
Abstract
HIV and hepatitis C virus (HCV) coinfection is associated with poor health outcomes. This study was designed to assess risk factors for and mortality with coinfection before direct-acting antiviral treatment availability in a state with an evolving opioid epidemic. HCV infection was determined from review of the medical record at two clinics serving the majority of people living with HIV (PLWH) in care in Middle Tennessee from 2004 to 2013. Association of potential risk factors with HCV-positivity was assessed using logistic regression. Association of HCV-positivity with mortality was assessed with a Cox proportional hazards model, adjusting for selected covariates. A total of 3,501 patients were included: 24% female; 51% men who have sex with men; 47% white; 44% African American/black; median age of 38 at their first visit; median most recent CD4 count 502 cells/μL (301–716); and HIV viral load 47 copies/mL (39–605); followed for a median of 3.0 (1–5) years. Prevalence of HCV was 13%. Those with a history of injection drug use (IDU) demonstrated the highest odds of HCV-positivity [odds ratio 12.94; 95% confidence interval (CI) 9.39–17.83]. There were 305 deaths; median age at death was 47 years (40–53). HCV coinfection was associated with greater mortality (hazard ratio 1.61; 95% CI 1.20–2.17; p < .001). Among PLWH, HCV coinfection was associated with IDU and an independent predictor of mortality. These results affirm the importance of HCV coinfection and inform interventions targeting the continuum of HCV care, uptake of HCV treatment, and the impact of drug use in this population.
Introduction
Hepatitis C virus (HCV) was estimated to infect 3.5 million persons in the United States in 2015. 1 The prevalence of HCV infection in the southeastern United States is unclear, due, in part, to lack of reporting from several states. 2 Tennessee, Kentucky, and West Virginia reported rates of infection per 100,000 population at least twice the national rate in 2016, at 2.3, 2.3, and 5.1 times the national rate, respectively. 3
From 2005 to 2014, the incidence of HCV infection in Tennessee increased nearly fivefold, in parallel with a growing opioid abuse and intravenous substance use crisis. 4 –7 A corresponding increase in HCV prevalence in Tennessee was observed even before augmentation of chronic HCV surveillance efforts by the state Department of Health in 2015, with an increase from 4,016 to 6,806 being reported confirmed and probable cases between 2013 and 2014. 8 In June 2016, the CDC released a list of 220 counties deemed at high risk of HIV and hepatitis C epidemics, based on factors including pharmacy sales of prescription painkillers, overdose deaths, and unemployment—possible indirect indicators of the prevalence of intravenous drug use. 9 Forty-one of the 220 high-risk counties are in Tennessee.
In December 2017, a state-level assessment of the counties in Tennessee analyzing opioid use rates and other data confirmed numerous counties at high risk for increases in incidence of HIV and/or HCV infection. 10 The present analysis includes data from clinics in Davidson County, Tennessee, one of two counties in the state with an overlap of higher range reported numbers of acute HCV and newly diagnosed HIV cases in 2015. 8 In particular, numbers of heroin-related arrests and seizures are rising in counties encompassing urban areas such as Nashville, the metropolitan center of Davidson County. 11
While newer direct-acting antiviral (DAA) agents for HCV are highly effective and HCV cure is now the expected outcome of treatment, drug costs, comorbidities, and challenges in testing those at high risk for contracting HCV make universal treatment infeasible at present. 12 Thus, understanding factors associated with HCV infection and mortality in those with HCV remains important. This is especially true in persons coinfected with HIV and HCV, for whom lower rates of spontaneous clearance and increased mortality are recognized disparities. 13,14
This study was designed to assess risk for and mortality with coinfection before DAA treatment availability in a state with an evolving opioid epidemic. Evidence of higher mortality in HIV-positive patients diagnosed with HCV in Middle Tennessee could impact the management of HIV/HCV coinfected patients in the region, and a better understanding of risk factors for HIV/HCV coinfection can guide the policy for frequency of screening for HCV. We hypothesized that sociodemographic factors would be associated with risk of and mortality in HIV-HCV coinfection and that coinfection would be associated with mortality in this population.
We analyzed the association of a priori selected risk factors that have been associated with HCV risk in other populations with HCV coinfection 15 –18 and difference in mortality with and without HCV coinfection in people living with HIV (PLWH) from two clinics in Middle Tennessee, which provided HIV care for 90% of HIV-positive persons in Davidson County. 19
Methods
Study design
We conducted a retrospective observational cohort study to analyze the association between preselected variables and HCV-positivity and all-cause mortality in PLWH with and without HCV coinfection during the period of 2004–2013. The study population included the two largest outpatient HIV clinics in the Nashville metropolitan area: Meharry Community Wellness Center (MCWC) and Vanderbilt Comprehensive Care Clinic (VCCC). Data were from PLWH whose first visit to one of the clinics occurred between 2004 and 2013, aged 18 years or older at their first visit, and with nonmissing HCV status. Persons who self-reported as transgender were excluded from the analysis. Vanderbilt and Meharry Institutional Review Boards approved the analysis using deidentified data, with waiver of informed consent.
Data collection
We extracted patient health data from electronic medical records at both clinics and performed quality checks for data completion and validation at both sites. HCV status was determined by automated and manual electronic chart review for free text diagnoses or diagnostic codes indicating HCV infection (Table 1).
Diagnoses Used for Determination of Hepatitis C Virus Coinfection
HCV, hepatitis C virus.
Statistical analyses
Demographic and clinical characteristics were summarized by HCV status using median [interquartile range (IQR)] or percent (frequency), as appropriate. Univariate and multivariable logistic regression models were used to investigate the association of HCV status with a priori selected potential risk factors. Multivariable models were fit using both complete case analysis and multiple imputation using predictive mean matching. 20
These risk factors included age [categorized as 18–24: reference variable/value (Ref.), 25–44, 45–64, 65+], sex [female (Ref.), male], race/ethnicity [non-Hispanic white (Ref.), black or African American, Hispanic/other (including Asian, Middle Eastern, mixed race/ethnicity, American Indian/Eskimo Pacific Islander, and undefined race/ethnicity)], HIV risk factors [heterosexual (Ref.), men who have sex with men (MSM), injection drug use (IDU) including MSM/IDU, other (i.e., transfusion, tattoo, vertical transmission, accidental needle stick, unidentified)], first CD4 cell count and plasma HIV-1 RNA (viral load) in care, and site (MCWC, VCCC, both). Those with undefined race were included with the “Other” group. CD4 count and viral load were fit with restricted cubic splines (three knots) to relax the linearity assumptions.
The association of mortality with HCV status was assessed using Kaplan–Meier curves, log rank tests, and univariate and multivariable (complete case and imputed) Cox proportional hazard models, stratified by site. Covariates included were similar to those used in the logistic regression model (sex, race/ethnicity, HIV risk factor, age, CD4 cell count, and viral load) except that first CD4 cell count and plasma HIV viral load were replaced with last measured values. A sensitivity analysis was also done in which first CD4 count and HIV-1 RNA, while in care, were used in place of the last recorded values. Missing data were multiply imputed using 10 imputation replications. All statistical analyses were performed using R, version 3.4.2 (
Results
Descriptive statistics
Of 3,637 identified patients in care between 2004 and 2013, 2 were excluded because they were younger than 18 years at their first clinic visit, 11 were excluded because they reported to be transgender, 121 were excluded because of missing or unknown HCV status, and 2 were excluded due to unresolved discrepancies in race.
A total of 3,501 subjects met the inclusion criteria, of whom 13% were HCV-positive. The cohort population was primarily male (76%) and MSM (51%), with similar proportions of white, non-Hispanic (47%), and black/African American (44%) race/ethnicity. Median (IQR) first and last absolute CD4 counts in care were 374 (208–572) and 502 (301–716) cells/mm3, respectively; median (IQR) first and last HIV-1 RNA measurements in care were 2,744 (112–34,725) and 47 (39–605) copies/mL, respectively. Median (IQR) follow-up time was 3.0 (1.0–5.0) years. During follow-up, 305 persons (8.7%) died with a median (IQR) age at death of 47 (40–53) (Table 2).
Descriptive Statistics by Hepatitis C Status
Data presented are % (N) or 25th percentile, median, and 75th percentile for categorical or continuous variable, respectively. “Other” race/ethnicity classification includes Asian, Middle Eastern, mixed race/ethnicity, American Indian/Eskimo Pacific Islander, and undefined race/ethnicity. “Other” risk factor classification includes transfusion, tattoo, vertical transmission, accidental needle stick, and patients with no risk factor identified.
Tests used: aPearson test; bWilcoxon test.
IDU, injection drug use; MCWC, Meharry Community Wellness Center; MSM, men who have sex with men; N, number of nonmissing values; VCCC, Vanderbilt Comprehensive Care Clinic.
Baseline variables and HCV status
HCV coinfection was significantly associated with IDU, which included MSM/IDU [odds ratio (OR) 12.94; 9.39–17.83, Table 3] as well as increased age, with the 45–64 group having the highest odds of HCV-positivity when compared with the 18–24 group (OR 7.45; 2.94–18.91, Table 3). Male sex was not significantly associated with coinfection.
Results from the Logistic Regression Model Investigating the Association of Hepatitis C Status with A Priori Selected Potential Risk Factors
Reference variable/value is abbreviated as (Ref.). “Other” race/ethnicity classification includes Asian, Middle Eastern, mixed race/ethnicity, American Indian/Eskimo Pacific Islander, and undefined race/ethnicity. “Other” risk factor classification includes transfusion, tattoo, vertical transmission, accidental needle stick, and patients with no risk factor identified. CD4 count and HIV-1 RNA (viral load) level were fit with restricted cubic splines (three knots) to relax the linearity assumptions.
CI, confidence interval; OR, odds ratio.
HCV coinfection and mortality
Coinfected patients had lower survival, with survival probability at 3 years of 0.87 versus 0.94 (Fig. 1, log rank p < .001). In imputed multivariable analysis, those with HCV coinfection, increased age, and lower last CD4 had higher hazards of mortality [adjusted hazard ratio (HR) 1.61; 95% confidence interval (CI) 1.20–2.17 for HCV coinfection, Table 4]. Patients of Hispanic or “other” (including those undetermined) race/ethnicity had reduced hazards of mortality (HR 0.46; 95% CI 0.26–0.81). Results from the sensitivity analysis in which first absolute CD4 count and HIV-1 RNA replaced last measurements were similar with the exception that viral load was no longer a significant predictor of mortality.
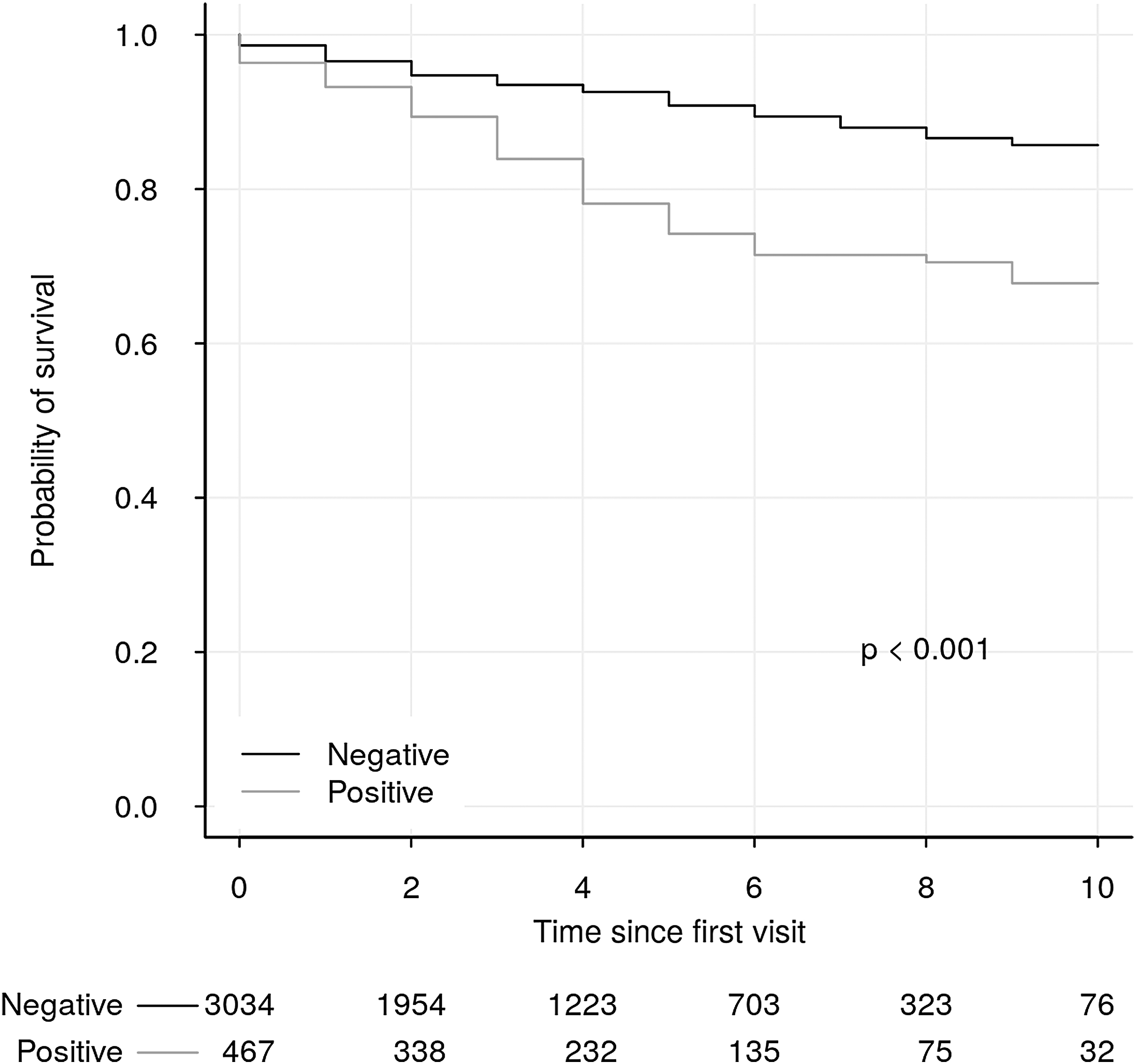
Kaplan–Meier curve for survival by HCV status at time in years since first visit. HCV, hepatitis C virus.
Results from the Cox Proportional Hazard Models Investigating the Association of Hepatitis C Status with Mortality
Test for proportional hazards: p = .005 for the complete case adjusted analysis and p = .007 for the imputed adjusted analysis. Non-significant p-values indicate the null that the hazards are proportional could not be rejected. Viral load was the main offending variable for both the complete case and the imputed analysis. Reference variable/value is abbreviated as (Ref.). “Other” race/ethnicity classification includes Asian, Middle Eastern, mixed race/ethnicity, American Indian/Eskimo Pacific Islander, and undefined race/ethnicity. “Other” risk factor classification includes transfusion, tattoo, vertical transmission, accidental needle stick, and patients with no risk factor identified. CD4 count and HIV-1 RNA (viral load) level were fit with restricted cubic splines (three knots) to relax the linearity assumptions.
HR, hazard ratio.
Discussion
In this cohort of PLWH in the pre-DAA era, we observed significant associations with HCV coinfection for those with reported HIV risk factor of IDU, which included MSM/IDU combined, and for those older than 24 years. This association was not limited to persons born between 1945 and 1965. Our data did not show male sex to be significantly associated with risk for HCV coinfection. We observed higher all-cause mortality among persons with HIV/HCV coinfection compared with those with HIV alone. Contemporary international and national multicenter cohort studies report increased mortality with HIV/HCV coinfection. 21 –25
Lower mortality observed in Hispanic and other ethnicity groups may represent an artifact of a small sample size and “false association.” However, it is also possible that in these clinic cohorts, persons from Hispanic and other minority race/ethnicity populations who are able to engage in care to meet eligibility criteria (at least two clinic visits) may have language skills and socioeconomic status to be able to maintain better overall health compared with others with these demographics. Future studies with larger sample sizes of persons of Hispanic and other minority race/ethnic origin could explore these differences.
Our study is among the largest analyzing HCV/HIV coinfection risk factors and mortality within a single metropolitan area in the southeastern United States, a region that may be at the intersection of risk for increases in both HIV and HCV infections. In an analysis of PLWH extending into the early DAA era, Breskin et al. report a similar risk association with HIV/HCV coinfection, as well as a 10-year risk difference for all-cause mortality of −3.8% if all PLWH in the study were to be treated with DAA versus none. 22
Our study has several limitations common to observational studies, including potential unmeasured confounders of HCV coinfection and mortality. We included several important factors in our adjusted models, but not all data were available across the different clinic cohorts. Our analysis cannot address the impact of HCV in the DAA era, nor does it address HCV-related morbidity or cause-specific mortality. The observational nature of the data also limits our ability to draw conclusions regarding causal relationships.
Conclusions
Results of our study support the finding that all-cause mortality without DAA treatment occurs earlier for PLWH and HCV coinfection, provide needed estimates for mortality in a diverse and vulnerable southeastern U.S. population, and highlight potential risk factors for HIV/HCV coinfection, which may differ from the general population. Investigation of the association of coinfection with mortality in this specific setting, a southern U.S. metropolitan center with potential for opioid, hepatitis C, and HIV epidemics, was pursued in hopes that outcomes might drive state and regional efforts to institute additional programs for harm reduction and opiate replacement therapy and especially syringe services programs. Syringe services programs remain illegal by federal law, regardless of HIV or viral hepatitis status, despite the potential for reduction of spread of these deadly infections. 26 –28
Additional analyses of concomitant HIV and HCV epidemics using data from heightened surveillance and reporting for chronic HCV, along with augmented screening for HCV and drug use, are needed to inform policy makers and insurers, expand access to DAA and harm reduction, and improve the continuum of hepatitis C care for PLWH.
Footnotes
Acknowledgments
The authors thank the clinic patients and staff. They thank Joanna Shaw-KaiKai, MD, for contributions to posters and early abstracts and Zudi Takizala for administrative support and submission assistance.
Authors' Contributions
T. Hall wrote the article. C.A.J. performed analyses and wrote the article. S.F. performed institutional review board/regulatory tasks, data harmonization between VCCC and MCWC sources, and VCCC data validation. M.T. performed chart review for VUMC. S.P. and M.T. participated in the overall data analysis. T. Hulgan, T.R.S., and V.B. participated in the study design and wrote the article. V.B. also performed chart review for MCWC. All authors reviewed and approved the final version of the article.
Author Disclosure Statement
No competing financial interests exist.
Funding Information
This work was funded, in part, by the National Institutes of Health (NIH)-funded Tennessee Center for AIDS Research (P30 AI110527) and by NIH grant MD007586.