell responses. A long-term immune reconstitution was observed after immediate initiation of antiretroviral therapy.
While the possible occurrence of opportunistic infections during HIV primary infection is well known, the CD4 T cell count does not usually drop <40 CD4/mm3 (range 40–1,542/mm3. 1 The CD4 cell count was described <20/mm3 in only two cases, one with Pneumocystis jiroveci coinfection 2 and the other in a hemophagocytic syndrome context. 3 After primary infection, the serology is usually positive except very early—about 20 days—after infection, 4 and HIV-specific CD4 T cell responses are normally rapidly detected after early onset of combined antiretroviral therapy (cART). 5
In this study we report a case of an HIV primary infection together with an exceptionally profound CD4 T cell lymphopenia and without severe documented coinfection. A delay in both seroconversion and T cell responses to HIV was observed, together with a well-documented successful immune restoration.
A 52-year-old Nigerian woman living in France was hospitalized for alteration of the general status. She had a heterosexual behavior at risk for HIV infection 3 months before in Nigeria. Fifteen days after arrival in France, she suffered from asthenia, oscillating fever, weight loss (−9 kg), microbiologically negative necrotic ulcer of the right tonsil, and oral candidiasis.
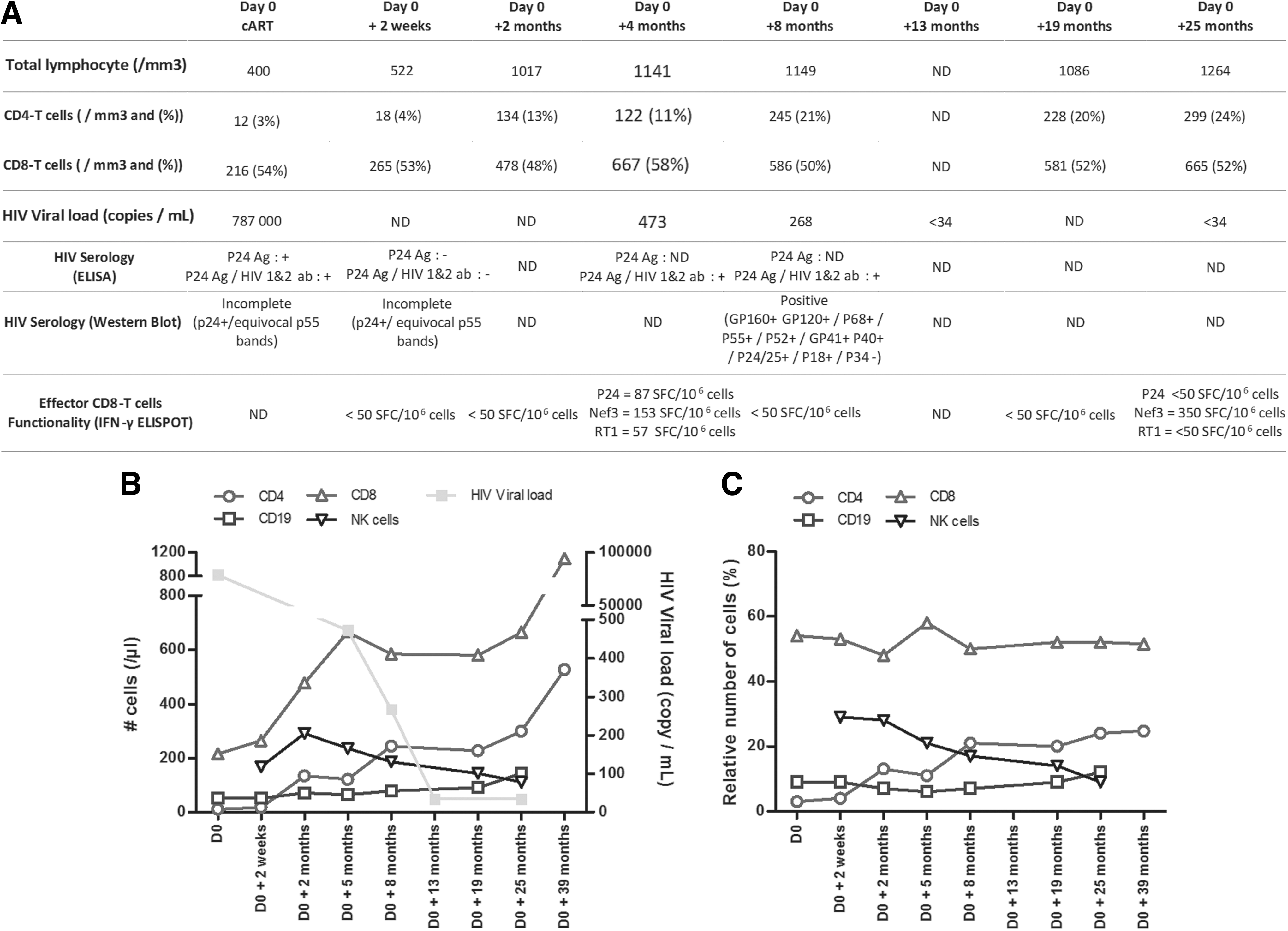
When hospitalized, enzyme-linked immunosorbent assay (ELISA) HIV serology suggested a positivity related to P24 antigen positivity alone, whereas Western blot (WB) showed an incomplete profile with positivity of the P24 and P55 bands (Fig. 1A). 6,7 The reverse transcriptase-polymerase chain reaction analysis confirmed HIV infection with a high viral load (VL; 787,000 copies/mL; Fig. 1A, B). HIV-1 strain was subtyped as CRF06_cpx. Genotypic resistance test showed a wild-type virus for reverse transcriptase and protease regions and an E157Q polymorphism in the integrase, with a non-CCR5 tropic strain. No other coinfection was found. The syphilis serology was negative and the virological analysis of the ulcer of the right tonsil was negative for Epstein-Barr virus (EB) and cytomegalovirus (CMV).
Successful T cell and antibody-specific immune reconstitutions after antiretroviral therapy in a patient with severe HIV primary infection.
Immunophenotyping revealed a major CD4 T cell defect (12/μL) together with a low CD8 T cell (216/μL) and a low B cell (52/μL) counts, contrasting with a normal natural killer (NK) cell count (168/μL) (Fig. 1A, B). The patient was treated within 3 days with fluconazole and tenofovir, emtricitabine and ritonavir boosted darunavir.
Clinical improvement was rapidly observed. Surprisingly, HIV-1 and HIV-2 serology and WB analysis performed 15 days after cART initiation showed negative results and an incomplete profile with a unique positivity at the P24 band and an equivocal P55 band (Fig. 1A). At month 8, both ELISA and WB serologies were fully positive. The HIV plasma load reached undetectability at month 13 of treatment (Fig. 1A, B).
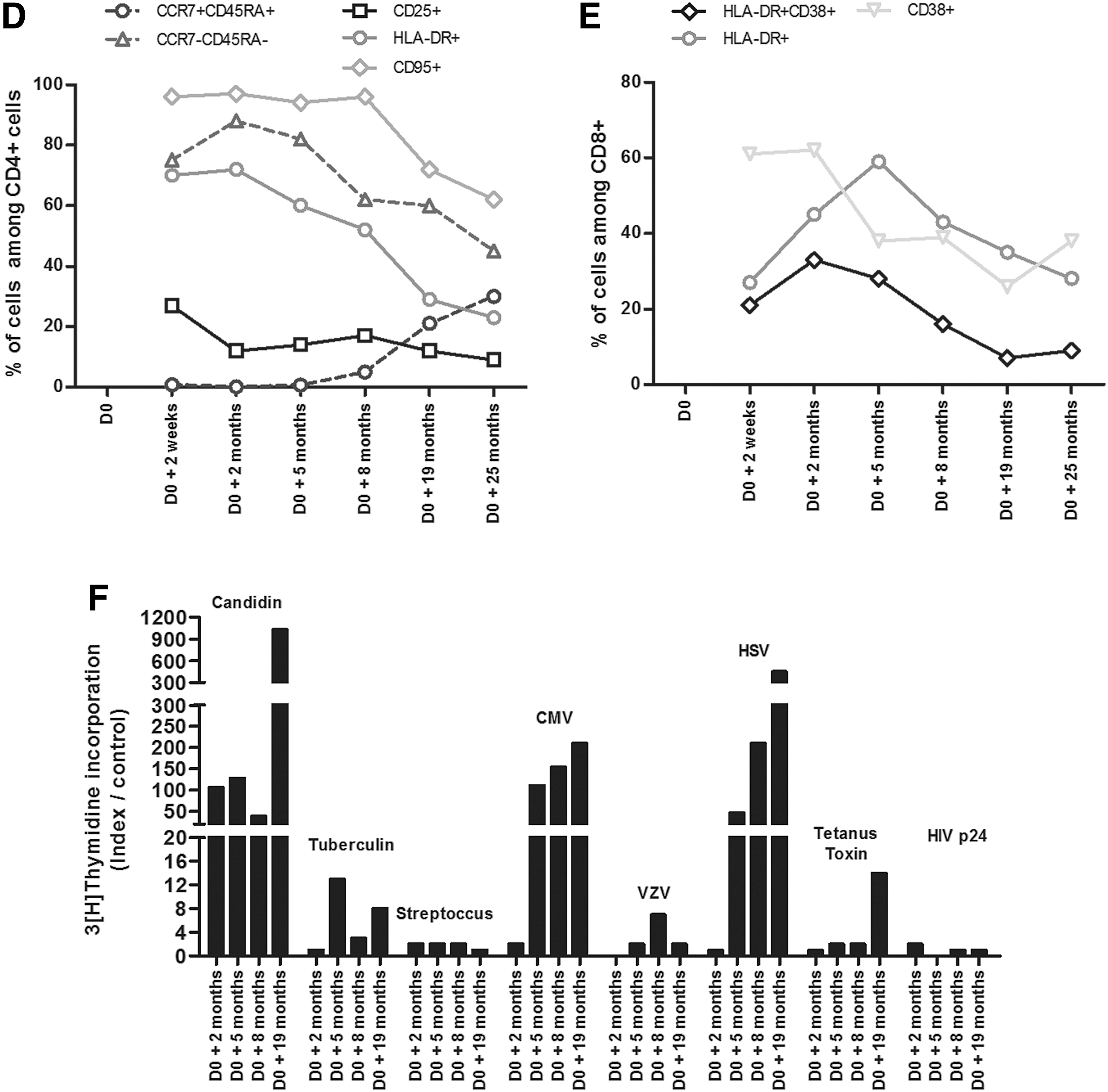
A slowly progressive CD4 T cell reconstitution was observed from 12/μL at D0 to 134/μL at 2 months, 245/μL at 8 months, 299/μL at month 25 and 527/μL at 39 month (Fig. 1B, C). Simultaneously, the total lymphocyte cell count increased from 400/mm3 at D0 to 1,264/mm3 at M25. The initial collapse of naive CD45RA+CCR7+CD4+ T cells (Fig. 1D) was followed by a subsequent increase at M25 post-cART (Fig. 1D). The in vitro T cell proliferation assays showed a lack of memory T cell responses to all recall antigens tested except for candidin at M2 post-cART (Fig. 1E). Five months after cART initiation, memory T cell responses to CMV and herpes simplex virus were restored, although without responses to the HIV-p24 antigen (Fig. 1E).
The CD8 T cell count also progressively increased (Fig. 1B). Activated CD8 T cells assessed by HLA-DR+CD38+ coexpression increased progressively up to M2, then gradually decreased reaching normal values at M19 (Fig. 1E). The HIV-specific effector memory CD8 T cells analyzed ex vivo by using an IFN-γ ELIspot assay against 15-mer overlapping peptides covering p24, p17, Nef, and RT showed negative responses during the first 2 months post-cART [all responses <50 spot-forming cells (SFCs)/106 peripheral blood mononuclear cell (PBMC)], became weakly positive at M4, probably related to partially controlled HIV replication (87 and 153 SFCs/106 PBMC against P24 and Nef, respectively), and then negative again at M8 (Fig. 1A).
In this study we report a case of a primary HIV infection with an unusual extremely severe immune suppression and CD4 T cell lymphopenia occurring in an adult with no pre-existing evidence of immune suppression. The CD4 count was not linked to the result of documented coinfection but could have been linked to the loss of activated cell or due to some predisposing genetic state or condition that might accentuate CD4 loss in acute HIV infection. 1,2,8 In this case, several characteristics were unusual in addition to this major CD4 lymphopenia: first HIV tropism has been determined as non-CCR5 based on V3 loop sequence, which is uncommon during a primary HIV infection but has been reported in 10%–15% of cases. 9 Noteworthy, the virus tropism was probably a CXCR4-tropic HIV, which is known to induce more profound CD4 lymphopenia. 10 Second, a very delayed HIV-specific humoral response detected only at month 8 after cART, 4 third the T cell anergy assessed by the extremely poor memory CD4 T cell response to HIV-p245 and the negativity of the anti-HIV ELISpot assay. 11 The immune reconstitution with cART was also partial though following some classical findings: first, a rapid and strong increase in CD4 and CD8 T cell counts, corresponding to the desequestration from lymph nodes, was, however, followed by a much lower pace of CD4 cell count continuous increase. 12
Those observations can be explained by (1) thymic production of naive cells as shown by the increase of CCR7+CD45RA+CD4+ cells in blood (Fig. 1D), 13 (2) by stopping the conversion of naive CD4 T cells to memory T cell after treatment, and (3) by the decrease of the activation-induced cell death attested by decreased activation markers (HLA-DR, CD25) and apoptosis marker (CD95) on CD4+ cells (Fig. 1D), thanks to the VL negativity. Also, the transient detectability of HIV-specific CD8 T cells that disappeared later on with viral control has already been described before. 14
Regarding the HIV-specific antibody responses, the unexpected negativity of the combined ELISA and WB 2 weeks after cART initiation can potentially be due to the profound immunosuppression. Nevertheless, the delay of the WB positivity does not exclude that the patient was diagnosed during the chronic phase of the HIV infection. Unfortunately, no blood sample was done before the diagnosis. However, the WB analysis showed a typical profile of primary infection with the low positivity of the HIV-1 p24 and p55 bands on WB (incomplete profile), 6,7 which was highly suggestive of acute infection in this particular clinical context. In the literature, negative results of HIV-1 antibody tests for patients who were tested positive for p24 antigenemia and/or HIV-1 nucleic acid amplification have been reported during rapid and severe disease course. 15
Noteworthy, in our patient, the possibility of an underlying common variable immunodeficiency (CVID) was ruled out with normal subsequent gammaglobulin levels, 16 although HIV infection can normalize IgG levels in CVID patients. 17 No genotyping evidence for an underlying primary immunodeficiency was found. Although it is well known that the rapid negativation of the VL with extremely early therapy may result in a major delay in the positivation of the HIV serology, 4 the lack of HIV VL determination between D0 and M5 prevents us to extrapolate data about a rapid virological control or not. However, the patient is still in the standard curve for HIV VL decrease because the initial VL has raised to 5.9 log so the decrease of the VL corresponds to what is expected in terms of delay: the objective is <50 copies/mL at M6 with an exception for the initial VLs >5 log for which the time of attaining undetectability can be longer according to the French guidelines. 18
So far, our hypothesis is that the initial extremely severe depletion in CD4 T cells had severely altered the T helper responses to the HIV-specific CD8 T cells, which might have altered cytotoxicity on HIV-infected cells and delayed undetectability of the HIV VL. Clinicians should be aware that such severe immunosuppression can be observed in the context of primary HIV infection with alteration of the general status but without severe coinfection, and can be associated with a delay in the seroconversion to HIV. This immunosuppression can be only partially corrected with rapid onset of ART.
Footnotes
Acknowledgments
The authors thank Christophe Parizot and the T4/T8 departments for help with flow cytometry.
Author Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was received for this article.