
Abstract
Balance deficits impose limitations and can impede safe walking contributing to falls and falls-related complications. The objective of this study was to perform an in-depth balance assessment and compare domains of limitations in older men with and without HIV infection. Fifteen sedentary African American men either with HIV (n = 6) or without HIV (n = 9 controls) participated. Standing balance was assessed under quiet stance on dual synchronized force plates during three 30 s trials with eyes open. Participants also completed standardized clinical instruments of balance, including the Berg Balance Scale (BBS) and Dynamic Gait Index (DGI). Older participants with HIV have lower BBS and DGI scores than controls (both p < .05). Adults with HIV have nearly twice the magnitude greater center of pressure (COP) sway variability than controls (1.42 ± 1.20 cm2 vs. 0.71 ± 0.1 cm2, p < .05). These data demonstrating differences in COP sway area between groups may further support evidence of potential fall risk and contribute to frailty in older adults with HIV.
Introduction
Frailty is common in adults living with HIV, and includes diminished functional performance 1 such as reduced ambulatory capacity, decline in physical activity, 2 and weakness (e.g., grip strength) 3 with a link between HIV infection and acceleration of frailty measures. 4 In older adults, frailty predicts poor health outcomes related to mobility and physical function. 3,5 –7 There are few studies to-date that have reported mechanistic balance deficits in individuals living with HIV. This is despite the fact that balance deficits are known to impose limitations in weight bearing (static or standing balance) and impede safe walking (dynamic balance), both independently and collectively contributing to falls and falls-related complications. The incidence of falls in adults with HIV is high 8 with frailty as a contributing factor. 9 Fall risk in middle-aged (average age 48 years) men and women patients with HIV is associated with increased number of medications, more than three comorbidities, and noncompliance with antiretroviral therapy (ARV). 10 In middle-aged adults with HIV, the odds of falling increased 1.7 and 1.4 for each comorbidity and medication, respectively, and was higher in those with frailty or disability among other conditions. 11 In the AIDS Clinical Trials Group A5322, older prefrail and frail individuals with HIV were at a significantly higher risk for falls than nonfrail individuals with slow walking speed and grip strength associated with recurrent falls. 9 Yet, a systematic review and meta-analysis point to insufficient quantification of locomotor impairments in adults with HIV. 12 In a study sample of 14 young asymptomatic adults with HIV, a decrease in lateral velocity during static balance (eyes open) and increase in anterior–posterior (AP) velocity during static balance (eyes closed) was reported as well as electromyography (EMG) changes with sudden tilt movement indicative of disturbances of dynamic balance. 13 Poor standing balance is reflected by center of pressure measures (see section “Materials and Methods”) in subjects with early HIV 14 ; neurologically asymptomatic HIV infection, 15 beginning HIV-1-related encephalopathy, 15 and HIV with comorbid psychiatric disorders 16 have also been reported. There is also limited evidence that static balance (eyes open) improves with a 3-month aerobic, strength, and balance program in middle-aged adults with HIV. 17 Thus, little is known about the mechanisms for balance problems which contribute to fall risk and frailty in older adults with HIV. Hence, the purpose of this preliminary investigation was to perform an in-depth balance assessment and compare domains of limitations in older men with and without HIV infection.
Materials and Methods
Study population and design
This cross-sectional pilot study includes baseline data from six HIV-infected men and nine hepatitis C virus (HCV) monoinfected men. All men were African American. The control group was selected among those with a similar substance abuse history and socioeconomic background who had chronic active Hepatitis C diagnosed as a positive test for HCV RNA and no history of antiviral treatment. Among the six HIV-infected men, five had history of HCV and one individual had durable viral suppression after prior antiviral therapy.
Exclusion criteria for both groups included poorly controlled hypertension (systolic pressure >180 mmHg or diastolic pressure >105 mmHg), severe anemia (hemoglobin <10 g/dL), and end-stage renal and liver disease. Subjects had to be free of any AIDS defining conditions for 6 months before enrollment. 18 HIV-infected men were also required to be on stable (≥6 months) ARV. All participants were sedentary (<20 min of aerobic exercise 2 × /week) before enrollment. Written informed consent was obtained from all subjects. Studies were approved by the University of Maryland, Baltimore Institutional Review Board and the Baltimore VA Medical Center Research and Development Committee.
Testing
Outcome assessors were blinded to HIV status for all testings. All testings were performed in a single visit.
Balance function
Standing balance was assessed under quiet stance on dual synchronized force plates during three 30 s trials with eyes open. Changes in control of postural stability under quiet stance was quantified by the whole-body center of pressure (COP) sway elliptical area, 19 –21 which was computed from the stabilogram [COP time series in the AP vs. mediolateral (ML) planes]. Before using this method, ground reaction force (GRF) signals were obtained using a strain gauge Bertec 4060-10 force platform and Bertec AM-6701 amplifier (Bertec Corp., Columbus, OH). Raw GRF data were sampled at 100 Hz and transformed to obtain COP values. Subsequently, an ellipse fit method is used, which consists of fitting a 95% confidence ellipse to the stabilogram (COP time series in the AP vs. ML planes). In other words, this ellipse quantifies 95% of the total area covered in the ML and AP directions.
The ellipse area is considered to be an index of overall postural performance—specifically, the variability of postural control or body sway. This is our primary measure for standing balance—a lower value reflects better standing balance, and vice versa. 22 The novelty of this method over clinical measures is that it yields multiple parameters, each of which provides a unique performance attribute related to standing balance.
To measure stride length, participants walked over ground at self-selected comfortable speed on an 8-m instrumented walkway (GAITRite; CIR Systems, Clifton, NJ) with at least two strides before the start and after the end for acceleration and deceleration. First and last steps were not included in the analyses to eliminate partial foot contacts at the extremes of the recording area. Tests were repeated three times, allowing 1-min rests between them, with the average across the three trials used for analysis.
In addition, subjects completed the Berg Balance Scale (BBS) and Dynamic Gait Index (DGI). These standardized clinical instruments of balance and self-report of falls efficacy are reliable and validated for older adults. The BBS 23 (out of 56 items), is a 14-item scale and each item scored 0–4 for a maximum of 56 points. The DGI 24 Scale evaluates balance impairments with an eight-item scale that includes ratings (0–3) on walking, walking while changing speed, walking while turning head-horizontally and vertically, walking with a pivot turn, walking over and around obstacles, and stair climbing.
Participants completed the short physical performance battery (SPPB), a comprehensive well-established measure of physical function that includes balance testing, timed 4-m walk, and timed repeated chair stands. Scoring was performed as per validated methods. 25
Statistical analyses
Descriptive means were calculated on variables. Unpaired t-tests or Fisher's exact test were used to test differences by group. Statistical significance was set at a two-tailed p < .05. Data were analyzed using SPSS Statistics 22 (SPSS, Inc., Chicago, IL); results are expressed as mean ± standard deviation.
Results
Subject characteristics are reported in Table 1. There was no difference in age, body weight, and body mass index between groups. Smoking status and comorbidities also did not differ by group. Five of the six participants with HIV had suppressed HIV replication (HIV-1 RNA <40 copies/mL) and a high CD4 cell count, consistent with stable ARV use (Table 1).
Characteristics of Participants With and Without HIV
BMI, body mass index; SD, standard deviation; ARV, antiretroviral therapy; HCV, hepatitis C virus; AA, African American; C, Caucasian; NRTI, nucleoside reverse transcriptase inhibitor; NNRTI, non-ucleoside reverse transcriptase inhibitor; PI, protease inhibitor; ISI, integrase inhibitor.
Participants with HIV have lower BBS than controls (48 ± 4 vs. 52 ± 5, p < .05, Fig. 1). In addition, participants with HIV have lower DGI scores than controls (19.5 ± 3.5 vs. 23 ± 1, p < .05, Fig. 2). SPPB scores did not differ between participants with and without HIV (10 ± 1 vs. 9 ± 3). Pooled BBS scores correlated with DGI scores (r = 0.74, p = .02), but not within only men with HIV and men without HIV, although the correlation trended toward significance in participants with HIV (r = 0.92, p = .07).

Comparisons of BBS score between older adults with HIV (n = 6) and those without HIV (n = 9). BBS, Berg Balance Scale. *p < 0.05.

DGI score between older adults with HIV (n = 6) and those without HIV (n = 9). DGI, Dynamic Gait Index. *p < 0.05.
Participants with HIV have nearly 100% greater or twice the magnitude COP sway variability (elliptical area) than controls (1.42 ± 1.20 cm2 vs. 0.71 ± 0.1 cm2, p < .05, Fig. 3). Finally, instrumented gait measures show impaired gait in participants with HIV as evidenced by a trend for shorter stride lengths compared to controls (132.9 ± 26.6 cm vs. 144.5 ± 15.3 cm, Fig. 4). COP area was not correlated with BBS score or DGI score for both groups and for the pooled data.

COP sway area in the medial–lateral (X-axis) versus anterior–posterior (Y-axis) plane under quiet stance between older adults with HIV (n = 6) and those without HIV (n = 9). COP sway area reflects static balance quantified by the 95% confidence COP ellipse derived using force plate ground reaction forces. In this measure, smaller ellipse reflects less sway and hence better standing balance and vice versa. The solid black color ellipse reflecting greater variability in standing balance is for participants with HIV. *p < .05. COP, center of pressure.
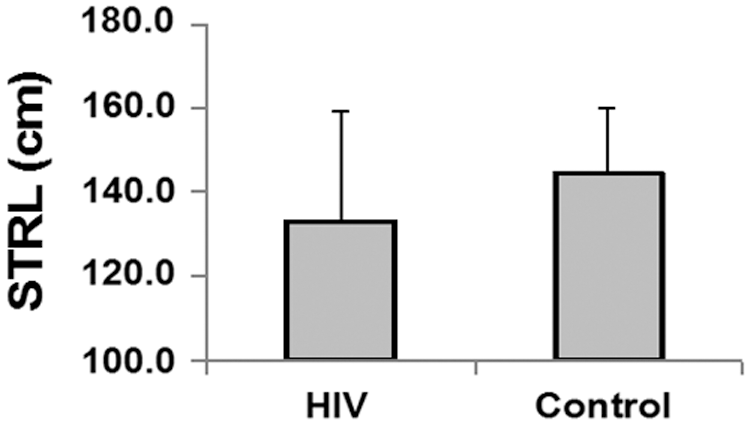
Stride length (STRL) during self-selected preferred walking speed between older adults with HIV (n = 6) and those without HIV (n = 9).
Discussion
Results from this preliminary study utilizing a battery of methods to quantify mobility function in a population at risk for frailty with movement disorders indicate worse balance in older adults with HIV compared with HIV negative controls with similar HCV status as evidenced by clinical scales and poor control of postural stability under quiet stance indicated by greater sway area. Our data support our hypothesis that older adults with HIV have impaired balance, gait, and functional mobility as evidenced by clinical and quantitative instrumented measures, and it requires further study.
Balance is an important factor contributing to falls and falls-related complications. In part, a facet of the problem could be the lack of quantitative techniques and objective measures to accurately discern changes in functional performance related to mobility. For example, there is limited evidence that body weight supported treadmill training that positively impacts balance in other populations such as those with stroke 26 and older adults, 27 but those gains may not be reflected due to not applying suitable balance measures to adequately capture dynamic balance in walking. This is significant; as dynamic balance during gait is poorly understood, despite the fact that walking has often been thought of and modeled as a series of “controlled falls.”
There have also been limited studies to-date that have investigated the quality of gait in older adults with HIV, beyond “global” measures such as walking speed. In a meta-analysis of gait and balance impairments in adults with HIV, balance was assessed using instrumented and clinical tests with results indicating that adults with HIV walk slower and have increased center of pressure excursions and long loop postural reflex latencies. 12 However, gait deficits emerge from more pervasive underlying biomechanical mechanisms that profoundly affect the biomechanics 28 and sensorimotor control 29 of both legs. For example, impaired ankle control resulting from dorsiflexor weakness impacts the ability to safely clear the ground during swing, position the foot for a safe and stable landing, and diminishes mechanical power for push off, 30,31 resulting in slower walking speeds and compensatory (e.g., asymmetric) gait. Hence, there is a need to look beyond “global” measures; kinematic and kinetic gait metrics may be key to revealing a fuller impact of disease-induced changes in walking function.
The same meta-analysis 12 showed the use of BBS 14 and COP measures 15 to quantify balance function in adults with HIV, but these two studies were conducted early in the HIV epidemic and may be less relevant to modern HIV. Stride length has not been used previously by any HIV study as a measure of gait function; however, doing so may provide information on the dynamic control of balance during gait. In this study, slower gaits indexed by shorter stride lengths, as evidenced here, have been shown to be directly associated with an increased fall risk, 32 and are correlated with poorer balance (greater COP sway). Collectively, these results indicate that many clinical and instrumented measures of gait and balance function are lacking in scope and accuracy use to measure mobility and frailty for the HIV population.
Standardized clinical instruments of balance such as the BBS and self-report of falls efficacy are reliable and validated for older adults. Our results indicate that the mean difference in BBS score between the participants with HIV and without HIV (ΔBBS = 3.25) is considered functionally or clinically significant. For example, cross-sectional studies in elderly people (>65 years) 33 have shown that the minimum detectable change at 95% confidence for the BBS is 4 points for patients with baseline scores within 45–56 range (both with and without HIV groups), consistent with the finding in our data. Note that BBS and DGI measures have been shown to be reliable for assessing static balance and fall risk, and ability to modify balance while walking in the presence of external demands, in adult populations. The rationale for using BBS and DGI measures in the adult HIV population is further strengthened given the functionally significant BBS difference between HIV groups (3.25 points) and that the pooled BBS was strongly correlated with DGI in our study.
We chose to use instrumented balance measures, for example, force platform posturography conducted during quiet stance, because they generate measures such as COP sway area that are less prone to inter- and intrarater variability than observed in most clinical balance measures, for example, BBS and DGI. Another benefit of using COP measures is that, unlike clinical measures, various parameters derived from the COP signal provide different types of information on postural control mechanisms, 34 predict falling risk, 35 –38 and evaluate the efficacy of balance training programs. 39,40 Because of these benefits, COP-based measures have been used extensively to study overall postural performance as well as underlying postural mechanisms in multiple populations, including athletes, 22,41,42 older healthy adults, 43,44 adults with diabetic sensory neuropathy, 45 adults with cerebellar ataxia, 46 and Parkinsonian and osteoporotic subjects, 47 to name a few.
Despite inherent benefits, their use in the adult HIV population has been scarce; our study is one of few that is reporting COP-based data along with spatial-temporal gait parameters such as stride length. The absence of a strong correlation between the clinical balance measures (BBS and DGI) and force posturography (COP area) is not surprising because of the type of balance information provided by these measures and emphasizes the need for a comprehensive balance assessment. While the clinical measures reliably index static and dynamic task-specific balance, posturography-based measures are more sensitive to characterizing postural control during quiet upright stance. Collectively, however, the combination of the clinical and instrumented battery is likely to provide a more comprehensive assessment of impaired standing and dynamic balance in older HIV adults.
Our primary COP-based balance outcome in this study was the 95% confidence ellipse COP area, chosen because of its importance as an index of overall postural performance. We specifically chose this measure over others such as composite COP sway velocity since the latter has often been interpreted to reflect the efficiency of the postural control system (the smaller the velocity, the better the postural control) while characterizing the net neuromuscular activity required to maintain balance. 48 In this study, however, our goal was to use a single global COP parameter to quantify standing balance in older HIV adults rather than looking at the underlying mechanisms for the control achieved. Thus, our data demonstrating differences in COP sway area between groups may be a better reflection of potential fall risk.
The preliminary study is limited in terms of the small sample size per group and lack of measures of leg strength. While injection drug use was common in both groups, methadone medication use was not available. Strengths of this study is the inclusion of objective measures to quantify mobility function that show high sensitivity in discerning changes in key functional gait and balance domains that are not captured by standard clinical scales.
Factors that may influence impaired balance could include depression and cognitive decline with additional mechanisms of structural damage of central nervous system (CNS) structures (basal ganglia and cerebellum) as possible contributors. In addition, the loss of lower body muscle strength and the muscle quality are important predictors in recovery from impaired balance. Although one might consider peripheral neuropathy to compromise balance in the HIV group, there was no difference in the prevalence between groups. Furthermore, neither peripheral neuropathy nor ARV has been shown to contribute to impaired balance in other studies. 12 Since the control of gait and balance is highly complex and influenced by several neuromotor factors, it is necessary to deploy whole-body techniques, including measuring AP force impulses, 31 components of COP motion, 19 –21 joint kinematics during quiet stance, and gait initiation while walking and during free-living physical activities. In addition, clinical scales (Berg Balance, 23 DGI, 24 Four Square Step Test 49 ) can characterize how older HIV patients with balance impairments can modify gait under different task conditions.
This preliminary report investigated gait and balance in older HIV adults using state-of-art instrumentation as well as measures, both quantitative and objective with enough specificity and sensitivity and clinical scales, to better inform the relationship between mobility and rehabilitation approaches. These biomechanical indices may help predict frailty precursors to better understand how HIV infection and aging exacerbate each other and could potentially inform management of mobility disorders in adults aging with HIV.
Footnotes
Author Disclosure Statement
No competing financial interests exist.
Funding Information
This work was supported by a Veterans Affairs Senior Research Career Scientist Award (Rehabilitation Research and Development), Veterans Affairs Rehabilitation Research and Development Merit (101 RX000667), and the University of Maryland Claude D. Pepper Older Americans Independence Center (P30AG028747).