
Abstract
Chronic inflammation that contributes to the deterioration of the mechanical form of both the vascular wall and the function of endothelial has been shown to cause vascular dysfunction in patients with human immunodeficiency virus (HIV). Nailfold videocapillaroscopy (NVC) is a noninvasive and simple technique used to analyze dermal microvasculature. The aims of our study were to detect the morphological and functional properties of microcirculation in HIV-positive patients utilizing NVC and to compare the results with those obtained from healthy individuals and investigate whether these changes had supported any correlation with HIV. In this prospective study, 51 male HIV-positive patients were the subjects and 59 male healthy individuals made up the control group. Capillaroscopic findings, obtained from both groups by NVC, were evaluated. Tortuosity, a capillaroscopic finding, was significantly higher in the group with HIV (p < .001). In logistic regression analysis, tortuosity [odds ratio (OR), 4.658; p = .001], bizarre capillary (OR, 1.733; p = .319), and capillary ectasia (OR, 0.867; p = .493) were considered significant. The changes of capillaroscopic findings were found to be correlated with HIV. We suggest videocapillaroscopy in the evaluation of microvascular changes in HIV patients, as a dependable contributing method.
Introduction
Antiretroviral therapy (ART) increases the quality and length of life in human immunodeficiency virus (HIV)-infected patients. Non-Acquired Immune Deficiency Syndrome (AIDS) complications related to AIDS, however, cause cardiovascular and cerebrovascular diseases particularly. 1 The cause of these complications is inflammation. 2 Chronic inflammation that contributes to the deterioration of the mechanical structure of both the vascular wall and the function of endothelial has been shown to cause vascular dysfunction in HIV patients. 2 –4
HIV infects the endothelial cells, the release of cytokines by activated monocytes/macrophages. These cytokines cause damage associated with regeneration and activation, a process that may ultimately impair endothelial functions. 5 Most of these complications in HIV patients do not manifest until the further phase and can quickly become worse. Unfortunately, conventional techniques are helpless to define or diagnose these complications until they become evident.
Nailfold videocapillaroscopy (NVC) is a noninvasive, highly sensitive, safe, low-cost, simple, and beneficial diagnostic tool that interprets the microvascular form of the nailfold and allows better evaluation besides monitoring capillary data. 6
We considered that endothelial dysfunction detected by NVC would be different in HIV-positive patients than those would in HIV-negative patients. The aims of this study were to analyze the morphological and functional properties of microcirculation in HIV-positive patients by NVC and to compare the results with those obtained from healthy individuals and investigate whether these changes had any correlation with the virus itself in HIV-infected patients.
Materials and Methods
Patients
In this study, 51 male HIV-positive patients and 59 male healthy controls without cardiovascular risk factors were the subjects from the outpatient clinic of a training and research hospital. Exclusion criteria were comorbid diseases including hypertension, collagen tissue disease, diabetes mellitus, drug usage that affect the fibrinolysis metabolism (such as oral contraceptives and glucocorticoids), alcohol consumption smoking, and working with the risk of microtrauma. All the patients, after providing written consents, were examined by a rheumatologist for capillary evaluation with the NVC device. The study was performed in accordance with the Declaration of Helsinki.
Capillaroscopic assessment
At 20°C–24°C room temperature after a resting of 20 min, the nailfold of all participants was applied with immersion oil for better visualization. Capillaroscopy was performed with capillaroscopy device (Videocap; DSMediGroup, Milan, Italy) on eight fingers of each participant (except the thumbs) at a 200× magnification by a rheumatologist blinded to the condition of the patient and four images (1 × 1 mm in size) from the nailfold in each finger were evaluated. On the videocapillaroscopy device, 32 images were obtained totally and recorded for each patient. According to the Maricq criteria modified by Bergman et al., the nailfold capillary system was assessed for capillary morphology, density, and distribution. 7 In the dermal papillae, the distal capillary rows have a parallel course to the nail surface and can be seen in their whole length in the normal nailfold. In healthy individuals, distal capillary rows appear as red and hairpin-shaped. 8 In patients with rheumatic disorders, characteristic findings on capillaroscopy include dilated capillaries, neoangiogenesis, capillary loss, giant capillaries, and/or vascular areas.
On capillaroscopy, abnormal findings were as follows: (1) bizarre capillaries: abnormal appearance that does not resemble other abnormal capillaries such as clover leaf; (2) tortuous capillaries: two or more cross capillaries per millimeter; (3) avascular area: presence of six or fewer capillaries per millimeter or loss of two consecutive capillaries; (4) microhemorrhage: ≥2 punctate hemorrhage surrounding a single capillary in at least two fingers (either distinct or melding microbleeding areas); (5) ectatic capillary: capillary wall with diameter of >0.02 and <0.05 μm (either regular or irregular); (6) megacapillary: capillary >0.05 μm in diameter; (7) neoangiogenesis: heterogeneous capillaries regarding size with tortuous, bush-like appearance; (a) extreme tortuosity with bush-like, branching, ramified, and coiled capillaries, (b) four or more capillaries in a single dermal papilla, and (c) tiny and branching interconnected capillaries, which originate from a single loop; (8) extravasation: leakage from capillary (Fig. 1). 8,9
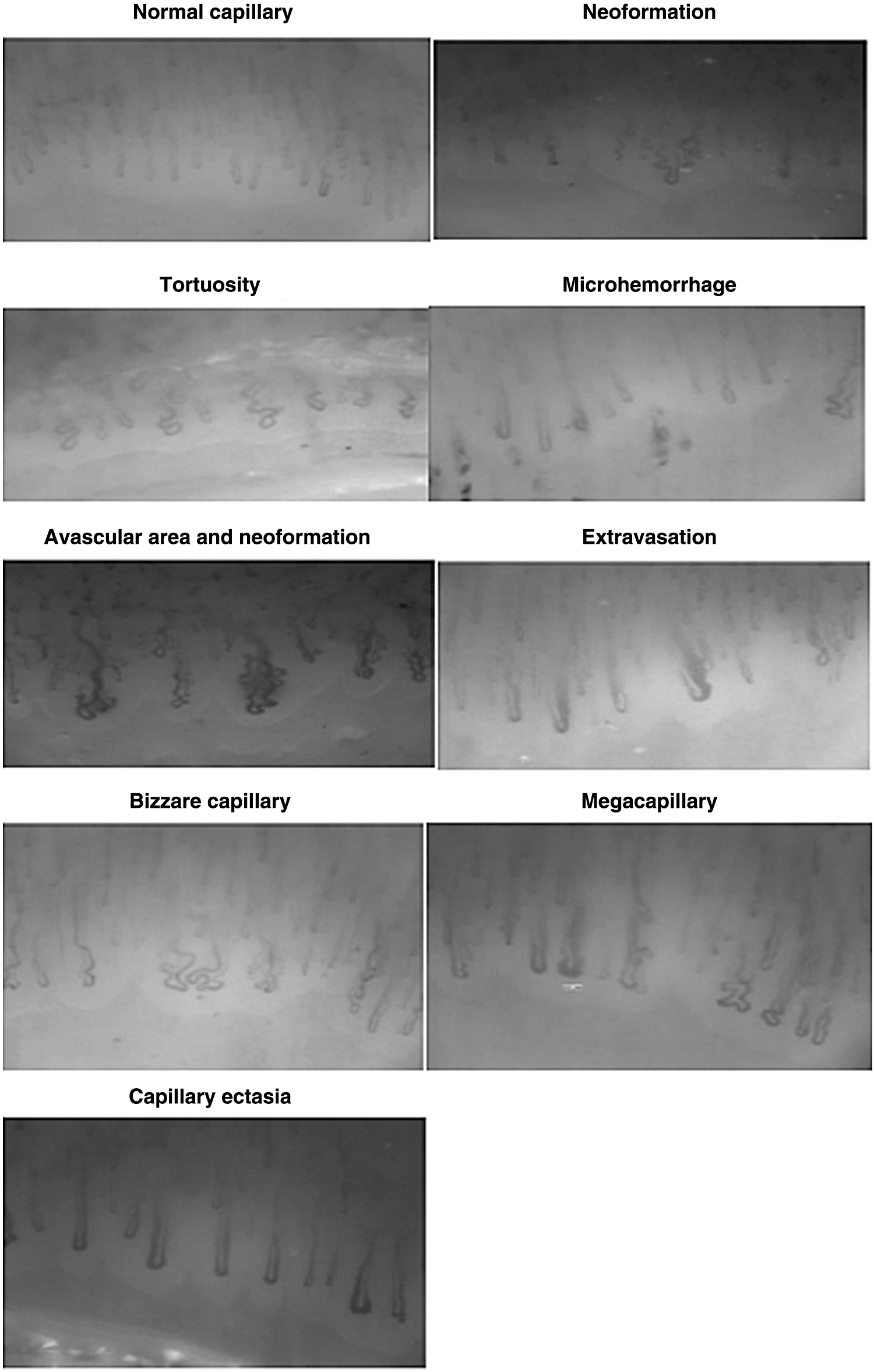
Normal and pathological videocapillaroscopy findings.
Statistical analysis
All data obtained were statistically analyzed on SPSS version 22.0. The p-values refer to the independent sample t-test comparison of the means for the patient and control groups, refer to 0.1, 0.05, and 0.01 level of significance, respectively.
Results
The mean age was 41.79 (20–77) years in the patient group, whereas 42.03 (20–78) years in the control group. The age was comparable in the groups (p = .176). Blood pressure and hemoglobin A1c values were also comparable in two groups (p = .189, p = .196). All the patients and controls were male. The mean disease duration was 15.5 (0–56) months. The patients' number on ART usage was 40 (90%); 5 (10%) patients were not on ART. The demographic and laboratory characteristics of patients with HIV/AIDS are shown in Table 1.
Demographic and Laboratory Characteristics of Patients with HIV/AIDS
The tortuosity was found to be increased significantly in the patient group compared with the control group (p = .009 and p = .000, respectively). Bizarre capillary and capillary ectasia were higher in the patient group than in the control group values (p = .039 and p = .013, respectively). The frequencies of capillaroscopic findings including bushy capillary, neoformation, microhemorrhage, aneurysm, extravasation, megacapillary, meander capillary, avascular area, and interstitial edema were similar in both groups (p > .05) (Table 2). Tortuosity was significantly associated with multivariate logistic regression analysis (odds ratio 4.658, confidence interval 1.811–11.982, p = .001) (Table 3).
Frequencies of Capillaroscopic Findings of Patients with HIV and Healthy Controls
The p-values refer to the independent sample t-test comparison of the means for the patient and control groups.
, **, and *** refer to 0.1, 0.05, and 0.01 level of significance, respectively.
NA, not applied.
Multivariate Logistic Regression Analysis of Significant Capillaroscopic Findings
The dependent variable is equal to 1 for HIV patients and equal to 0 for the controls. Capillary ectasia is an interval variable, and tortuosity and bizarre capillary are dummy variables. ***Tortuosity is significantly associated with HIV.
Discussion
We found that the frequency of tortuosity, a minor capillaroscopic finding, was increased in our HIV-infected patients. Tortuosity is an indicator of endothelial damage. 10 NVC is a proven tool and diagnostic, staging, and prognostic reliability in rheumatology. 11 –13 However, NVC has been used for evaluating microvascular abnormalities in extra-rheumatic diseases. 14,15 To our knowledge, there are a few studies on videocapillaroscopic findings in HIV patients. 16,17 The risk of endothelial dysfunction and subclinical atherosclerosis in HIV patients are higher than they are in non-HIV-infected people. 18 Many factors are implicated in the etiopathogenesis of endothelial dysfunction. The cause of these complications is chronic inflammation. 2 Dysfunction of endothelial is described by elevated levels of the biomarkers of the endothelial lesion and the adhesion molecules of endothelial cells. 19 Both HIV and its treatment have been corporated with hypercoagulable features with vasculopathy and subsequent thrombosis. 18
Our patients have been treated for 15.5 (0–56) months and had a mean HIV viral load of 6.7+E3, only 10% of patients did not use ART. Monocyte activation and chronic inflammation endothelial dysfunction have been widely evaluated among HIV-infected patients following sustained viral suppression. 18 The inflammation is going on in the endothelial walls despite viral suppression. Protease inhibitors have been shown to play a facilitating role of endothelial damage, 20 but our patients were treated with integrase strand transfer inhibitors. Therefore, we estimated that there would be no change in other major and minor capillaroscopic findings.
Maggi et al. showed that videocapillaroscopy alterations were not correlated with CD4 T cell count, HIV disease stage, time from diagnosis of HIV infection, antiretroviral regimen, alcohol consumption, smoking, hyperglycemia, hypercholesterolemia, hypertriglyceridemia, and active intravenous drug addiction. 16 In this study, we neither compare them nor we initially removed them from the study. In Maggi et al. study, the comparison of the capillaroscopy between three groups: sclerodermic, HIV patients, and healthy control groups were performed. They found that capillaroscopy results were altered in 100% of the patients in sclerodermic patients, but the results were normal in the other two groups.
The videocapillaroscopy instrument (200× magnification) was used in our study; it is accepted to be the best actual evaluation method. The evaluation of subclinical atherosclerosis by evaluating intima–media thickness and endothelial function gave new insights on the pathogenesis of functional and structural changes detected in patients with HIV-related vascular disease. 21 The effects of HIV on carotid artery structure may be lifelong. Carotid artery intima–media thickness was measured by carotid artery B-mode ultrasonographic methods, and in many studies, the risk of cardiovascular disease was shown to be associated with the carotid artery intima–media thickness. 22 –24
In this study, we analyzed major and minor capillaroscopic findings in HIV-infected patients. Capillaries of similar appearances, such as the heart, kidney, and brain, are found in other organs. The involvement of these capillaries can result in the development of non-AIDS-associated diseases (cardiovascular disease, renal disease, cognitive impairment, osteoporosis, cancer) in these patients. 1
In conclusion, we defined an increase in capillaroscopic findings in HIV-infected patients compared with healthy controls. In our study, these data will contribute to the larger sample size to suggest on this subject in future studies. However, this noninvasive method may be a preliminary indicator for comorbidities due to chronic inflammation caused by HIV, and in this case, patients' conditions may be observed more effectively.
Footnotes
Author Disclosure Statement
No competing financial interests exist.
Funding Information
The authors received no financial support for the research, authorship, and/or publication of this article.