
Abstract
Analytical treatment interruptions (ATIs) aim to assess effects of HIV cure-focused interventions, but poses potential risks. Understanding of ATI acceptability among people living with HIV (PLHIV) and their HIV health care providers (HHP) is limited. Two international online surveys for PLHIV and HHP assessed understanding and acceptability of monitoring strategies during ATI. Survey items included the following: frequency of CD4, viral load (VL) and clinical assessment, CD4 and VL threshold to restart antiretroviral therapy (ART), acceptability of detectable viremia during ATI, and potential risks of ATI. Responses were collected from July 2017 to January 2018, and a descriptive analysis was performed. Responses to questions asked in both surveys were compared by χ2 test. Four hundred forty-two completed the PLHIV survey: 22% identified as female, 39% older than 50 years of age, and 64% identified as gay/homosexual/lesbian. Ninety-five percent were on ART, of which 83% reported an undetectable VL. The preferred frequency of CD4, VL, and clinical monitoring during ATI was monthly. Thirty-five percent of respondents preferred VL to remain undetectable during ATI and would not accept any sustained period of viremia, compared to 18% of 144 HHP (p < .01). Having previously interrupted ART predicted preference for VL to remain undetectable during ATI (odds ratio 0.6, p = .05). Both clinicians and PLHIV were concerned about HIV transmission during ATI. Our work demonstrates that PLHIV expectations of ATI in cure-focused clinical trials do not align with current practices, with PLHIV less accepting of viremia during ATI and preferring less frequent monitoring. Clear education messages and careful consent processes need to be developed in relationship to ATIs in HIV cure research.
Introduction
Antiretroviral therapy (ART) has dramatically reduced morbidity and mortality of people living with HIV (PLHIV), but HIV cannot be cured, and life-long treatment is required. 1 Scientific and community interest in eliminating HIV has increased over the last decade. The main barrier to achieving a cure is HIV latency, defined as the long-term persistence of virus in resting T cells. 2 In the absence of ART, latent HIV can reactivate leading to virus replication, decline in the immune system, and poor clinical outcomes. 3 Analytical treatment interruptions (ATIs) are structured and temporary cessations of ART, performed in the context of HIV cure clinical trials. They are used to assess the effects of interventions aimed at achieving HIV remission or virological control in the absence of ART.
After cessation of ART, viral load (VL) set point and time to viral rebound are important outcomes to test the efficacy of interventions in cure trials and are increasingly reported. Prolonged treatment interruptions have been reported to increase the risk of serious opportunistic infections and all-cause mortality 3 most notably demonstrated in The Strategies for Management of Antiretroviral Therapy (SMART) study. 4 More recent studies, however, suggest that closely monitored, short-term ATI is safe, and does not affect the size of the HIV reservoir. 5 –7 Significant heterogeneity in ATI study design has led to the development of consensus recommendations for future trial protocols involving ATI. 3,8
The increased frequency of ATI trials coexists with all major HIV treatment guidelines recommending continuous ART for all people with HIV. 9,10 Considering the significant ethical and clinical challenges 11 to incorporating ATI into trials for both PLHIV and their HIV health care providers (HHP), there is a critical need to gain a more detailed description of participant and provider understanding of ATI. The aims of this study were to assess PLHIV and HHP for acceptability of monitoring strategies (including frequency of monitoring, threshold to restart ART and duration of ATI), and perceived risks in enrolling in cure-focused clinical trials. This will help researchers to meet the expectations of participants and their clinicians in these studies and assist in designing trials and informed consent processes to match these expectations.
Materials and Methods
Two international online surveys (Supplementary Data) were designed—one for PLHIV (38 questions) and one for HHP (16 questions). Information was collected on self-reported demographics (PLHIV: country of residence, gender, age, sexuality, country of residence, years on ART, HIV VL, and CD4 count; HHP: country and type of practice, number of patients treated for HIV), as well as previous experience with any interruption of ART. The PLHIV survey assessed the acceptability of different monitoring strategies during ATI, including frequency of CD4, VL, and clinical assessment; CD4 and VL threshold to restart ART, and how long participants would be comfortable off ART (duration of ATI). The HHP survey assessed how long clinicians would be accepting of interruption of ART in a clinical trial, as well as minimum CD4 parameters within the trial. Both surveys addressed the potential risks of ATI, including HIV transmission to a negative partner, decline in general health, risk of opportunistic infections, and development of resistant virus. The sample of surveyed PLHIV and HHP were not linked in any way.
The surveys were designed and hosted on an online platform, Qualtrics™, and accessed via a link from
Analysis
Participant responses to both surveys were reported as proportions for categorical variables and median and interquartile ranges for continuous variables. Responses to questions that were asked of both PLHIV and HHP were compared by χ2 test. Uni- and multivariate logistic regression for a preference for HIV VL to remain undetectable during ATI estimated odds ratios (ORs) for different predictor variables. These were age, gender, sexuality, years since HIV diagnosis, CD4 count, tertiary education, country of residence (high- vs. low-/middle-income country as per World Bank country classification), and having ever interrupted ART. Variables with p < .2 in univariate analyses were entered into the multivariate model. Variables not reaching statistical significance (p < .05) were deleted from the model. Age and gender were considered as potential confounders and retained in the final multivariate models. Validation of goodness-of-fit was via the Pearson goodness of fit test, with a value of p > .05 indicating an appropriate fit. All analyses were conducted using STATA v15 (StataCorp, College Station, TX).
Results
PLHIV survey
The PLHIV survey was completed by 442 participants. All except 2 of the 38 questions were answered by at least 80% of respondents. All 38 questions were answered by 345 (78%) respondents. Respondent characteristics are summarized in Table 1. Seventy-five (22%) respondents were female and 137 (39%) were older than 50 years of age. Two hundred twenty-two (64%) respondents identified as gay, lesbian, or homosexual. The majority of participants, 272 (80%), resided in high- or middle-income countries such as North America (27%), Europe (28%), and Australasia (20%), with 274 (80%) living in urban or metropolitan areas. Three hundred thirty-one (95%) participants were on ART, of whom 285 (83%) reported an undetectable VL, and 245 (71%) reported having a CD4 count above 500 cells/mm3. One hundred fifty-one (44%) participants were diagnosed with HIV over 10 years ago, and 116 (35%) had been taking ART for over 10 years.
Participant Characteristics
ART, antiretroviral therapy; GED, general education development; HSC, high school certificate; PLHIV, people living with HIV; TAFE, technical and further education; VL, viral load.
Frequency of monitoring
Three hundred seventy-five participants responded to questions on how frequently they would prefer to have clinical, virological, and immunological monitoring during ATI. The most common response was monthly, with 118 (31%), 132 (35%), and 147 (39%) of respondents choosing this for CD4 count, HIV VL, and clinical review, respectively (Fig. 1). Half of the respondents (187, 50%) selected the same frequency of monitoring for all three parameters. For 188 (50%), who did not select the same frequency of monitoring, 116 (62%) selected less frequent clinical review compared to VL testing, and 67 (36%) selected a less frequent CD4 count check compared to VL.
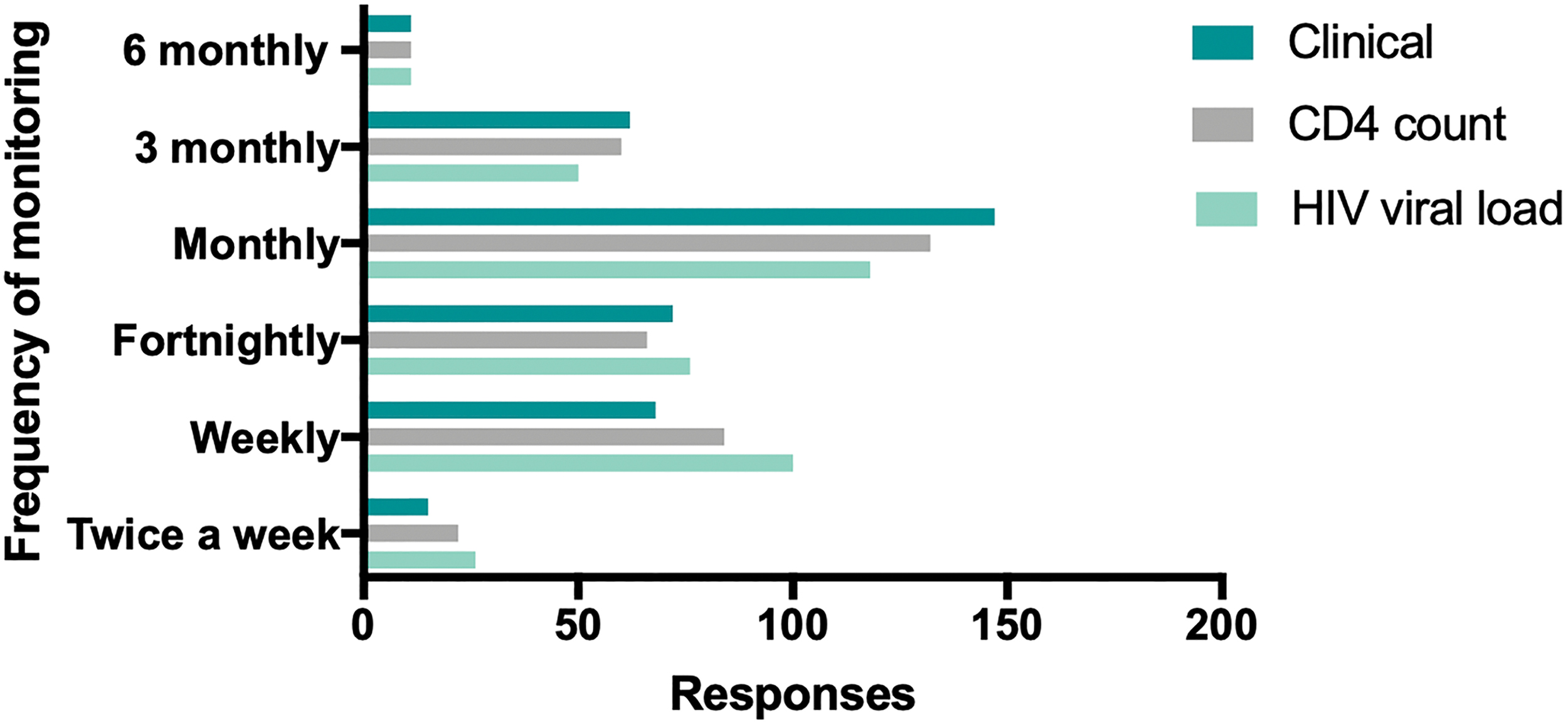
PLHIV preferred monthly monitoring for HIV VL, CD4 count, and clinical review during ATI. ATI, analytical treatment interruption; PLHIV, people living with HIV; VL, viral load. Color images are available online.
Threshold to restart ART
We asked participants what would be the preferred upper limit of HIV VL during ATI, if they remained clinically well and their CD4 count did not decline. One hundred twenty-one (34%) respondents wanted their VL to remain undetectable and would not accept any sustained period of viremia. Ninety-eight (27%) participants accepted a VL rise to 1,000 copies/mL, 58 (16%) to 5,000 copies/mL, and 84 (23%) were not concerned about how high their VL rose during ATI. In the same context, only 36 (10%) participants accepted a CD4 count below 350 cells/mm3 during ATI, with 286 (80%) wanting their CD4 count to remain above 350 cells/mm3 (Fig. 2A).

PLHIV preferred CD4 count >350 cells/mm3
ATI Duration
PLHIV were asked how long they would be prepared to remain off ART during ATI, as long as they remained clinically well and CD4 count did not drop. Results are summarized in Figure 2B. One hundred thirty-five (35%) responded that they would not allow a sustained period with detectable VL and would want their ART recommenced if their VL was detectable. Ninety-nine (25%) stated that they were not concerned about how long they remained off ART in these circumstances. Twenty-four (6%) were comfortable remaining off ART for up to 1 month, 50 (13%) for between 1–3 months, 38 (10%) for 3–6 months, and 41 (11%) for 6–12 months.
Factors affecting willingness to participate in ATI
Table 2 summarizes the factors affecting the willingness of PLHIV to participate in HIV cure trials involving ATI. Almost two-thirds of respondents (217, 59%) stated that they would be more willing to undergo ATI if home-based VL testing was available, 187 (51%) would be more willing if nurses could perform home visits, and 188 (54%) more willing if preexposure prophylaxis (PrEP) was offered for HIV negative partners. Just under half of participants (161, 44%) stated that they would be more willing to interrupt treatment if financial compensation was offered. Frequency of monitoring was not a deterrent for PLHIV to participate in a study with ATI, with 169 (45%) responding that more frequent monitoring, and 176 (48%) that less frequent monitoring, would not affect their willingness to interrupt treatment. Concern about the risk of transmitting HIV to a seronegative partner also affected participant willingness, with 155 (44%) stating that they would be less willing to interrupt treatment in these circumstances. Factors that predict preference for HIV VL to remain undetectable during ATI are presented in Table 3. In univariate analyses factors predicting preference for VL to remain undetectable are having previously interrupted ART [OR 0.6, p = .03, 95% confidence interval (CI) 0.3–0.9] and identifying as gay, homosexual, or bisexual (OR 0.5, p = .02, 95% CI 0.35–0.94). In multivariate analysis which included age, gender, sexuality, and having ever interrupted ART, having ever interrupted ART predicted preference for VL to remain undetectable (OR 0.6, p = .05, 95% CI 0.3–1). This 40% reduction in odds for preferring VL to remain undetectable suggests that people who have ever previously interrupted ART are more accepting of a detectable VL during ATI.
Factors Affecting People Living with HIV Willingness to Participate in HIV Cure Trials Involving Analytical Treatment Interruptions
PrEP, pre-exposure prophylaxis.
Uni- and Multivariate Logistic Regression Predicting Preference for HIV Viral Load to Remain Undetectable
As defined by the World Bank country classification.
CI, confidence interval; OR, odds ratio.
HHP survey
The HHP survey was completed by 144 people, as summarized in Table 1. Most respondents (137, 95%) answered all questions. The majority of respondents practiced in Australia (101, 72%) and worked in tertiary teaching hospitals (72, 51%).
Twenty-four (18%) HHP respondents were uncomfortable with their patients having any detectable viremia during ATI and wanted ART recommenced once HIV VL was detectable. Only 29 (21%) felt that it was acceptable for their patients to have detectable viremia for 1–3 months during ATI, 20 (15%) for 3–6 months, and 15 (11%) for 6–12 months. Thirty-seven (27%) HHP were not concerned how long their patients had detectable viremia in these circumstances, and were comfortable with their patients being off ART for however long is required to assess the trial intervention, as long as they remained well. The majority of respondents (102, 75%) felt that CD4 count should be above 500 cells/mm3 to enrol in an ATI trial, and only 9 (7%) were comfortable with a CD4 count dropping below 350 cells/mm3 during ATI, even if the patient remained well.
Responses compared between PLHIV and HHP
More PLHIV stated a preference for HIV VL to remain undetectable during ATI compared to HHP (35% vs. 18%, p < .01, Fig. 1). Both groups preferred CD4 count to remain >350 cells/mm3 during ATI (80% vs. 88% p = .04, Fig. 2). We asked both PLHIV and HHP how concerned they were about risks associated with interrupting ART. Figure 3 describes how PLHIV and HHP characterized the potential risks of ATI, including antiviral resistance, declining health, developing symptoms of HIV or opportunistic infections, and transmitting HIV to a seronegative partner. Forty-four percent of PLHIV and 42% of HHP were “very concerned” about the risk of transmitting HIV during ATI.

Perceived concerns of PLHIV
Discussion
We have surveyed PLHIV and HIV clinicians globally about their understanding, and acceptance, of interrupting ART in the context of an HIV cure clinical trial. While several studies have assessed both community and physician attitudes toward HIV cure trials, 13,14 this is the first quantitative study exploring the perceptions of both of these groups specifically toward ATI. We found a disparity between the expectations of PLHIV for ATI cure trials and the current conduct of these studies, which will be discussed in greater details below.
We explored preferences for the frequency of monitoring in trials. When asked about preferred frequency of monitoring for HIV VL, CD4 count, and clinical review, the most common response to all three scenarios was “monthly,” with over 30% of respondents choosing this option. This is out of keeping with current cure research involving ATI, where VL is being monitored weekly if not more frequently. 3 Furthermore, consensus recommendations state that VL testing should be performed weekly for the first 12 weeks of ATI. 8 Less frequent monitoring was seen in ATI studies in the SMART study era, 4 where VL was checked monthly to begin with, then less frequently. Follow-up and VL monitoring in routine HIV care is typically performed three to six monthly, but monitoring in clinical trials is much more intense. Survey responses may reflect an expectation from PLHIV that participation in a clinical trial should not involve more demanding follow-up in addition to usual standard of care.
Our survey provided insight into the acceptability of VL increases during ATI. When asked how high they would allow HIV VL to go during an ATI, 34% PLHIV stated that their VL would have to stay undetectable. The majority of recent cure research involving ATI has used a VL threshold of 1,000 copies/mL on two consecutive readings to trigger the reintroduction of ART. 3 Testing of VL is usually performed weekly, so participants are likely to be viremic for at least 2 weeks. There are findings from the literature, however, where a VL cutoff of 1,000 copies/mL for ART restart could mask important results. For example, a recent trial investigating a combination of therapeutic vaccine and romidepsin identified 5 out of 13 participants with viremic control up to 28 weeks off ART, despite having detectable viremia (up to 2,000 copies/mL) at several individual time points during the study. 15 A threshold of 1,000 copies/mL for restarting ART may also miss the identification of posttreatment control, where individuals maintain viremic control off ART without intervention. Using the Control of HIV After Antiretroviral Medication Pause (CHAMP) cohort of posttreatment controllers (PTCs) as an example, a threshold of 1,000 copies/mL to reinitiate ART, would fail to identify 45% of PTCs, as many would experience a higher peak viremia before establishing control. 16
Country of residence (high- vs. low-/middle-income country) was not associated with preference for undetectable VL during ATI; however, people who had previously interrupted ART were more likely to be accepting of viremia during ATI. In contrast to the people who preferred to have a low or undetectable VL during ATI, 23% of PLHIV responded that they were not concerned how high their VL becomes in these circumstances. These responses demonstrate considerable heterogeneity for a parameter that often represents the most important outcome in ATI clinical trials. One reason for this may be that PLHIV who have previously experienced periods off ART may be more comfortable with the prospect of rebound viremia, particularly if their previous treatment interruptions occurred without complications.
When asked how long they would be willing to have a detectable VL during ATI, 35% of PLHIV surveyed would not allow any sustained period with detectable VL. Once again, this is out of keeping with current trial methods, as no HIV cure trial to date has demonstrated a mechanism for effective viral control off ART. A rise in VL is currently an inevitable outcome of ATI, and many recent trials have been designed with a predetermined VL threshold to restart ART. It is possible that the 25% of PLHIV who responded that they were not concerned about how long they remained off ART in these circumstances understood this, or at least were reassured that they would be closely monitored in a clinical trial.
PLHIV and HHP were concerned with risks associated with ATI, in particular with the risk of transmission of HIV to seronegative partners. This survey was conducted while the message of “undetectable equals untransmittable” (U = U) was being widely endorsed and promoted. 17 Viral rebound is expected after a period of time off ART during ATI, but PrEP has not been routinely offered to seronegative partners of trial participants. 3 As a result of our survey, we recommend that provision of PrEP, or referral to appropriate PrEP services for seronegative partners of study participants should be incorporated into all ATI trial protocols. This is in keeping with recent consensus recommendations on ATI, 8 which advocated for information on PrEP and HIV testing to be given to trial participants to provide to their sexual partners. PLHIV were less accepting than HHP of a sustained period of viremia, possibly indicating that HHP had a better understanding of clinical trial design and the rigorous follow-up and monitoring required during a trial. Both groups felt that CD4 counts should remain >350 cells/mm3, reflecting learnings from previous ATI studies that demonstrated worse outcomes when CD4 counts were allowed to drop below this level. 3 This is also the CD4 count threshold to restart ART in recommendations for the conduct of ATI. 8 Our findings demonstrate clear discrepancies between current recommended ATI practices and stakeholder preferences, and highlight the importance of including broader input and feedback from PLHIV and HHP in the design of future ATI trials.
While this is the first study to assess both PLHIV and HHP preferences during ATI, it had a number of limitations. The surveys were hosted online in English, limiting participants to a convenience sample of English-speaking people who are able to use the internet. This restricts access for 34 million of the nearly 37 million PLHIV in the world who live in low- or middle-income countries, 18 where internet access is not universal and English is not the first language. As the surveys were accessed via a website focused on HIV cure, there may be a bias toward PLHIV and HHP who are already interested or involved in HIV cure research. Despite being a global survey, the majority of respondents in both the PLHIV and HHP surveys were from Western and high-income countries, but this reflects where the majority of HIV cure research is currently being conducted. 19 Greater efforts should be made in future survey work to capture the views of the global HIV epidemic.
Recommendations and considerations arising from our survey findings are summarized in Table 4. Our study found that despite interest in HIV cure-related research, there was a reluctance among PLHIV to accept a detectable VL during ATI, something that is currently necessary to evaluate HIV cure strategies. More research needs to be conducted to better understand this reluctance and the impact of factors such as fear of onward transmission, anxiety about becoming unwell, and the importance of an undetectable status. Better understanding of these factors will help target education strategies and direct conversations between researchers and potential trial participants. Furthermore, there is a need for researchers and community educators to work together to improve the translation of scientific knowledge and trial findings into understandable and digestible language. This could include the use of infographics to compliment patient information, video dialogues where the science is broken down in a discussion format, and peer education from PLHIV who have completed an ATI trial.
Recommendations and Considerations for Future Analytical Treatment Interruption Trials Resulting from the Surveys
ATI, analytical treatment interruption; PrEP, pre-exposure prophylaxis; PLHIV, people living with HIV; VL, viral load.
Conclusion
Despite community interest in HIV cure research and optimism toward a cure being achievable, there is a clear disconnect between what PLHIV expect from cure-focused clinical trials and what is currently being practiced. This is particularly pronounced in regard to monitoring and duration of ATI. We found that PLHIV were less accepting of having a detectable VL during ATI, compared to HHP. This is likely a response to the current emphasis on the benefits of an undetectable VL for preventing HIV transmission. Concerns about HIV transmission during ATI were identified by both PLHIV and HHP, but provision of PrEP to seronegative partners and home VL testing could encourage study participation. While there is enthusiasm from both the community and clinicians for participation in this type of research, clear education messages in relationship to ATIs should be developed for both PLHIV and HHP, and careful consent must be obtained from all participants enrolling in cure studies with ATI.
Footnotes
Acknowledgments
The authors thank all those who participated in the online surveys, as well as the multiple community advocacy bodies and professional organizations who helped to disseminate them. These include Living Positive Victoria, Positive Women, the National Association of People Living with HIV Australia, the Australian Federation of AIDS organizations, NAM:AIDSmap, Project Inform, the Terrence Higgins Trust, DefeatHIV, The Institute of Many, the British HIV Association, The Well Project, TREATAsia, amfAR, the Treatment Action Group,
Author Disclosure Statement
No competing financial interests exist.
Funding Information
The institution of James H. McMahon and Jillian S.Y. Lau receive funding from Gilead Sciences, ViiV Healthcare, Merck, and Shire to conduct clinical trials. Jillian S.Y. Lau has an NHMRC Postgraduate Scholarship (1151607). James H. McMahon has an NHMRC Early Career Fellowship (1111099). Sharon R. Lewin is an NHMRC Practitioner Fellow (1042654) and is supported by the National Institutes of Health Delaney AIDS Research Enterprise (UM1 AI126611-01) and the American Foundation for AIDS Research (109226-58 RGRL).
Supplementary Material
Supplementary Data
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.