
Abstract
To assess the efficacy of long-term calcium and vitamin D treatment on bone mineral density (BMD) in HIV+ patients on combined antiretroviral therapy (cART). A retrospective, single-center cohort study. Between March 2010 and July 2012, 268 HIV+ patients were screened for vitamin D and calcium deficiency. Those with proven vitamin D or calcium deficiency received supplementation according to a predefined protocol, and were offered further evaluation of BMD by dual-energy X-ray absorptiometry (DEXA). Calcium and vitamin D status and BMD were assessed at baseline (T0) and approximately one (T1) and 4–6 years (T2) later. Percentual change in BMD of the lumbar spine and hip was compared with reported rates of change in HIV+ patients on cART without standard calcium and vitamin D treatment. The prevalence of vitamin D deficiency and calcium deficiency was 46% and 43%, respectively. Thirteen percent of patients had secondary hyperparathyroidism at baseline. DEXA performed in patients with a deficiency revealed osteopenia in 40% and osteoporosis in 8% of patients. The expected long-term change in lumbar spine and hip BMDs at T2 was −0.7%, −1.5%, and −1.5%, respectively. The measured changes were +2.3%, −0.6%, and −0.6%, respectively. The difference between measured and expected rate of change was significant for the lumbar spine (3.0%, p < .05), but not for the hip. Long-term vitamin D and calcium supplementation improves lumbar spine BMD of HIV+ patients with osteopenia or osteoporosis and with proven calcium and/or vitamin D deficiencies. Screening and treatment are recommended to become part of regular care.
Introduction
Although antiretroviral therapy has improved the life expectancy of HIV-infected (HIV+) patients considerably, it may also have adverse effects. 1 The combination of HIV infection and prolonged exposure to combined antiretroviral therapy (cART) is associated with a higher prevalence of several chronic diseases than in noninfected subjects of similar age and sex. 2 –5 HIV-related osteoporosis and osteomalacia occur relatively frequently and put patients at risk for fractures at a rather young age. 6,7 Recent estimations of the prevalence of osteopenia and osteoporosis in HIV+ individuals range from 48% to 52% and from 10% to 23%, respectively. 8 –10
Prospective and retrospective studies have demonstrated decreases in bone mineral density (BMD) of 2%–6% in the first 2 years after the start of cART, depending on the type of cART. 11 –15 Thereafter, the decrease in BMD appears to slow down to 0%–1% per year in the years that follow. 16,17
The trabecular structure of the lumbar spine appears to be the most susceptible to bone loss. Its decline in BMD after more than 2 years of cART is about 0.14% per year greater than in non-HIV controls in the lumbar spine. No difference has been observed in BMD change between HIV patients and non-HIV controls at the hip. 16
The high prevalence of bone disease in HIV+ patients has been attributed to general risk factors such as tobacco use and low BMI, as well as to HIV-specific risk factors. Of these, HIV RNA levels, the use of tenofovir, and protease inhibitors (PIs) appear to be the most important. 18 –25 The roles of vitamin D and calcium are not clear yet. Several observational studies reported a widely varying prevalence of vitamin D deficiency in the HIV+ population, ranging from 24% to 81%. This large variety is related to differences in geographic locations, ethnic groups, and HIV-specific factors such as medication use. 26 The role of vitamin D and calcium supplementation in HIV+ individuals remains largely unknown. While supplementation of vitamin D and calcium is the cornerstone for treatment of osteopenia and osteoporosis in the general population, the treatment in HIV+ individuals appears to be more complex. 27 –30 Current American guidelines do not offer specific supplementation regimens for HIV+ patients. 31 The European AIDS Clinical Society (EACS) guideline advises to check vitamin D status in people with a history of bone disease or a high risk for fracture, but not routinely in all HIV+ patients. Furthermore, the EACS guideline offers no standard regimen to treat a deficiency or to maintain vitamin D levels within the normal range. 32
Screening for osteoporosis or osteopenia in HIV patients with a calcium and/or vitamin D deficiency is currently not standard practice. The EACS guideline recommends to consider screening patients for reduced BMD if they have at least one risk factor (e.g., postmenopause, men aged ≥50 years, history of low-impact fracture, and glucocorticoid use). 30 This is similar as in non-HIV+ subjects. American expert groups recommend to screen for reduced BMD only in postmenopausal women or men aged ≥50 years. 33
Recently, it has been shown that high-dose vitamin D3 (4,000 IU/day) combined with calcium supplementation (1,000 mg/day) attenuates bone loss in HIV+ patients starting cART by about 50%. 34 This beneficial effect was observed despite the fact that only 25% of the included patients had vitamin D levels less than 50 nM. The present study addresses a different type of HIV+ patients. It was designed to assess the impact of a standardized calcium and vitamin D treatment regimen on bone density in patients on cART with a documented vitamin D and/or calcium deficiency and a reduced bone density.
Patients and Methods
Patients
Routine screening for vitamin D and calcium deficiency in HIV+ patients in Rijnstate Hospital, Arnhem, The Netherlands, was started in March 2010. All patients who were screened between March 2010 and December 2012 were eligible for inclusion. Only patients with proven calcium and/or vitamin D deficiency were offered further evaluation of bone density. Patients already using calcium and vitamin D, and those starting bisphosphonate or denosumab treatment during the study period were excluded.
Ethical approval
This study was approved by the local ethics committee.
Definitions and treatments
Vitamin D deficiency was defined as a serum 25-hydroxyvitamin D (25OHD) level <50 nM. 35 Vitamin D-deficient patients were treated with water-soluble cholecalciferol 50,000 IU/mL with the aim to raise serum 25OHD to a level of 75 nM. All patients received a cholecalciferol loading dose that was calculated, based on body weight and baseline serum 25OHD levels, according to the following equation: Loading dose in IU = 40 × (75–25OHD) × body weight. 36 The calculated dose was rounded off upward to the next 25,000 IU, and was administered in portions of 50,000 IU/week orally until the full dose was reached. Subsequently, all patients received a maintenance dose of 50,000 IU once a month, taken on the first day of the month. 37
Calcium deficiency was defined as a urinary calcium excretion <4 mmol/24 h. 38 Calcium-deficient patients were treated with calcium carbonate, 1,000 mg once daily.
Osteoporosis was defined as a T score < −2.5, and osteopenia as a T score between −1 and −2.5. 39
Measurements
Laboratory investigations and dual-energy X-ray absorptiometry (DEXA) scans were performed at baseline (T0), about 1 year after the start of treatment (T1), and at the end of the study (4–6 years after the start of the treatment) (T2). Blood samples were taken in the fasting state, between 8.00 and 10.00 a.m., for the measurement of serum calcium, albumin, parathyroid hormone (PTH), and serum 25OHD. Twenty-four-hour urine samples were collected to assess urinary calcium excretion. Measured serum calcium was corrected for albumin levels using the following formula: Cacorr = total calcium—(0.025 × albumin) +1, expressed in mM.
Assays
Serum 25OHD was measured by immunoassay, and serum calcium and albumin were measured by the photometric method on a routine clinical chemistry analyzer (Modular E170 and P800; Roche Diagnostics, Almere, The Netherlands). Serum-intact PTH was measured by a solid-phase, two-site chemiluminescent immunoassay (Immulite 2000 XPi; Siemens, Los Angeles, CA). The reference range for this assay was 1.3–6.8 pM.
Bone density measurements
BMD measurements of the lumbar spine and the right and left hip were performed by DEXA scanning with the Lunar iDXA densitometry (GE Health Care, Madison, WI).
Analysis
The measured percentual changes in BMD were compared with expected changes in BMD, as reported in the literature, for the early as well as the late period of cART use. 12,13,15 –17,20 The expected rate of change was adjusted for the duration of cART use because previous studies have shown that the decrease in BMD is the highest in the first 2 years after initiation (early phase) of cART than in the years to follow (late phase). 11 –17 To assess the expected rate of change in BMD in patients, the weighted average of the expected change in hip and lumbar spine BMD was calculated based on the studies in Supplementary Tables S1 and S2, the early and late phase, respectively. This yielded an annual change in lumbar spine and hip BMD during the first 2 years after initialization of cART of −1.3% per year and −1.4% per year, respectively, assuming a linear change in BMD. Based on the studies summarized in Supplementary Table S2, the expected annual change in BMD in lumbar spine and hip after the first 2 years on cART was +0.09 per year and −0.2% per year, respectively (late phase), again assuming a linear change in BMD.
For each patient, we calculated the total expected rate of change in BMD of the lumbar spine and hip as follows:
Expected Rate of Change in BMD after total follow-up = Expected Rate of change in Early phase + Expected Rate of Change in Late Phase.
Expected Rate of change in Early Phase = −1.3% (lumbar spine)/or −1.4% (hip)/year x number of years a patient was followed in their early phase
Expected Rate of Change in Late Phase = +0.09% (lumbar spine)/or −0.2% (hip)/year x number of years a patient was followed in their late phase.
Baseline characteristics are described as mean values ± SDs. The paired t-test was used to analyze the difference between the measured and the expected rate of change in BMD, and to analyze the difference between the mean serum calcium, urinary calcium, and serum vitamin D at T0 and T2. A p-value < .05 was considered significant. All statistical analyses were performed using SPSS version 25 software.
Results
Patient inclusion and baseline characteristics
The screening and selection procedure is illustrated in Figure 1. In total, 268 consecutive HIV+ patients were screened. One hundred eighty (67%) patients had calcium and/or vitamin D deficiency: 125 patients were diagnosed with vitamin D deficiency (47%), 117 patients were diagnosed with calcium deficiency (43%), and 62 patients had a combined vitamin D and calcium deficiency (24%). All 180 patients with a proven calcium or vitamin D deficiency were offered a DEXA scan and 143 patients agreed to participate. Sixty-nine patients (49%) had a reduced BMD and were included for long-term follow-up. Their mean age at inclusion was 43 years and mean BMI was 23.9 (kg/m2). Mean CD4 T cell counts were 546 (SD 234), 94% of all patients had CD4 T cell counts >200 cells/mm3. None of the patients was cART naive. At inclusion, they had been using cART for 3–191 months, with a mean of 70 months (Table 1). Osteopenia was diagnosed in 57 (40%) patients, and osteoporosis in 12 patients (8.4%). Follow-up DEXA scans at T2 were available in 61 of 69 patients with a reduced BMD at baseline. Three additional patients had to be excluded because denosumab treatment for osteoporosis was started in the period between their second and third DEXA scan. Thus, long-term follow-up DEXA scans were available in 58 of 69 patients (84%) initially included in the study. The mean follow-up was 15 ± 7.6 months at T1 and 70 ± 14.5 months at T2.
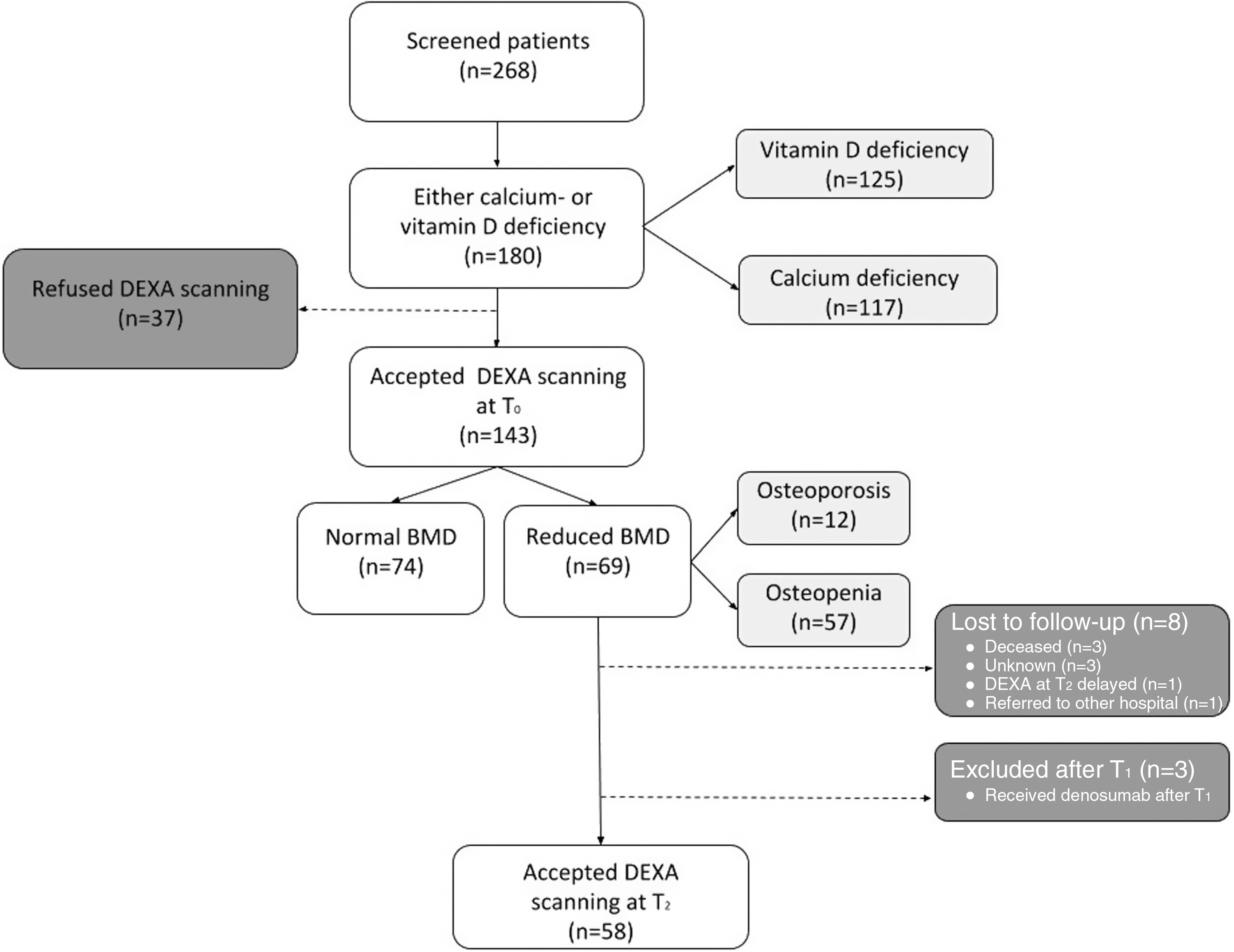
Screening, inclusion, and follow-up. Dashed line represents excluded patients. Figure can be viewed in greater detail online.
Baseline Characteristics of HIV+ Patients with Vitamin D and/or Calcium Deficiency and a Reduced Bone Mineral Density
Values are shown as mean ± SD unless otherwise specified.
These patients (n = 3) used combinations of dolutegravir, abacavir, lamivudine, and nevirapine.
Changes in vitamin D and calcium status
Vitamin D and calcium deficiency was diagnosed in 34 (49%) and 53 (77%) patients who were included for DEXA follow-up at T0. Twenty-two (32%) of all included patients had a combined vitamin D and calcium deficiency. Nine of 69 patients (13%) had secondary hyperparathyroidism due to calcium or vitamin D deficiency, or a combination of both. Mean vitamin D increased from 48.1 to 80 nM at T1 (p < .001), and remained relatively stable thereafter (Fig. 2). Vitamin D levels >50 nM were reached in 90% at T1 and in 85% at T2 of all patients treated for vitamin D deficiency. Target levels of vitamin D (≥75 nM) were reached in 59% at T1 and in 59% at T2 of all patients treated for vitamin D deficiency.
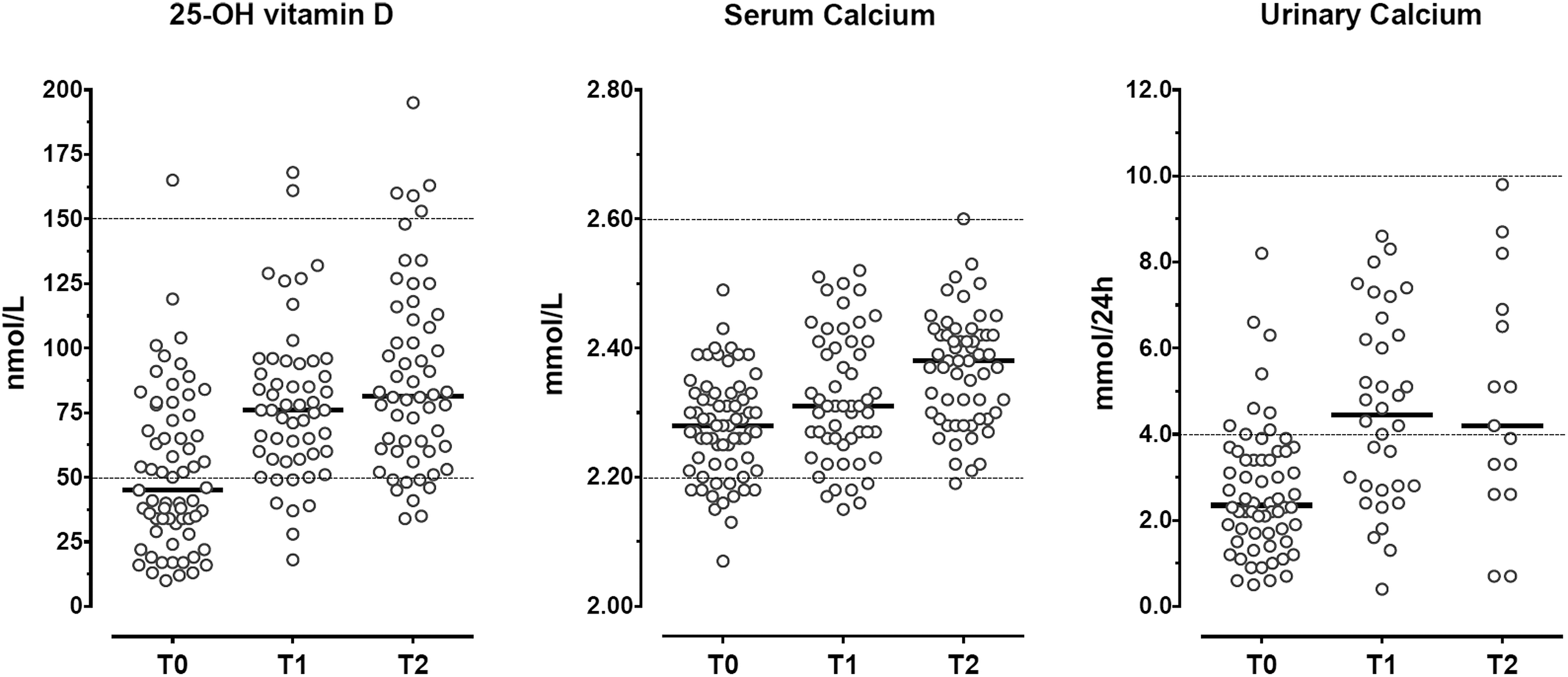
Individual vitamin D, serum calcium, and 24-h urine calcium excretion at baseline and after short-term (T1) and long-term (T2) follow-up. Each dot represents an individual patient. Bold lines represent median values.
Mean serum calcium increased gradually over the course of 70 months, from 2.28 to 2.37 mM (p < .001). Hypercalcemia was not observed (Fig. 2). Mean urinary calcium excretion increased from 2.7 to 4.6 mmol/24 h (p < .001) at T1 months and then remained rather stable with a value of 4.5 mmol/24 h at T2 (p = .4). Target levels of urinary calcium (>4 mM/24 h) were reached in 57% at T1 and in 44% at T2 of all patients treated for calcium deficiency. Mean serum PTH levels decreased from 5.4 to 4.1 (mean difference 1.3 pM, 95% CI: 0.01–2.6 pM, p < .05) at T1 and by another 2.3 pM (95% CI −0.8 to 5.5, p = 0.09) at T2.
Change in BMD at T1
Lumbar spine BMD increased significantly by 2.0% (95% CI 0.7%–3%, p < .05), right BMD increased by 0.5% (95% CI −0.3% to 1.2%, p = .2), and left hip BMD increased by 1.0% (95% CI 0.2%–1.7%, p < .05), respectively (Table 2). The expected rates of change were −0.2% for the lumbar spine and −0.5% for left and right hip. The relative increases in BMD compared with the expected changes are therefore 2.2% (95% CI 0.9%–3.4%) for the lumbar spine, 1.1% (95% CI 0.3%–1.8%) for the right hip, and 1.5% (95% CI 0.9%–2.3%) for the left hip (p < .05 for all comparisons).
Measured Versus Expected Change in Bone Mineral Density at Different Anatomical Sites, After 15 (T1) and 70 Months (T2)
Results are expressed as mean value ± SEM.
BMD, bone mineral density.
Rate of change in BMD at T2
Lumbar spine BMD increased only slightly from +2.0% to +2.3% between T1 and T2 (Table 2). As the expected rate of change in lumbar spine BMD over the 70-month period was −0.7%, the difference between the measured and the expected rate of change rose to +3.0% (95% CI 1.2% −4.8%, p < .05). Both hip BMDs started to decrease after T1, and after 70 months the decline had become greater than the increase observed during the first 15 months of treatment. The measured rate of change after total follow-up was −0.6% for both the right and left hip BMDs, whereas the expected rate of change over this period was −1.5%. The positive difference between the measured and the expected rate of change did not reach statistical significance (0.9%; 95% CI −0.6% to 2.3%, p = .24).
Switching in cART regimens
At baseline, 82% of the patients received tenofovir disoproxil fumarate (TDF)-containing cART and 33% used PIs. In our population, TDF or PI was switched to a non-TDF/PI regimen in 20/69 patients (29%). Six (9%) patients switched between T0 and T1, whereas the remaining 14 patients switched between T1 and T2. No association was found between the discontinuation of TDF or PIs and changes in BMD.
Discussion
This retrospective cohort study performed in a real-life outpatient setting shows that structured vitamin D and/or calcium supplementation in HIV+ patients delays the long-term decrease in the hip BMD and increases BMD in the lumbar spine during 70 months of follow-up. The main increase in BMD occurred in the first year of vitamin D and/or calcium supplementation, in particular for the lumbar spine. Lumbar BMD increased by 2% after 15 months, with a further increase to a total of 2.3% after 70 months. Right and left hip BMDs increased slightly after 15 months (0.5% and 1.0%, respectively) and then declined slightly to a net change of −0.6% over 70 months.
The relatively large improvement in BMD during the first 15 months is most likely due to the treatment of vitamin D deficiency-related osteomalacia. Long-term continuation of supplementation after this period serves to maintain the improved vitamin D and/or calcium status and slow the decrease in BMD in the years to follow. The improvement of BMD is not likely attributed to an improvement of immunity status of the HIV+ patients over the years, because 94% of patients at baseline were adequately treated with CD4 T cell counts larger than 200/mm3.
The prevalence of vitamin D deficiency in our Dutch cohort at baseline was 46%. This is in agreement with previous studies in HIV+ patients. 27 The prevalence of calcium deficiency in HIV+ patients has not been investigated previously. In our population, it was as high as 43%, a figure that is 15%–25% higher than that observed in hospitalized patients. 40 Secondary hyperparathyroidism attributed to calcium or vitamin D deficiency was present in 13% of patients. The prevalence of osteopenia (40.0%) and osteoporosis (8.4%) in our cohort was comparable with numbers reported in previous studies. 8 –10 These similarities in baseline BMD findings compared with other cohorts suggest that the results of treatment achieved in the present study may also apply to other HIV+ populations.
Vitamin D supplementation in HIV+ patients has been investigated previously, however, these studies 41 –43 only assessed short-term efficacy (up to a maximum of 2 years) and most studies only assessed the effect of vitamin D supplementation on serum vitamin D levels, without reporting changes in BMD. The vitamin D-deficient patients in the study by Benguella et al. 41 received a loading dose of 100,000 IU cholecalciferol twice monthly for 4–8 weeks, followed by at least four doses of 100,000 IU per year for 2 years, whereas Noe et al. 42 prescribed 20,000 IU cholecalciferol weekly, without a loading dose, and Lerma-Chippirraz 43 used a cholecalciferol regimen of 16,000 IU weekly. In these studies, target levels of >50 nM were reached in 78% and 82% after one and 2 years of supplementation, respectively. 42,43 Target levels of >75 nM were reached in 42% and 53% after one and 2 years of treatment, respectively. 42,43
In comparison, we reached target levels of >50 nM in 90% of treated patients and levels of >75 nM in 59% of treated patients (Fig. 2). The vitamin D regimen we used raised and maintained vitamin D levels above 50 mM in 90% at 15 months and this percentage declined only slightly to 85% after long-term follow-up, suggesting high compliance. Calcium supplementation was less successful. Target levels of urinary calcium (>4 mM/24 h) were reached in only 57% at T1 and in 44% at T2 of all patients treated for calcium deficiency. Poor compliance to calcium supplementation appears to be a major issue.
The difference in response between lumbar spine and hip BMD was considerable. This may be related to differences in bone architecture. Lumbar vertebrae mostly consist of trabecular bone, whereas the hip is mainly cortical bone. 44 Trabecular bone has a higher turnover and a shorter response rate to disease as well as treatment. 45 Another explanation might be that the increase in lumbar bone density is overestimated due to overlying sclerosis of lumbar vertebrae or aortic sclerosis. 46,47 However, this is an unlikely explanation as the prevalence of sclerosis of vertebrae and aorta primarily increases with age in the elderly. 48 Our patients were relatively young with their mean age of 43 years.
Switching off TDF or PIs can lead to an improvement in BMD. 49,50 However, it is unlikely that the small group of (early) switchers contributed significantly to the increase in BMD at T1, that is, the period that the main improvement in BMD was observed. In addition, no association was found between switching and long-term bone density changes. Patients who switched off TDF or PIs did not have more favorable changes in BMD than patients who did not switch or were not on TDF or PIs at the start.
Strengths and limitations
The strengths of this study are the long-term follow-up with multiple DEXA scans and laboratory measurements, and the correction for the duration of cART use. Furthermore, it provides insight to the actual efficacy of vitamin D and/or calcium supplementation of a real-life HIV+ population, instead of a strictly controlled research population, where compliance to treatment might be higher due to intensive monitoring. However, this study also has some limitations: it lacks a parallel control group not receiving calcium and/or vitamin D supplementation for its deficiencies. Instead, we used a control group derived from previously reported studies, with data correction for duration of cART use, to put our results into perspective by describing the natural course of bone density changes in HIV+ patients on cART. Such a control group has its limitations. It does not account for differences in cART regimens and DEXA machines. However, the possible bias thus introduced is considered to be small since the baseline characteristics and the use of TDF and PIs in most reference studies were quite similar to that in ours, and differences between DEXA machines were reduced by expressing results in percentage change per year instead of g/cm2. However, the use of concomitant medication affecting BMD (e.g., bisphosphonates, testosterone, corticosteroids, and anticonvulsant) was not always described in the reference studies, and in some studies the results may have been affected by these type of drugs. For example, in the study by Grant et al., 7 of 97 patients had used a BMD improving drug (e.g., bisphosphonates), whereas 14 of 97 patients had used a drug with a negative impact on BMD (e.g., corticosteroids). 16 Finally, the number of missing values of urinary calcium excretion was high, which limits the strength of our findings on calcium balance, and the number of patients was too small to evaluate the impact of the different cART regimens on bone health status at baseline and their responsiveness to vitamin D and calcium supplementation.
Implications for future research and clinical impact
This study confirms that vitamin D and calcium deficiency as well as osteopenia and osteoporosis are highly prevalent in HIV+ patients, and it has shown that long-term correction of vitamin D and calcium deficiencies improves lumbar spine BMD and tends to attenuate the cART-related decrease in hip BMD. We recommend that screening of calcium and vitamin D status, as well as BMD, should be considered to become part of regular care.
Footnotes
Acknowledgment
We thank Lian Roovers for her assistance with statistical issues.
Author Disclosure Statement
All authors declare no conflict of interest.
Funding Information
No funding was received for this article.
Supplementary Material
Supplementary Table S1
Supplementary Table S2
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.