
Abstract
Gait speed declines at a faster rate in persons with HIV (PWH) than in the general population but the risk factors associated with this decline are not well understood. In the AIDS Clinical Trials Group (ACTG) A5322 (HAILO, HIV Infection, Aging, and Immune Function Long-term Observational Study), an observational cohort study of PWH ≥40 years of age, those who developed slow gait during the first 3 years of follow-up were compared with persons who maintained normal speed. Associations with demographic and clinical covariates were assessed using multivariable logistic regression. Of 929 participants, 81% were men, 31% Black, and 20% Hispanic. Median age was 51 years [interquartile range (IQR) = 46–56]. At study entry, 92% had plasma HIV RNA <50 copies/mL with median CD4 count 631 cells/mm3 (IQR = 458–840). At study entry, 7% of participants had slow gait, 16% had neurocognitive impairment (NCI), and 12% had diabetes. Over 3 years, 87% maintained normal gait speed, 3% maintained a slow gait, 6% developed a slow gait, and 4% improved from slow to normal gait speed. In multivariable models, hemoglobin A1C (HbA1C) percentage, per one unit increase [odds ratio (OR) = 1.36; 95% confidence interval (CI) = 1.03–1.81; p = .033], NCI (OR = 3.47; 95% CI = 1.57–7.69 p = .002), and black versus white race (OR = 2.45; 95% CI = 1.08–5.59; p = .032) at entry were significantly associated with development of slow gait compared with those maintaining normal gait speed. The association between baseline HbA1C and development of slow gait speed highlights an intervenable target to prevent progression of physical function limitations.
Introduction
Although routine use of virally suppressive combination antiretroviral therapy (ART) has dramatically extended the life expectancy of persons with HIV (PWH), this population now experiences both earlier onset and higher rates of chronic noninfectious aging-related comorbidities than the general population. 1 –3 Compared with seronegative controls, PWH exhibit an accelerated decline in physical function and higher than expected rates of frailty. 4 –6 Such declines in functional status have been associated with poor health outcomes such as disability, falls, and reduced quality of life in this population. 7 –10
Slow gait speed is a simple, easily obtainable measure in the clinical setting that requires minimal equipment, training, and time. 11 Slow gait speed is highly predictive of disability and mortality in older adults, 12 –14 and we have similarly found that slow gait speed is associated with subsequent poor outcomes including disability, falls, and mortality in middle-aged PWH. 15 Schrack et al. previously observed that gait speed declines more rapidly with increasing age in men with HIV compared with demographically similar men without HIV. 5 Proposed mechanisms for this accelerated decline in gait speed among PWH include those observed with general aging, such as changes in energy utilization and body composition, decreased aerobic capacity, and worsened biomechanics 16 –19 and characteristics specific to HIV infection, including exposure to ART, prolonged immune suppression, chronic inflammation and immune activation, and mitochondrial dysfunction. 20 –23 Multiple studies among PWH have found associations between decreased gait speed and increasing age, socioeconomic factors (such as nonwhite race, less education, public insurance, and social support), obesity, lower physical activity, tobacco or intravenous drug use, certain mitochondrial DNA haplogroups, and medical comorbidities [particularly renal disease, peripheral neuropathy, neurocognitive impairment (NCI), and diabetes]. 21,24 –30 However, many of these studies have been limited to cross-sectional analyses.
The goal of this investigation was to identify baseline characteristics associated with development of slow gait speed among participants currently enrolled in AIDS Clinical Trial Group (ACTG) A5322/HAILO (HIV Infection, Aging, and Immune Function Long-term Observational Study). This cohort of both men and women has well-defined ART exposure and detailed history of immune and clinical health. Through investigation of this diverse and well-characterized cohort, we aim to better understand risk factors for slow gait to guide strategies to screen for and prevent functional impairment among persons aging with HIV.
Methods
Study population
We performed a longitudinal analysis of participants in ACTG A5322/HAILO, an ongoing observational cohort study of older men and women with HIV who initiated ART through an ACTG clinical trial and were previously followed in the observational study ACTG A5001. Between November 2013 and July 2014, a subset of A5001 participants (n = 1,035) ≥40 years old were enrolled in HAILO for continued long-term follow-up. All participants underwent semiannual visits including fasting laboratory tests and annual evaluations of frailty and neurocognitive function. HAILO participants who had more than one gait speed measurement through the first 3 years of follow-up were included in this analysis.
Outcome
Gait speed was measured as part of the Fried frailty assessment. Slow gait was defined by the average of two readings on a 4-m walk: men ≤173 cm and women ≤159 cm in height who required ≥6.22 s or men >173 cm and women >159 cm who required ≥5.33 s to complete the walk met the criteria for slow gait. 31
Covariates
Baseline covariates included age, nadir CD4+ T lymphocyte count (CD4), history of AIDS-defining illness, CD4, HIV-1 RNA viral load, alcohol use (none, light, moderate, or heavy drinking), body mass index (BMI), waist circumference (elevated if >102 cm in men, >88 cm in women), 32 physical activity (≥3 days moderate/vigorous activity in the last week vs. <3 days), peripheral neuropathy, cigarette use (never, former, and current), substance use within the past month, and use of antidepressant/anxiolytic medication. The presence of any comorbidity was considered as a single covariate. Comorbidities assessed included cardiovascular disease (myocardial infarction, stroke, and coronary artery disease), liver disease, kidney disease, malignancy (within the past 5 years), diabetes [diagnosis or hemoglobin A1C (HbA1C) ≥6.5%], hypertension (diagnosis or use of antihypertensive medications), and hepatitis C (positive HCV antibody or diagnosis). NCI was assessed using the A5001 NeuroScreen that includes Trailmaking tests A and B and the Wechsler Adult Intelligence Scale-Revised Digit Symbol tests. 33 The NeuroScreen was previously validated by comparison with a comprehensive neuropsychological battery. 34 NCI was defined by at least one z-score that was at least 2 standard deviations (SDs) below the mean or multiple z-scores that were at least 1 SD below the mean on separate tests within the A5001 NeuroScreen. Antiretroviral exposures examined were integrase strand transfer inhibitors, tenofovir disoproxil (TDF), efavirenz, and protease inhibitors at initial randomization and at HAILO entry as well as any previous exposure to didanosine (DDI), stavudine (D4T), or zidovudine (AZT).
Statistical analysis
Participants were categorized into four groups based on their gait speed over time: persistently normal, persistently slow, development of slow gait, or resolution of slow gait. Participants who developed slow gait were compared with those who maintained normal gait speed, and those who had resolution of slow gait with those who had persistently slow gait, by demographic, clinical, and behavioral characteristics. Chi-square tests were used for categorical variables and the Kruskal–Wallis test for continuous variables.
Logistic regression models were fit to assess associations between baseline covariates and development of slow gait (vs. being stable normal) and, separately, a return to normal speed (vs. being stable slow). Age was forced into all models, as it is strongly associated with gait speed. Each of the covariates defined above were included separately in the age-adjusted models, and those that were significantly associated with the outcome (p < .1) were included in the final, multivariable models. A two-sided 5% significance level was used for all analyses.
We also fit a series of age-adjusted models stratified by diabetes status to determine if effects of HbA1C were independent of diabetes status, and by sex and race/ethnicity, to determine if sex differences primarily explained by differences in race/ethnicity. Covariates were added to each model as described previously.
Results
Of 929 participants included in this analysis, the median age at baseline was 51 years [interquartile range (IQR) = 46–56]. Eighty-one percent were men, 31% black, and 20% Hispanic. Most individuals had well-controlled HIV infection at study entry: 92% had undetectable plasma HIV-1 RNA (viral load <50 copies/mL) with median CD4 631 cells/mm3 (IQR = 458–840). At study entry, 7% of participants had slow gait.
Over the 3 years of observation, 87% maintained normal gait speed, 3% maintained a slow gait, 6% developed a slow gait, and 4% improved from slow to normal gait speed. The prevalence of each gait speed trajectory group is given in Figure 1. Median time to complete the 4-m walk in each gait speed trajectory group at baseline and at each year of follow-up in the study is given in Supplementary Table S1. Characteristics of participants by gait speed trajectory group are given in Table 1. In brief, age, sex, race, HbA1C, BMI, waist circumference, level of physical activity, peripheral neuropathy, alcohol and illicit drug use, use of anxiolytic or antidepressant medications, TDF use at HAILO study entry, neurocognitive function, presence of kidney or liver disease, hypertension, and diabetes differed across groups. Between HAILO participants included in and excluded from this analysis, there were no significant differences in age; sex; HIV virologic control; current or nadir CD4; ART treatment history; BMI; reported physical activity; or use of alcohol, cigarettes, other substance use, or antidepressants or anxiolytics. Black non-Hispanic, white non-Hispanic, and Hispanic participants were more likely to be included in the analysis than Asian, Pacific Islander, and American Indian, Alaskan native participants. In addition, excluded participants had a higher median HbA1C (5.6 vs. 5.5, p = .01).
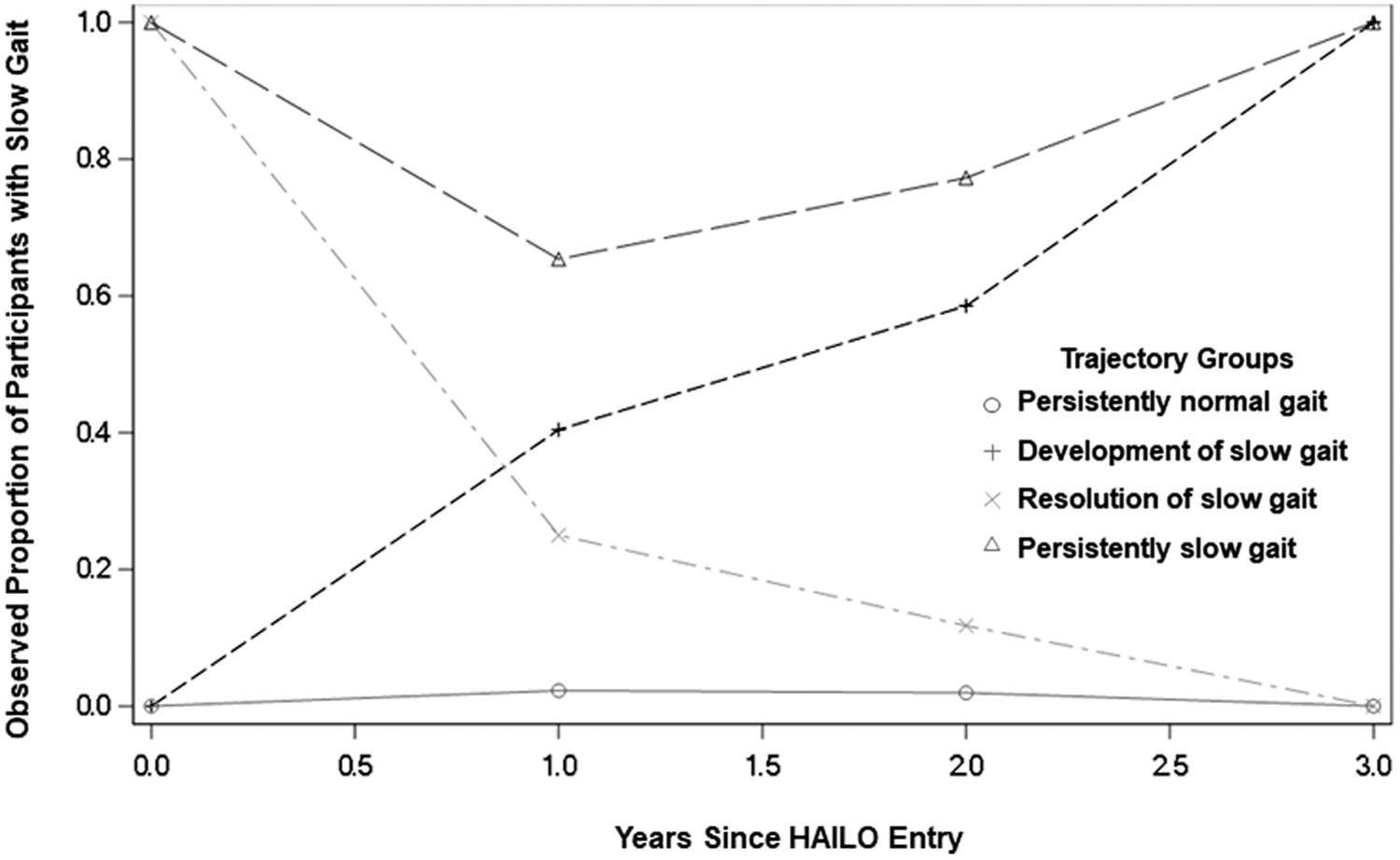
Prevalence of slow gait within each gait speed trajectory group. Over 3 years of observation, 87% of HAILO participants maintained normal gait speed, 3% maintained a slow gait speed, 6% developed a slow gait, and 4% improved from a slow to a normal gait speed. HAILO, HIV Infection, Aging, and Immune Function Long-term Observational Study.
Demographic and Clinical Characteristics by Gait Speed Trajectory Categories
Chi-square tests were used for categorical variables and the Kruskal–Wallis test for continuous variable was used to assess differences in demographic and clinical characteristics between gait speed trajectory groups. Characteristics were measured at baseline unless otherwise indicated.
ART, antiretroviral therapy; AZT, zidovudine; BMI, body mass index; CD4, CD4+ T lymphocyte count; D4T, stavudine; DDI, didanosine; EFV, efavirenz; HAILO, HIV Infection, Aging, and Immune Function Long-term Observational Study; HbA1C, hemoglobin A1C; INSTI, integrase strand transfer inhibitor; NCI, neurocognitive impairment; PI, protease inhibitor; TDF, tenofovir disoproxil; VL, viral load.
Characteristics associated with development of slow gait
In the age-adjusted bivariate models, the development of slow gait was associated with female sex, black versus white race, Hispanic ethnicity versus white race, 12th grade and higher education, higher HbA1C percentage, higher BMI, elevated waist circumference, no alcohol versus light alcohol use, lower NPZ3 score, NCI, and peripheral neuropathy (Supplementary Table S2). Each of these covariates was included in the multivariable model.
In the multivariable model (Table 2), development of slow gait was associated with increase in baseline HbA1C percentage, per one unit increase [odds ratio (OR) = 1.36; 95% confidence interval (CI) = 1.03–1.81; p = .033], presence of NCI (OR = 3.47; 95% CI = 1.57–7.69; p = .002), and black versus white race (OR = 2.45; 95% CI = 1.08–5.59; p = .033). When the models were restricted to nondiabetic participants, development of slow gait was associated with NCI (OR = 4.14; 95% CI = 1.94–8.84; p < .001) and black race (OR = 2.56; 95% CI = 1.12–5.81; p = .025) but not HbA1C (age-adjusted OR = 1.24; 95% CI = 0.58–2.63; p = .57). In contrast, a multivariable model restricted to diabetic participants showed an association between HbA1C and development of slow gait (OR = 1.50; 95% CI = 0.99–2.27; p = .054).
Factors Associated with Gait Speed Change in Multivariable Models
Covariates with p < 0.05 are italicized and in bold.
Characteristics were measured at baseline unless otherwise indicated.
CI, confidence interval; OR, odds ratio.
Sex and race/ethnicity-stratified models were also fit. Among men, the odds of developing slow gait were associated with NCI (OR = 3.69; 95% CI = 1.37–9.94; p = .01), HbA1C (OR = 1.58; 95% CI = 1.15–2.16; p = .004), and a marginal association with greater BMI (OR = 1.07; 95% CI = 0.99–1.16; p = .079). In women, only NCI (OR = 4.06, 95% CI = 1.36–12.2; p = .012) was associated with development of slow gait. In a multivariable model restricted to black non-Hispanic participants, the odds of developing slow gait were lower for those with at least a high school education (OR = 0.22; 95% CI = 0.07–0.73; p = .014) and greater with higher HbA1C (OR = 1.51; 95% CI = 1.07–2.14; p = .018). Among Hispanic participants, development of slow gait was associated with NCI (OR = 6.74; 95% CI = 1.62–28.10; p = .009) and high waist circumference (OR = 4.27; 95% CI = 1.10–16.5; p = .035). In this group, older age tended to be associated with greater odds of developing slow gait, although this was not statistically significant (OR = 1.07; 95% CI = 0.99–1.16; p = .09). No baseline characteristics were significantly associated with development of slow gait among white, non-Hispanic participants.
Characteristics associated with resolution of slow gait
The age-adjusted bivariate model (Supplementary Table S2) showed that resolution of slow gait was inversely associated with higher BMI and elevated waist circumference; these factors were included in the final, multivariable model. In the multivariable model (Table 2), age was the only factor associated with improvement from slow to normal gait speed, with older individuals less likely to improve (OR = 0.92 per year; 95% CI = 0.86–0.98; p = .013). In nondiabetic participants, no factors examined were significantly associated with resolution of slow gait in the multivariable model. Among participants with diabetes, resolution of slow gait was significantly associated with being physically active (OR = 26.0; 95% CI = 1.29–520; p = .033) and younger age (OR = 0.82 per year increase; 95% CI = 0.68–0.97; p = .024).
In the sex-stratified model of men alone, increasing age (OR = 0.90; 95% CI = 0.83–0.98; p = .011) and BMI (OR = 0.88; 95% CI = 0.79–0.99; p = .03) were inversely associated with resolution of slow gait. Among women, no characteristics were associated with improvement in slow gait. In a model restricted to black non-Hispanic participants, resolution of slow gait was inversely associated only with older age (OR = 0.85; 95% CI = 0.76–0.95; p = .003). Among Hispanics, older age also tended to be associated with lower odds of resolution of slow gait, although this was not statistically significant (OR = 0.88, 95% CI = 0.76–1.02; p = .09). No baseline characteristics were significantly associated with resolution of slow gait among white, non-Hispanic participants.
Discussion
Gait speed declines more rapidly with age among PWH than in HIV-uninfected individuals, but a longitudinal assessment of characteristics related to this functional outcome have previously been limited. In this large cohort of men and women living with HIV, we found that development of slow gait speed was significantly associated with higher HbA1C, NCI, and black race. These findings reveal a modifiable risk factor (HbA1C) and vulnerable populations (individuals who have NCI or black race) that may benefit from early screening and intervention to preserve physical function in PWH.
Associations between impaired neurologic and physical function have been noted among older populations of people with and without HIV. 35,36 Previous cross-sectional analysis in PWH have shown a relationship between slowed gait and more advanced AIDS dementia complex stage. 30 Structural changes in brain regions involved in both cognitive and motor function may provide a mechanistic explanation for this relationship. Both gait and cognition are vulnerable to impaired communication between brain regions in long white matter tracts. A small cross-sectional study of men and women (average age 50.6 years) in the Hawaii Aging with HIV cohort showed volumetric changes in brain regions (cerebellar white matter and subcortical gray matter) linked to cognition and motor control. 37 In a previous cross-sectional analysis of the HAILO cohort, we reported an association between impaired cognitive function and gait speed. 25 This study adds longitudinal evidence from this large, well-characterized cohort of PWH, where we similarly find that NCI is strongly associated with development of slow gait.
Similarly, abnormal glucose metabolism has been associated with gait speed decline in the general population. 38 –42 Decreased muscle quality and strength and mitochondrial dysfunction have been identified as potential causes of this relationship. 43,44 Among diabetic participants, inflammation has been linked to increased risk of functional decline. 45 Among men with HIV compared with seronegative controls, inflammation and insulin resistance have previously been associated with frailty, a complex phenotype of which gait speed is a key component. 20 We found that the association between increased HbA1C and development of slow gait was most apparent among diabetic participants. These results suggest that individuals with both diabetes and HIV represent a particularly high-risk group for development of functional impairment.
In addition, studies of the general population have noted a complex interplay between insulin resistance and cognitive and physical dysfunction. 46 Hyperglycemia, insulin resistance, and hyperinsulinemia have been associated both with frailty and cognitive performance in HIV cohorts. 20,47,48 A recent study of MACS participants showed HIV and diabetes interact to produce white matter changes and that the extent of these structural alterations was significantly associated with psychomotor speed. 49 Previous studies have shown that cerebral white matter disease links these three characteristics. White matter T2/FLAIR hyperintensities and abnormal diffusion tensor imaging are present in conditions such as cerebral microvascular disease and HIV. 50,51 Because of the relatively low incidence of marked slowness as defined for this cohort, we were not sufficiently powered to detect interactions between A1C and NCI and the development of impaired gait speed. Additional analyses as this cohort continues to age will help to further characterize these relationships.
Our findings suggest that strategies to prevent and treat hyperglycemia may help avert functional impairment in PWH. Pharmacologic interventions, including metformin, to improve glucose control have shown some promise in elderly individuals with diabetes. 52 –54 However, the risks and benefits of such therapies must be carefully considered. Because of an increased risk of hypoglycemia, intensive glucose treatment may not be appropriate for aging PWH who are vulnerable to other geriatric syndromes such as polypharmacy and falls. 55 –57 Lifestyle interventions may help prevent insulin resistance in PWH and lead to improved glucose control and functional outcomes in individuals with known diabetes. 58,59 Dietary and exercise interventions to thwart excess weight gain and reduce obesity are essential to prevent development of diabetes and physical limitations. 60 In addition to weight benefits, exercise-based interventions promote physical function in older diabetic and nondiabetic participants alike. 29,61 –63 Indeed, in our analysis of participants with diabetes, physical activity was significantly associated with resolution of slow gait. This finding suggests that physical activity is a key intervention to maintain gait speed in older PWH, particularly those with diabetes.
In this study, we also found that black race had a significant association with development of slow gait. A previous analysis of gait trajectories among participants in the Multicenter AIDS Cohort Study also found significantly faster declines in nonwhite men with and at risk for HIV. 5 Higher rates of impaired physical function among older individuals of black race have been previously noted in the general aging population. 64,65 These differences are incompletely understood but have been linked to increased disease burden and socioeconomic inequalities. 66 Indeed, increased education (completion of high school or beyond) was protective against development of slow gait among black participants, suggesting that socioeconomic disparity may in part be driving this difference. Furthermore, among black participants in this study, increasing HbA1C was significantly associated with development of slow gait, suggesting that black PWH should be prioritized for early screening and interventions for insulin resistance.
Several limitations of this study must be acknowledged. Although the HAILO cohort is diverse, its participants have been continuously enrolled in ACTG trials and observational studies since at least 2009. As a result, they may be more adherent and not be fully representative of the general population of older PWH. In addition, women remain underrepresented in this cohort and only account for 19% of participants included in this study. Similarly, the restricted number of participants in each subgroup analysis limits the power of our findings. As such, our preliminary study did not allow for more complex analysis of the relationship between NCI and gait speed. Without a control group of participants who do not have HIV, it remains unclear whether our findings are specific to or accentuated among PWH. Furthermore, there are limitations in obtaining some of the characteristics considered in this analysis. Minor differences in gait speed measurement may have persisted across sites, although all sites receive regular training and quality control procedures. Physical activity was assessed by self-report, which may be unreliable. Although the 4-m gait speed test is a useful screening tool, it is an acute stressor test and does not capture physiologic reserve and exercise tolerance in the setting of prolonged stressor conditions such as the 400-m walk test. Finally, the A5001 Neuroscreen is a limited assessment of neurocognitive function and may not capture all cognitive domains affected in participants.
The growing number of older PWH are vulnerable to poor health outcomes such as disability and reduced quality of life. 7,22,67 Targeted interventions to preserve physical function and independence and promote resiliency is imperative in this population. As decline in gait speed was associated with increased HbA1C, NCI, and black race, we have identified those at the highest risk for physical function impairment who may benefit most from screening, prevention, and early intervention. Moreover, the association between baseline HbA1C and development of slow gait speed highlights an intervenable target to prevent progression of physical function limitations.
Footnotes
Acknowledgment
The authors thank the ACTG A5322 HAILO Study Team.
Disclaimer
The content is solely the responsibility of the authors and does not necessarily represent the official views of the National Institutes of Health.
Author Disclosure Statement
No competing financial interests exist.
Funding Information
Research reported in this publication was supported by the National Institute of Allergy and Infectious Diseases of the National Institutes of Health under award number UM1 AI068634, UM1 AI068636, UM1 AI106701, and NIAID K24 120834 (to T.T.B), the National Institute of Aging K32 63008845 and R01 AG0504366 (to K.M.E); and National Institute of Diabetes and Digestive and Kidney Diseases T32 DK007169 (to M.C.M.).
Supplementary Material
Supplementary Table S1
Supplementary Table S2
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.