
Abstract
Elderly people living with HIV are increasing. At present in the United States, nearly half of newly diagnosed HIV-infected people are aged >50 years. Diagnosis and treatment of HIV-infected elderly patients tends to be delayed by several health care factors as several life-threatening diseases are common in elderly people. This study aimed to find the pooled HIV prevalence in elderly population and the present situation of continuum care for the elderly HIV patients through systematic review and meta-analysis. All previously published articles from 2000 to 2018 are retrieved using MEDLINE, PUBMED, Cochrane Library, EMBASE, and Google Scholar. DerSimonian and Laird Random Effects model are used to critically appraise articles. STATA 13.0 is used to perform the meta-analysis and quantum-geographic information system (Q-GIS) is used to prepare desired map. I 2 statistics has been used to test heterogeneity and publication biases. Results have been presented using forest plots. A total of 28 studies are included in this meta-analysis. Present analysis revealed pooled prevalence of HIV in elderly population as 15.79% with a lower rate of viral suppression as 11.524% (95% confidence interval, CI: 11.199–11.855), where a moderate number 38.643% (95% CI: 38.289–38.997) of elderly patients received antiretroviral therapy (ART) globally. The ART retention rate was 12.769% (95% CI: 12.540–13.001) with 6.15% (95% CI: 6.089–6.212) mortality. Despite successful administration of ART in developing part of the world that have relatively higher retention rates among HIV-infected elderly patients only a small percentage are virally suppressed, largely due to elderly drugs interact with ART and several comorbidities reduce the life span of the elderly people.
Introduction
Age is an indicator of clinical progression in HIV. In an investigation assessing the anticipation of HIV infection in treatment-naive patients beginning on highly active anti-retroviral therapy (HAART), Egger et al., 1 distinguished age 50 years and more as an independent prognostic factor that influencing clinical progression from HIV to death. A study led by Butt et al. 2 uncovered that people aged 50 years and more diagnosed HIV reactive was related with shorter life span. Thus, in similar investigation on HIV, Babiker et al. 3 confirmed that elderly age at time of seroconversion was related with lower endurance rates among HIV-naive patients, especially in the years before HAART. 3 It was found that general aging impacts on mortality of HIV patient. The average endurance for the individuals who were infected in between 25 and 34 years of age was 11 years, which contrasted with 6.6–4.4 years in the elderly people who were infected at 55–64 years of age and 65 years and more established. 4 It is observed that for each 10-year increment in age at time of HIV disease, the general death rate expanded by 43%. Besides age at disease, the time since infection was categorically associated with expanded mortality in more aged people (ages 45 55 years) who had the most higher mortality rate when contrasted with more youthful people <45 years. 4 Rapid development to AIDS and reduced endurance in elder HIV-infected patients has also been established in French and Spanish cohorts. 5 As life expectancy in Africa and several other developing countries in Asia is lesser than advanced countries around the world, WHO have characterized elderlies as people of 50 years or more. 6 Present definition of older adults for reporting HIV occurrence and antiretroviral therapy (ART) adherence, in low- to middle-income countries, is finely documented in the published articles. 6,7
It is globally estimated that 36.7 million people are living with HIV. 1 According to UNAIDS, there are 5.8 million people aged 50 years and older are living with HIV, which represents 17% of all adults aged 15 years and over are living with HIV. 2 In the United States, nearly half of freshly diagnosed HIV-infected people are existing with age >50 years (Fig. 1). According to an estimation of UNAIDS along with WHO, 40 million people are living with HIV/AIDS in the world, of them 2.8 million are 50 years and more. As per Public Health Agency of Canada, 8% of HIV cases (12% of these are women) and 12% of AIDS patients were 50 years or older in Canada. 8 Similarly, in United Kingdom, 3.8%–8.5% of HIV cases have been diagnosed in adult women and men at the age of 50 years or elder, respectively. 9
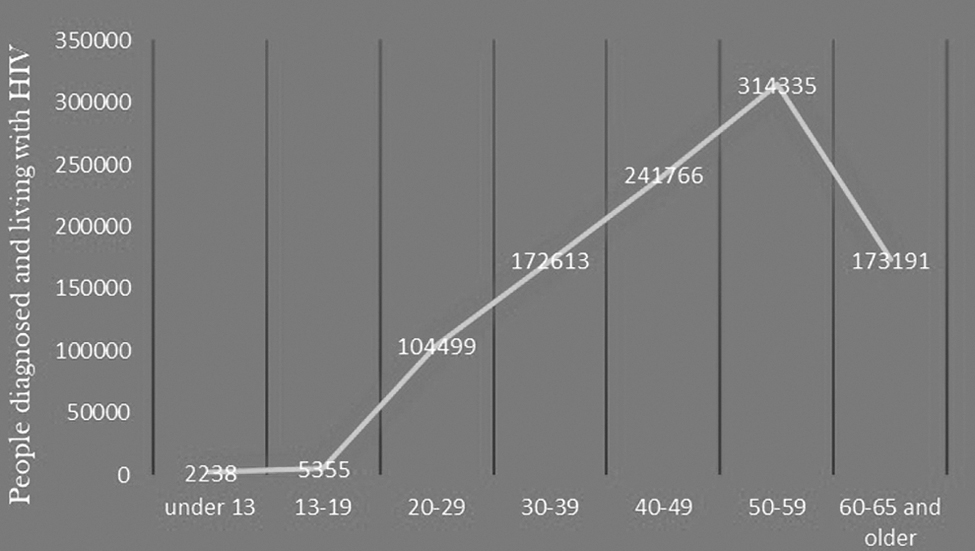
People diagnosed and living with HIV in the United States and dependent areas of them 48% aged ≥50 years, (after CDC: Diagnosis of HIV infection in the United States and dependent areas, 2017: HIV surveillance report, 2018). CDC, Centers for Disease Control and Prevention.
During past decade there has been a rise in the admittance to life-prolonging ART, and factors such as enhanced HIV surveillance, clinician consciousness of HIV infection, development of diagnostic, collectively have led to a rise in people aged 50 years and older presently living with HIV. 4,10
With the increased life span, aging people become susceptible to several pathogens to numerous diseases, 11,12 which in turn may affect their adherence to ART. Evidence shows that deprived immunological response to ART is a substitute of biological aging. 13,14 The normal aging process decline in immunocompetence and making elderly people susceptible to both infectious and noninfectious diseases such as diabetes, cardiovascular diseases, and hypertension. Therefore, sympathetic adherence to ART is essential to develop strong HIV treatment program for the elderly people. Optimal adherence has the benefit for individual to public health benefits in prevention of HIV endemic. 15 –17 However, lower adherence of ART leads to inadequate viral suppression letting advancement of disease, which eventually increases mortality among elderly people. Through a report available in public domain Centers for Disease Control and Prevention (CDC) shows the predictable number of deaths among persons with HIV increased in people aged ≥45 years, with a 28% increase in elderly people of 50 years and more and sharp 18% increase in persons 60 years and older. 17,18
Several older HIV-infected people remain sexually active and make themselves continue to involve in unprotected sexual intercourse far into advanced age. 19,20 In higher level of society several widowed and divorced people are engage in dating, and they are reluctant to use condoms for difficult maintaining issues. Also, elderly women, who are no longer concerning about being pregnant, are less likely to insist their partners to exercise safe sex, increasing the risk of HIV transmission. 16,19
During 2014, UNAIDS announced its 90-90-90 program with the aim to culminate global AIDS epidemic through improved surveillance, ART adherence, and viral suppression among infected people. 10,21,22 Motto of this program is to accomplish its goals by 2020, and one of the targets is to have 90% of all infected persons aware of their HIV status and simultaneously 90% people receive antiretroviral treatment (ART) to achieve 90% viral suppression by 2020. This target could be achieved through strong emphasis on ART. Despite growing recognition that older people are increasingly infected with HIV 6,10,23 and are accessing treatment. 10,24,25 There are reasons to believe this in the context of developed part of the world, where elderly people are likely to be financially stable and medically aware of their health. However, developing countries might involve in different blockades such as higher rates of poverty, inadequate resources for care and support 26,27 ; multimorbidity along with several chronic diseases collectively leads to polypharmacy, 10,28 social isolation, 10,29,30 ageism, or elder abuse. 10,31,32 To gain insight of the status of HIV care among elderly people, this study of the systematic review and meta-analysis has been initiated using available previously published evidence.
Methods
Design of the study, including policy of exploration
This study is a systematic review and meta-analysis of previously published articles on HIV care among elderly population. Guideline on Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) is followed for the present meta-analysis (Supplementary Data). 33 All published articles are retrieved using appropriate search terms in Google Scholar, MEDLINE, PUBMED, EMBASE, and Cochrane Library. This review article included all published articles from January 2000 to December 2018. For the exploration used terms are HIV infections in elderly or elderly population or elderly medicine or adolescent or adolescence or people >50 years of age or older people or older men or older women and HIV care or HIV continuum of care or retention or follow-up and viral suppression and ART or antiretroviral therapy.
Study choice and acceptance criteria
Acceptance criteria have been defined according to the population, interventions, and comparisons, including outcomes as well as study design (PICOS) arrangement. Present review comprised entire articles, which included experiments directed to measure the pooled prevalence of HIV infection among the elderly people and available care toward it. All available articles comprised not confining to a definite study policy. All the references selected from previous studies have been screened to retrieve additional articles that could be included in this study. Full text article only in English (U.K. or U.S.) are included.
Quality evaluation and data accumulation
Evaluation of articles has been performed using their title, abstract, and a full review of the text written before including it in the ultimate meta-analysis. Calculation of pooled prevalence is done with corresponding 95% confidence intervals (CIs), for retention in the care of elderly patients as well as viral suppression among them the DerSimonian and Laird Random Effects (REs) model has been used, with double arcsine transformation to stabilize the variance. 34 The standard instruments included are randomly selected study articles, clear explanation of the standards for the inclusion of the article to this study identification and addressing of confusing factors, use of objective criteria to assess the outcome of interest, and consistent measurement of outcome variable along with the suitable statistical application. 34 A critical judgment has been conducted before the data accumulation.
Data abstraction
Data mining has been performed with the help of Joanna Briggs Institute's (JBI) critical appraisal tool for the study of pooled prevalence. 35 All the essential information is mined from the finally chosen articles using the data mining option, which includes information on author name and year of publication, study area, study design, study period, sample size, pooled prevalence of HIV in the elderly population, period of retention or follow-up, viral suppression, chances of noninfectious comorbidities (cardiovascular disease, bone disease, renal failure, etc.) among elderly HIV patients on ART.
Noteworthy observations
One of the objects of this article is to find out the collective occurrence of HIV among the elderly people from different clusters of the world. For the present meta-analysis “elderly population” is taken as the “parent population” and factor “HIV positive” is treated here as the “disease.” With the administration of ART, nowadays HIV infection has become a controllable chronic disease, and many infected patients are now living into their 60s and beyond. In addition to this, many patients with newly diagnosed HIV infection are >50 years. Subsequent rising frequency of HIV infection in older adults presents several challenges for the minimum primary health care facilitators. This article depicts a scenario of increased HIV infection among elderly people and highlights the present situation of continuum care for the elderly people along with various comorbidities inherent in the aging HIV patients.
Prejudice of publications along with heterogeneity
Heterogeneity of the studies is evaluated by I 2 test and its equivalent p value. If the p values go <0.05 the situation assumed as heterogeneity. I 2 test of 25%, 50%, and 75% has been, respectively, assumed as low, moderate, and high heterogeneity. 36 Egger's test as well as Begg and Mazumdar's test are used to calculate publication bias, and a p value <0.05 are used to state its statistical significance. 37,38 Using the RE analysis the Duval and Tweedie nonparametric trim and fill analysis has been performed for meta-analysis, which showed the presence of nonsignificant publication bias (Egger test, p > .05). 39
Statistical approaches toward data analysis
Accumulated data are put into Microsoft Excel (MS-Office 2016) and then transferred to STATA 13 (for Windows) for meta-analysis. 40 Pooled prevalence of HIV in the elderly people with 95% CI has been represented through forest plots. Pooled prevalence with 95% CI has been accessible through forest plot, which displays the factors associated with HIV in the elderly population. Subgroup analysis has been conducted for the study region included region of study [North America, Europe, Africa, and Asia] and type of the study (prospective cohort, retrospective cohort, and cross-sectional studies). A weighted inverse variance REs model used to conduct the meta-analysis and evaluate the overall pooled prevalence from the included studies. 36
Preparation of map
Topographical sheets of world map have scanned, geo-referenced, and then digitized with the help of quantum-geographic information system (Q-GIS), a free, open-sourced, cross-platform desktop based GIS application, written in C++, Python, QT languages and provides services like viewing, editing, analysis of geospatial data. Data based on region has been entered to the newly prepared digitized map as the nonspatial data or attributes. 41,42
Results
Study selection
The entire 122 articles are retrieved through electronic database searching. Articles are screened using their titles, abstracts, and through full article review. Therefore, overall 94 articles are omitted after their title and abstract review. Twenty-eight articles are assessed for eligibility. Twenty-eight articles finally comprised this study (Fig. 2).
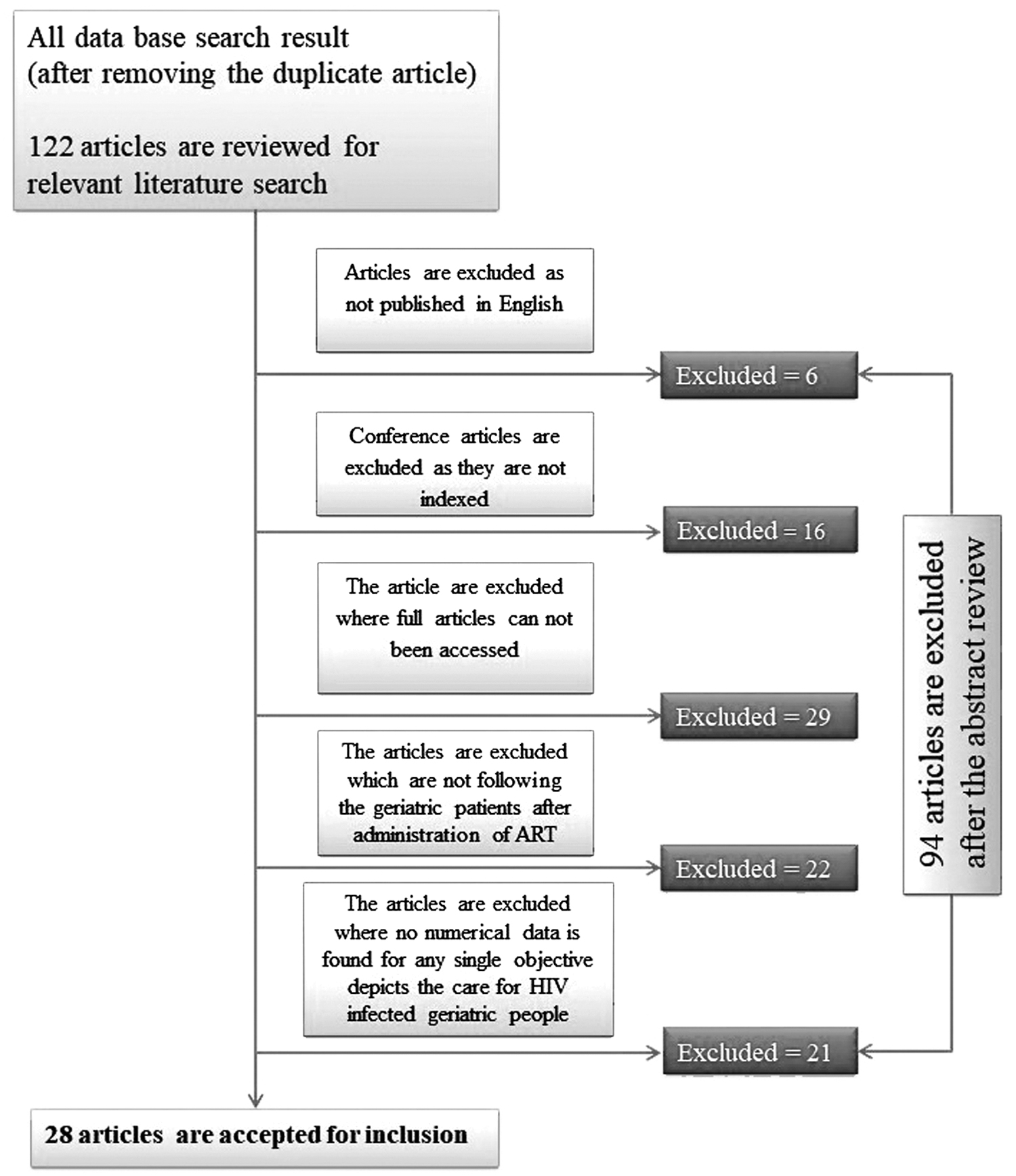
Flow diagram of search and selection procedures for systematic review.
Publication bias
After checking funnel plot and the significance of Egger's regression test, no studies have been excluded from pooled prevalence estimation. Nonsignificant publication bias with an Egger's regression p value >0.05 has been observed during this study (Fig. 3).
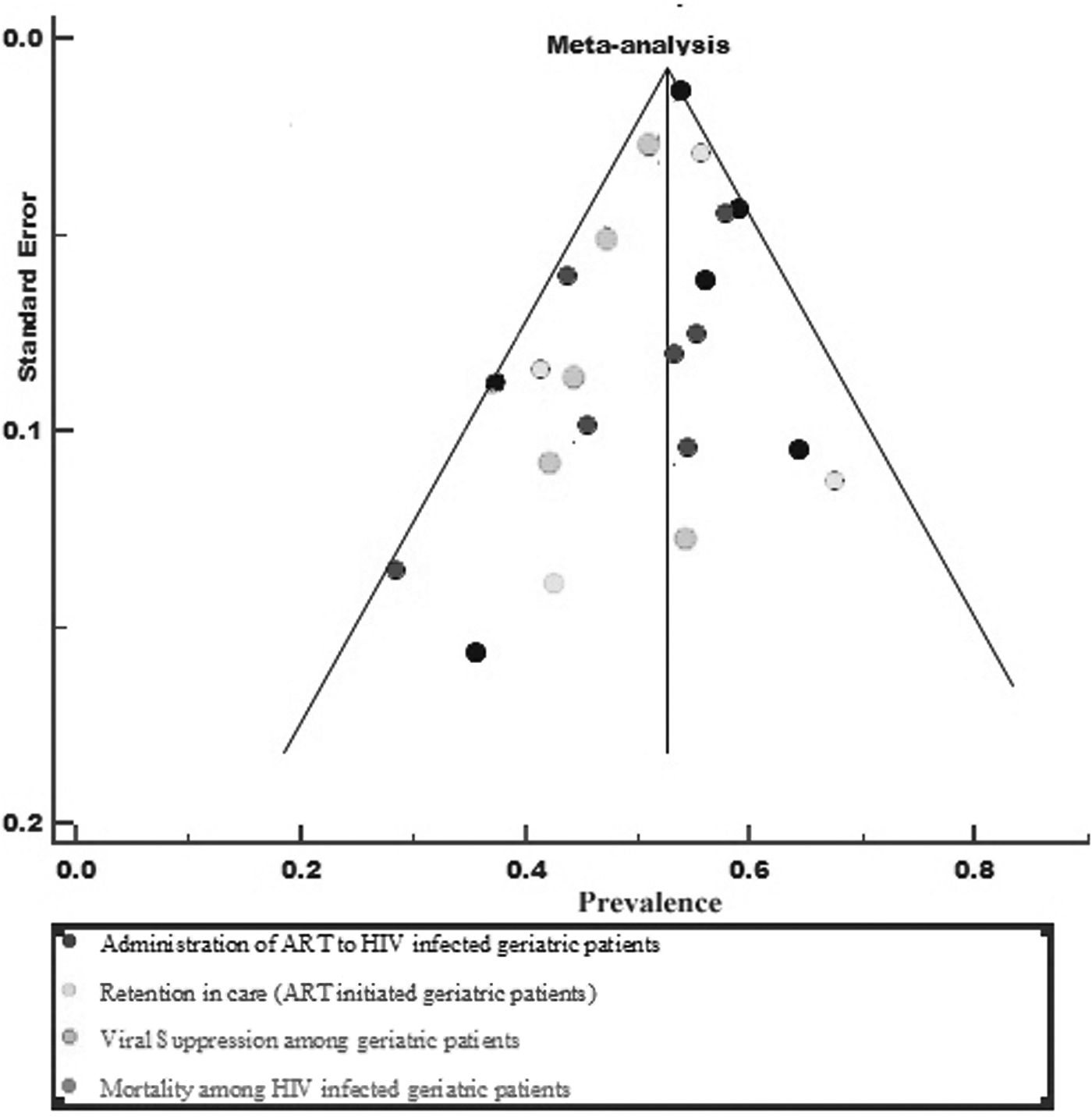
Funnel plot to find out publication bias.
Features of included studies
Sixteen of the studies included in the ultimate analysis have been retrospective cohort studies, 43 –58 five studies are prospective cohort studies, 59 –63 and a single cross-sectional study. 64 The studies used health care-based data on elderly people who are infected with HIV, which has been collected from 2002 to 2018, although there is no published article found before 2002, which could qualify the inclusion criteria for this study. All studies included the care for HIV-infected elderly people in various health institutions. Overall, a total of 1,149,767 elderly people with HIV infection are incorporated in this article (Table 1).
Summary Characteristics of Studies Included in the Meta-Analysis of the Pooled Prevalence of HIV Among Elderly Population Around the World
Quality of included articles
Quality of included studies have been determined and depicted separately (Fig. 4). It would be noted that quality of any individual study, which are calculated and presented here is exclusively to fulfill the demands of aims and objectives of this study. Authors are not intended to comment on overall quality of any article included in this study.
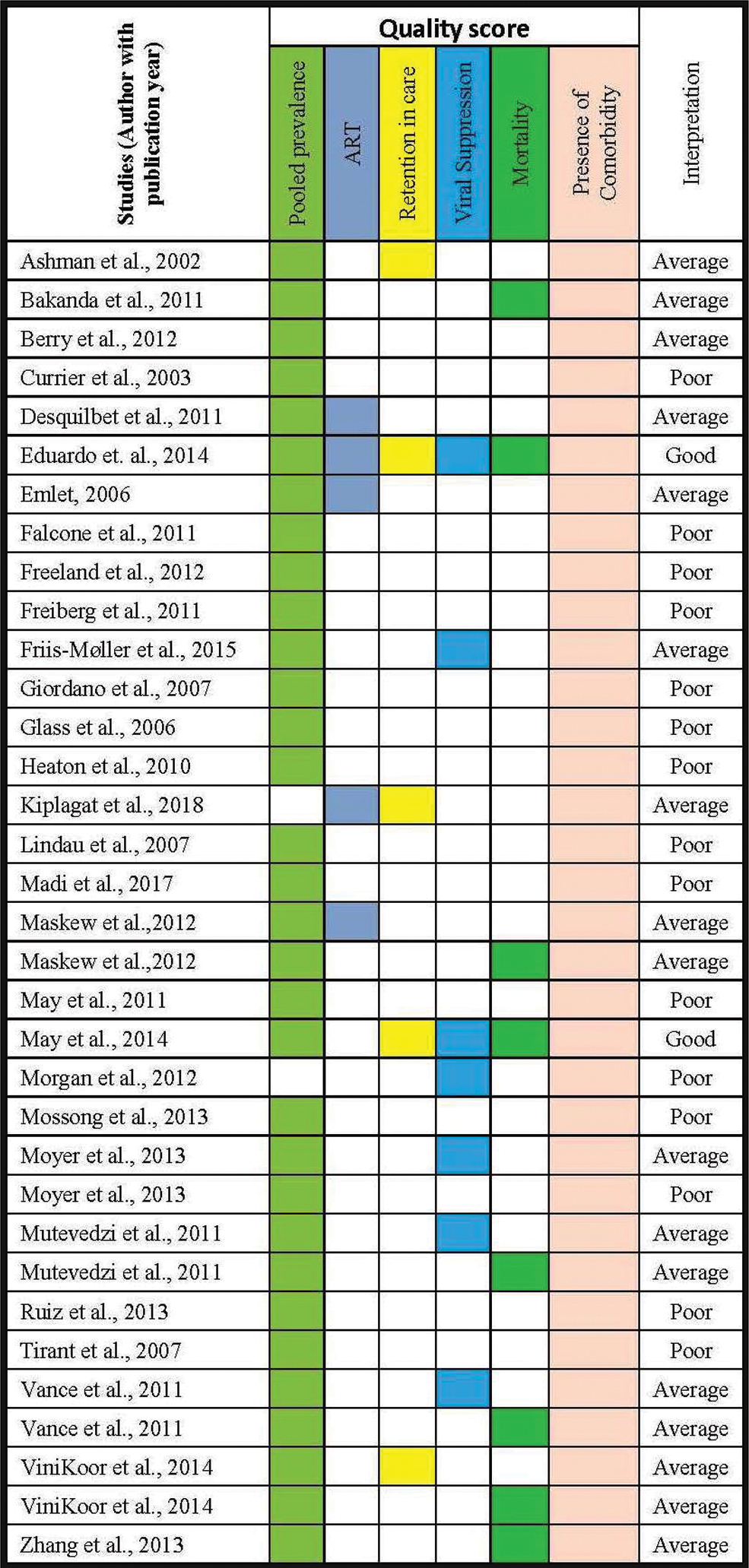
Quality of included studies. (It would be noted that quality of any individual study, which are calculated and presented here is exclusively to fulfill the demands of aims and objectives of this article. Authors are not intended to comment on general quality of any article). Color images are available online.
Pooled prevalence of HIV infection among elderly people
Pooled prevalence of HIV infection among elderly people in the studies comprises from as low as of 1.67% (95% CI: 0.727–3.278) revealed by Moyer 54 in the United States and as high as 59.82% (95% CI: 56.31–63.265) revealed through Desquilbet et al., 59 in multicenter sites located in Baltimore, Chicago, Los Angeles, and Pittsburgh. Moreover, the pooled prevalence of HIV infection among elderly people across the world has been found 15.7%. Similar result was obtained from regional subgroup study also.
Subgroup analysis for HIV infection among elderly people
Subgroup analysis has been conducted by different study characteristics are depicted as follows.
Subgroup analysis (based on study period)
Detailed analysis on the study period has been done separately given full 100% weightage to the pooled prevalence of HIV infection among elderly people around the globe on the basis of study period. Here pooled prevalence for the studies performed before 2010 are found 15.059% (95% CI: 5.064–29.128) and I 2 = 99.90% (95% CI: 99.89–99.91), p < .0001, Q = 601.79 (Fig. 5) and for studies performed after the year 2010 in across earth are found 13.033% (95% CI: 7.780–19.395) and I 2 = 99.57% (95% CI: 99.51–99.62), p < .0001, Q = 369.8 (Fig. 6).
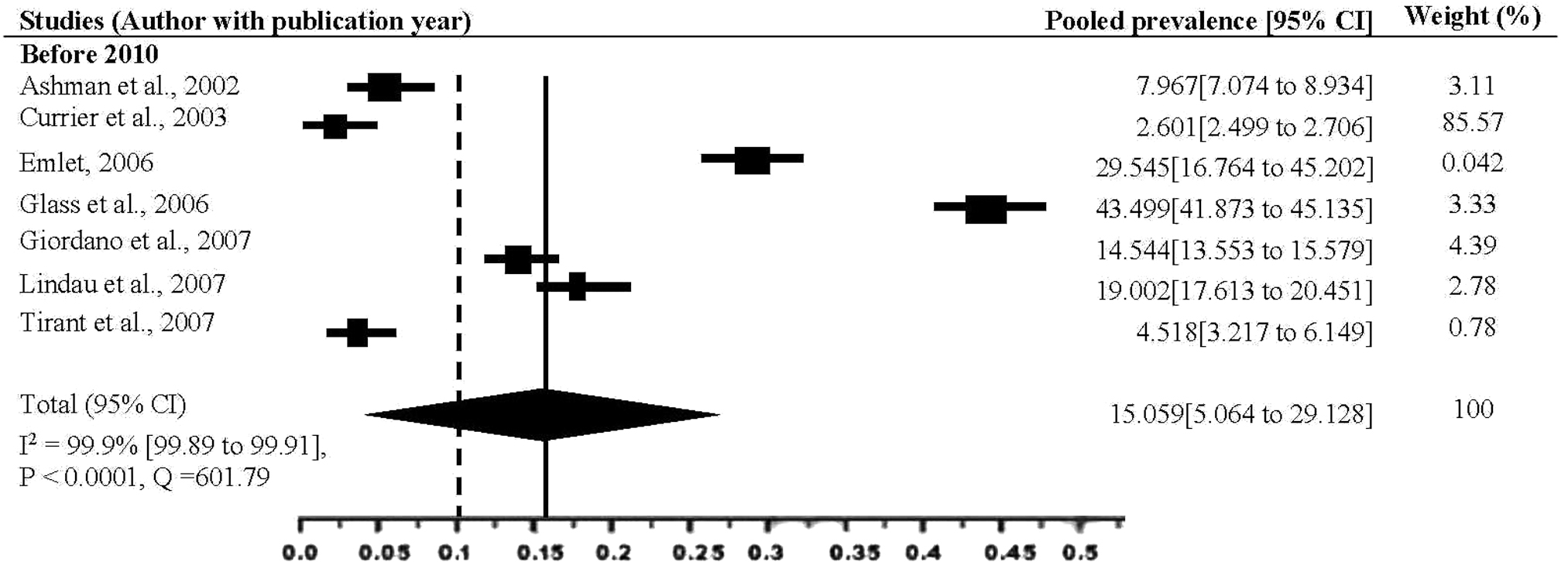
Subgroup analyses (meta-analysis of the year before 2010) for the pooled prevalence of HIV among elderly population. The midpoint and the length of each segment indicated pooled prevalence and a 95% CI, whereas the diamond shape showed the combined pooled prevalence. CI, confidence interval.

Subgroup analyses (meta-analysis of the year from 2010) for the pooled prevalence of HIV among elderly population. The midpoint and the length of each segment indicated pooled prevalence and a 95% CI, whereas the diamond shape showed the combined pooled prevalence.
Subgroup analysis (based on type of study)
Detailed analysis on type of study has been done separately given full 100% weightage to the pooled prevalence of HIV infection among elderly people on the earth on the basis of type of study. Here, five studies are included as prospective studies. Pooled prevalence for prospective studies is observed 10.969% (95% CI: 10.665–11.279) and I 2 = 99.89% (95% CI: 99.88–99.91), p < .0001, Q = 377.94 and for the retrospective studies pooled prevalence is found 9.992% (95% CI: 5.587–15.497) and I 2 = 99.78% (95% CI: 99.68–99.81), p < .0001, Q = 672.8. However, there is a single study found as cross-sectional study for pooled prevalence analysis (Fig. 7).

Pooled prevalence with corresponding 95% CIs of the subgroup analysis based on the study type (cohort or cross-sectional).
Subgroup analysis (based on region)
Detailed analysis on type of study has been done separately given full 100% weightage to the pooled prevalence of HIV infection among elderly people on the earth on the basis of type of study.
Fourteen studies are added from United States or from North America. Pooled prevalence for studies from United States is observed as 4.257% (95% CI: 4.139–4.377) and I 2 = 99.67% (95% CI: 99.62–99.71), p < .0001, Q = 366.0. Four studies are added from Europe, one from Switzerland and other three from the United Kingdom. Pooled prevalence for studies from Europe is observed as 36.723% (95% CI: 35.754–37.7) and I 2 = 99.38% (95% CI: 99.12–99.56), p < .0001, Q = 282.0. Five studies are included from Africa. Pooled prevalence for studies from Africa is observed as 10.599% (95% CI: 10.117–11.096) and I 2 = 98.67% (95% CI: 98.50–99.33), p < .0001, Q = 30.0. Moreover, two articles are included from Asia especially those articles are each from India and China. Pooled prevalence for studies from Asia is observed as 18.462% (95% CI: 16.619–20.419) and I 2 = 90.25% (95% CI: 64.47–97.32), p = .0014, Q = 10. Overall, pooled prevalence for elderly population of the world (from the article included) is 15.791% (95% CI: 4.308–32.653) and I 2 = 99.96% (95% CI: 99.95–99.97), p < .0001, Q = 75.0 (Fig. 8).

Pooled prevalence with corresponding 95% CIs of the subgroup analysis based on the regional clustering. The midpoint and the length of each segment indicated pooled prevalence and a 95% CI, whereas the diamond shape showed the combined pooled prevalence.
Moreover, the area included in this study is added on a map (world map) with the help of Q-GIS (Fig. 9).

Geographical map of world showing HIV-infected elderly population (for this study purpose). Color images are available online.
Administration of ART to HIV-infected elderly patients
Five studies, 101,162 elderly people, are included in this category of meta-analysis. 46,50,51,59,64 Except for a single study, 51 all other four included studies revealed that the administration of ART to the HIV-infected elderly patients for treatment and care has been successfully implemented across the world. The present meta-analysis showed a strong administration of ART among HIV-infected elderly patients, 38.643% (95% CI: 38.289–38.997). The statistically significant heterogeneity has been observed; I 2 = 99.75% (95% CI: 99.68–99.81), p < .0001, Q = 314 (Fig. 10). The Begg and Mazumdar's test as well as Egger's test for publication bias also showed no statistical evidence of publication bias (p < .001).
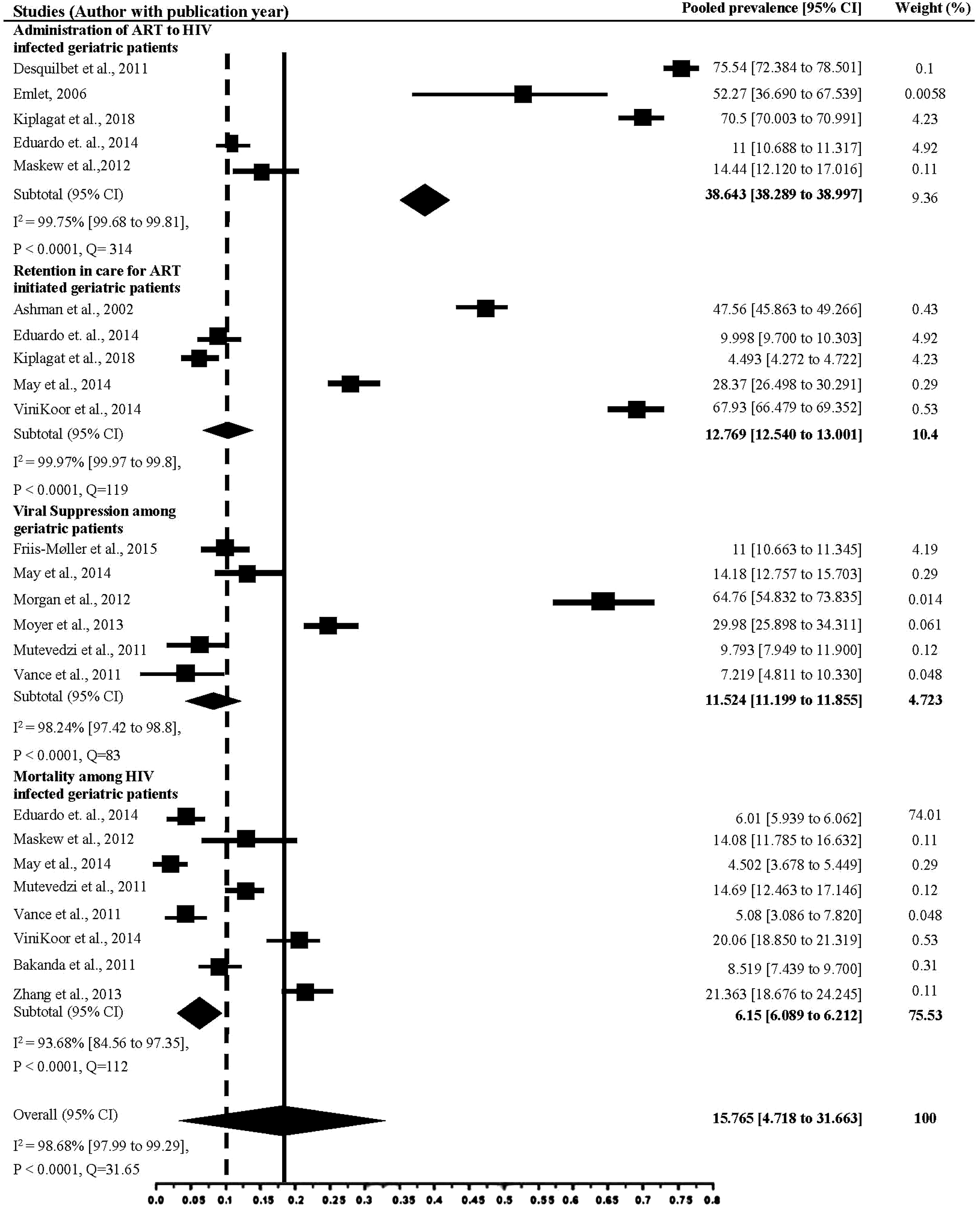
Forest plot of the pooled prevalence with corresponding 95% CIs of the study. The midpoint and the length of each segment indicated pooled prevalence and a 95% CI, whereas the diamond shape showed the combined pooled prevalence showing administration of ART to HIV-infected elderly patients, Retention in care (ART initiated elderly patients), Viral suppression among elderly patients having HIV and mortality among HIV-infected elderly patients. ART, antiretroviral therapy.
Retention in care (ART initiated elderly patients)
A total of five studies, 91,353 elderly people, are included in this category of meta-analysis. 43,50,52,58,64 Two studies clearly showed nonsignificant association between retention and HIV-infected elderly patient care. 50,52 The rest of the included articles in this category of the meta-analysis shows significant association. Consequently, the pooled meta-analysis showed that elderly patients who are not participating in the retention of care program are more likely to carry the burden of infection than their counterparts, 12.769% (95% CI: 12.540–13.001). However, statistically significant heterogeneity has been observed, I 2 = 99.97% (95% CI: 99.97–99.8), p < .0001, Q = 119 (Fig. 10). The Begg and Mazumdar's test and Egger's test for publication bias showed no statistical evidence of publication bias (p < .00001).
Viral suppression among elderly patients
Six studies, 40,995 elderly people, are included in this category of meta-analysis. 53,54,55,57,61,66 Two of the incorporated studies 61,66 showed significant association between viral suppression and elderly patient care. Rest clearly showed nonsignificant association between retention and HIV-infected elderly patient care. The analysis shows viral suppression among elderly people is 11.524% (95% CI: 11.199–11.855). Statistically significant heterogeneity has been observed, I 2 = 98.24% (95% CI: 97.42–98.8), p < .0001, Q = 83 (Fig. 10). Whereas, the Begg and Mazumdar's test and Egger's tests showed no statistical confirmation of publication bias (p = .003).
Mortality among HIV-infected elderly patients
Eight studies, 624,782 elderly people, are included in this category of meta-analysis. 51,53,55,57,58,64,67,68 Five of the included studies 55,58,64,67,68 showed a significant rate of mortality among the elderly people having HIV. Remaining studies showed no such relation. The pooled meta-analysis showed mortality rate among elderly people having HIV is 6.15% (95% CI: 6.089–6.212). Statistically significant heterogeneity has been observed, I 2 = 93.68% (95% CI: 84.56–97.35), p < .0001, Q = 112 (Fig. 10), whereas the Begg and Mazumdar's test as well as Egger's tests showed no statistical confirmation of publication bias (p < .005).
Moreover, overall pooled prevalence for elderly population of the world (from the article included) is 15.765% (95% CI: 4.718–31.663) and I 2 = 98.68% (95% CI: 97.99–99.29), p < .0001, Q = 31.65 (Fig. 10).
Discussion
HIV-infected people who are engaged in care are going through four chief blockades to effective dealing with antiretroviral medications: postponement, interruption or failure to initiate the therapy, deficiency of persistence with therapy, and poor adherence and viral resistance to ART medicines. Present analysis shows a moderate number of elderly patients infected with HIV are opted for ART and successfully adhere to it. Several elderly people having HIV can expect to live as normal people, but those who diagnosed late and started late ART may have a lower life expectancy. 17
Successful treatment of HIV needs sustained engagement in HIV care. 17,44 –46 Opportunistic diseases such as pneumocystis (pneumonia) are most common in individuals with unknown HIV serostatus and in those people who are presently not receiving HIV treatment or care. 17,54 Present findings also reveal that the number of elderly people who are opted for ART and successfully adhere to ART but lost in follow-up due course of time. Multiple cohort studies in different countries have found that large numbers of HIV-infected individuals are completely lost to follow-up, 17,59,64 in some cases these people eventually re-establish care. Four studies in Europe found that out of care HIV-infected individuals return to care in 1–2 years. 59,66 Effectively treated patients who attained viral suppression during initial year of ART have a normal life expectancy; a HIV-positive person with age of 35 years is estimated to live up to 80 years on an average. 67,68 Present finding also shows a moderate rate of viral suppression among the elderly people, but for an elderly person increment of life expectancy is still a matter of challenge even in developed parts of the world. 17,69,70
As many patients were lost during follow-up, there remains the possibility of undocumented deaths, which may bias in estimations of predictable age at death upward. Present finding also shows a good number of elderly people are lost due to death, who are enrolled in ART program. 17,71
However, many HIV patients living longer due to successful administration of ART are now suffering in treatment-related problems. This has directed them to increased prospect of polypharmacy, defined as the use of four or more medications. Overall, polypharmacy in the elderly people is associated with adversative drug actions and interactions, unsuitable medicine, restlessness, falls, fractures, and poor medication adherence. 60,72 But this develops additional problem in HIV-infected elderly patients, as numerous drug interactions can modify the effectiveness of the antiretroviral treatment and could consequence in drug toxicity.
Death rate in HIV-infected elderly patients during ART have been from noninfectious comorbidities, which might be cardiovascular disease, bone disease, renal failure, and so on, which coexist and are associated as well as advanced with age. 57,68,73 However, elderly age and each added year on ART might lead to a situation called of polypathology (simultaneous occurrence of two or more defined diseases). 57,74
The pooled prevalence of diabetes mellitus is 3% in HIV-infected people who have never opted for ART, but glucose intolerance increases to lower to much higher range in those who have opted for it. 75,76 Glucose disorders are associated with HIV-associated factors such as lipodystrophy and ART, mostly the long-term practice of protease inhibitors. 65 Several antiretroviral treatments have been connected with substantial bone loss and osteoporosis, which comprises with tenofovir-based as well as protease inhibitor-based treatments. 58,77,78 Most studies have shown that bone mineral density decreases during the first 2 years of ART in such regime. 17,59,68
HIV-related neurocognitive syndromes are common with an estimated half of HIV-infected patients experience some degree of cognitive loss and some developing dementia. 50,79,80,81 HIV-related dementia is frequently subcortical, with changing symptoms such as psychomotor retardation to difficulty multitasking and in some case apathy. 82,83 A frailty-associated phenomenon of severe weight loss, exhaustion, snowlines, and low physical activity is more frequent in HIV-infected elderly people than in noninfected elderly people. 66,84,85 HIV-infected elderly men are more than age-matched controls to be frail, and the possibility of frailty increases through age and duration of HIV infection. 64,86,87 People having HIV are going through a higher risk of cancer, specifically, compared with the normal population. However, the elderly people infected with HIV are suffering through non-HIV-related cancers, such as malignant tumor formation in kidney, lung, anus, liver, head or neck, and skin and Hodgkin lymphoma 64,87,88
Limitations of the Study
The present systematic review following the PRISMA guideline included only qualified articles on HIV care among elderly population and excluded unpublished research studies and several reports by governmental and nongovernmental agencies, articles published in locally available journals that are not indexed in most databases. The countries of sub-Saharan Africa, Southeast Asia, which represent most of the HIV-affected people in the world, are not allowed to publish their result (due to several geo-political issues), little often publish their results, or only publish in locally available journals. Several conference articles and abstracts that are not indexed are not included in this study. This review included only a few variables associated with HIV care among elderly population, because of the limited number of published studies. Only those articles published in English (U.K. or U.S.) are included in this study, and these altogether may have led to potential reporting bias.
Conclusions
People with HIV living longer may be an outcome of newer effective combination of antiretroviral treatments; physicians face innovative challenges to deal with sudden rising situation for elderly patients with HIV. It is necessary to improve the understanding of drug–drug interactions and polypharmacy problems, which are outcomes of complex medication treatments, enhanced risk of adverse drug actions, and cost of high medication and be able to discourse the complex psychosocial materials among these growing HIV-infected elderly population. As a combined outcome of currently mentioned issues, when an individual with HIV on active ART grows older, the burden of comorbid medical disease, which includes cardiovascular disease, diabetes mellitus, osteoporosis, dementia, and various types of cancer (unrelated to HIV) will continue to increase.
Ethics Approval and Consent to Participate
Not applicable as published data were analyzed for this study.
Availability of Data and Material
All data generated or analyzed are included in this article.
Footnotes
Acknowledgment
The authors thank the staff of Virology Division, ICMR-National Institute of Cholera and Enteric Diseases, Kolkata, India, for help and support.
Authors' Contributions
M.B. and M.K.S. conceived and designed the study. M.B., S.D., and S.N. established the search strategy. M.K.S. and S.D. contributed software/analysis tools. M.B. and S.N. extracted the data. M.B. performs the analysis. M.B., S.D., M.K.S., S.N., and N.D. wrote the article. All the authors read the article before they have given the final approval for publication.
Author Disclosure Statement
No competing financial interests exist.
Funding Information
The study was funded from internal resources.
Supplementary Material
Supplementary Data
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.