
Abstract
In high-income countries, causes of death in people living with HIV (PLHIV) have changed. Three French national surveys from 2000 to 2010 showed a decrease in AIDS-related and an increase in non-AIDS-related deaths. Deaths notified in PLHIV followed between January 1, 2011 and December 31, 2015 in 1 of 13 participating hospitals northeast of Paris area were described. Risk factors for death were assessed, using a multivariable logistic regression model. Of 14,403 individuals, 295 died. Median age at death was 52 years (interquartile range = 47–60) and 77% were men. Sixty-seven individuals (23%) died from non-AIDS-defining nonviral hepatitis-related (NaNH) malignancy, 40 (14%) from AIDS, 34 (12%) from cardiovascular disease (CVD), 33 (11%) from non-AIDS infection, 21 (7%) from liver disease, and 12 (4%) from suicide. Men and women born in sub-Saharan Africa had a lower adjusted odds ratio (aOR) of dying than men having sex with men (MSM) born in France (0.70, 95% confidence interval = 0.45–1.09; and 0.45, 0.28–0.73, respectively). Risk factors for death were older age (aOR = 2.26, 1.36–3.77 for 40–49 years and 2.91, 1.75–4.84 for >50 years vs. 18–39 years), male intravenous drug users (IVDU) transmission (2.24, 1.42–3.54 vs. MSM born in France), AIDS (2.75, 2.10–3.59), antiretroviral therapy initiation in earlier periods, time since HIV diagnosis <1 year, low CD4 cell count nadir, hepatitis B virus and/or hepatitis C virus coinfection (1.69, 1.23–2.30), and psychiatric disorders (1.73, 1.27–2.38). Our study confirms the increasing frequency of non-AIDS-related deaths, mainly NaNH malignancies and CVD, in PLHIV, justifying overall and in some specific populations (psychiatric and IVDU) prevention and screening.
Introduction
Antiretroviral therapy (ART) has dramatically reduced mortality in people living with HIV (PLHIV). 1 Although mortality rates in many nonintravenous drug users (IVDU) HIV-infected individuals with restored CD4 cell count on ART are similar to those of the general population, 2 overall mortality remains higher than in the general population, 1 –4 partly because of late diagnosis and/or late treatment initiation. Premature aging of PLHIV has been raised because age-related comorbidities, such as cardiovascular diseases (CVDs), non-AIDS-defining infectious and noninfectious cancers, 5 osteoporosis, liver disease, and renal disease, are more frequent and occur at younger age in PLHIV compared with the general population. 6,7
Three successive French national surveys in 2000, 2005, and 2010 showed a decrease in AIDS-related diseases and an increase in non-AIDS-defining nonviral hepatitis-related (NaNH) malignancies and CVDs as causes of death in PLHIV. 1,8,9 Apart from the French West Indies, Paris area is the region in France with the highest prevalence and incidence of HIV. 10 We studied mortality and causes of death in PLHIV followed during the 5 years after the last national survey in 13 hospitals in the north and east of Paris area participating to the Nadis® Cohort.
Materials and Methods
Nadis® (Fedialis Medica, Marly le Roi, France) is an electronic medical record for HIV-, hepatitis B virus (HBV)-, or hepatitis C virus (HCV)-infected adults seeking care in French public hospitals 11 and is at present implemented in >30 clinical units all over France. 12 All individual data are recorded with no time delay in a structured database, allowing use of the database for clinical, epidemiological, or therapeutic studies.
The Cohort received approval from the French “Comité consultatif sur le traitement de l'information en matière de recherche dans le domaine de la santé” (registration number 15.196) and is registered with identifier NCT02898987 in
We studied mortality and causes of deaths of HIV-infected adults followed (with at least one visit between January 1, 2011 and December 31, 2015) in 1 of the 13 hospitals in the northeast of Paris area taking part in the study. The patients could be on ART (in most cases) or not. Hospitals reported all deaths that occurred during the study period either in their hospital, in another institution, or at home. HIV specialists filled in a standardized questionnaire to complete the main cause of death from the individuals' medical records when the cause was not recorded in the database. Epidemiological, clinical, and immunovirological data and treatment were retrieved from the Nadis® database.
We used the algorithm used in the last French mortality survey, “Mortalité 2010” to describe the causes of death. 1,8,9 This algorithm is adapted to the specificities of HIV infection 8 and allows categorization of deaths as follows: AIDS-related causes (1,993 Centers for Disease Control clinical classification), deaths related to non-AIDS-defining and nonviral hepatitis (NaNH)-related malignancies, hepatic diseases, CVDs, non-AIDS-defining infections, and suicide/violent deaths/other causes. When the only information about the circumstances of a death was its brutal occurrence, it was defined as “unexplained sudden death.” When no information was available, cause was considered as “unknown.”
Two clinicians classified each cause of death independently. Disagreements between clinicians were resolved through panel discussion with one other clinician. The percentage of included individuals that died was defined by the number of deaths divided by the number of individuals seen at least once during the study period. The distribution of the causes of death was compared with those of “Mortality 2010.” Because of high percentage of unknown causes of death, sensitivity analyses were performed, first after exclusion of data of two centers where >25% of causes of death were unknown, then after assuming that unknown causes of death of people with CD4 cell count <200/mm3 before death were AIDS.
Risk factors for death were assessed using logistic regression models. Variables considered for the analyses were sex, age, region of birth (France, sub-Saharan Africa [SSA], other), HIV transmission group, AIDS status, CD4 cell count, HIV RNA, HBV (HB surface antigen positive) and/or HCV antibody infection, psychiatric disorders (depression, and/or generalized anxiety and/or psychosis), arterial hypertension and metabolic disorders (diabetes mellitus and/or dyslipidemia with medical care), ART or not on the date of the last follow-up visit during the study period, CD4 cell count nadir, and HIV RNA zenith.
To explore differences related to region of birth, sex, and HIV transmission group, a combined 10-category variable was created: men having sex with men (MSM) originating from France (FRA MSM), nonhomosexual and non-IVDU men originating from France (FRA nonhomosexual men), non-IVDU women originating from France (FRA women), men originating from SSA (SSA men), women originating from SSA (SSA women), MSM originating from other countries (OTH MSM), nonhomosexual and non-IVDU men originating from other countries (OTH nonhomosexual men), non-IVDU women originating from other countries (OTH women), IVDU men, and IVDU women. IVDU men and women were not categorized according to their country of origin because IVDU were mainly from France (618/809, 76%), other IVDU being from other countries. Very few individuals (n = 134) originating from SSA declared having sex with men and men from SSA were not dichotomized according to their sexual HIV transmission group.
Multivariable logistic regression models were used to assess adjusted risk factors for death including all variables possibly associated with the outcome of interest in the univariable analysis (p < .15). All analyses were adjusted to the care center. Sensitivity analyses were carried out with IVDU separated according to the country of origin to verify that country of origin did not change the odds ratio (OR) of death in IVDU. Analyses were performed using R statistical package (version 3.3.2 online at
Results
Characteristics of dead HIV-infected adults in the northeast of Paris area study
Among 14,403 HIV-infected individuals followed in the northeast of Paris area between January 1, 2011 and December 31, 2015, 295 deaths (percentage of included individuals that died, 2.0%) were reported. From the 295 deaths, 77% were men, median age at death was 52 years (interquartile range [IQR] = 47–60); 42% were non-native from France. Death occurred 16 years after the diagnosis of HIV infection (IQR = 9–22), but HIV infection was diagnosed <6 months in 4% of dead patients and 3% had never been given ART. Forty-three percent of patients were heterosexual, 23% MSM, 23% IVDU, and 11% had other or no identified risk factor for HIV infection. Previous or current AIDS status was found in 58% of dead patients. CD4 cell count was 241 (IQR = 115–469) at death and HIV RNA was <50 copies/mL in 61% of cases. Twenty-eight percent of dead patients had HCV antibodies (with or without HCV RNA) and 12% had HBs antigen (with or without HBV DNA). Sixteen percent of dead patients were treated for arterial hypertension. Table 1 gives main epidemiological, biological, and therapeutic characteristics of the individuals who died in each study, “Mortalité 2010” and north and east of Paris area 2011–2015 studies.
Characteristics of HIV-Infected Adults Dying in the French “Mortalité 2010 Survey” and in the North and East of Paris Area 2011–2015 Study, According to the Underlying Causes of Death, France
ART, antiretroviral therapy; HBV, hepatitis B virus; HCV, hepatitis C virus; IQR, interquartile range; IVDU, intravenous drug users; n, number; NaNH malignancy, non-AIDS-defining nonviral hepatitis-related malignancy; NE Paris, north and east of Paris area.
Underlying causes of death
Underlying causes of deaths are described in Table 1 and Figure 1.
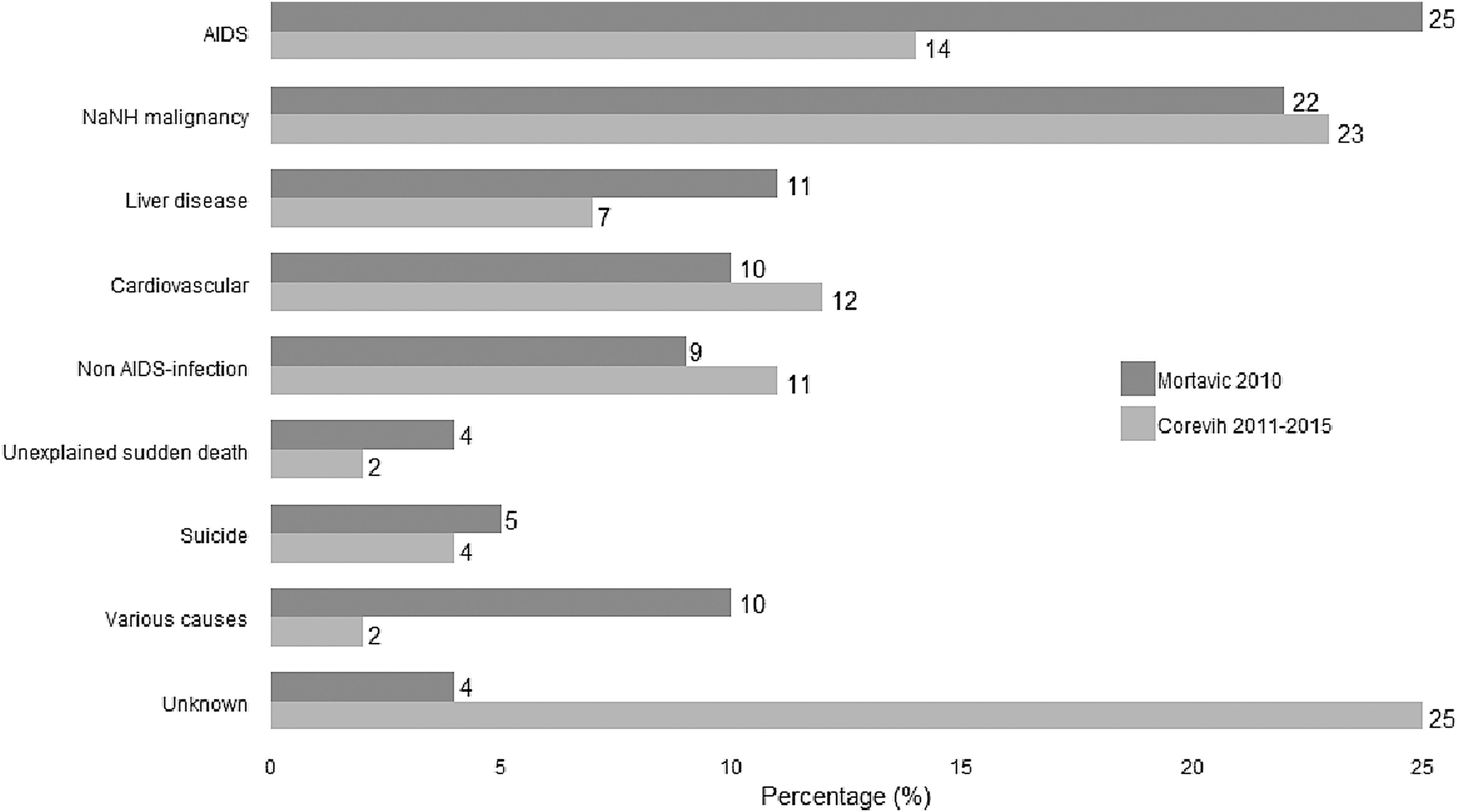
Distribution (percentages) of the underlying causes of death among HIV-infected adults, in the French mortality 2010 survey Mortavic and in Paris area 2011–2015 study. NaNH malignancy, non-AIDS-defining nonviral hepatitis-related malignancy.
The main underlying causes of death were NaNH-related malignancies (67, 23%), AIDS-related (40, 14%), CVDs (34, 12%), non-AIDS-related infections (33, 11%), liver related (21, 7%), and suicide (12, 4%). The 67 NaNH-related malignancies were mainly gastrointestinal (18, 27% of NaNH-related malignancies), bronchopulmonary (16, 24%), urogenital (12, 18%), ear–nose–throat (6, 9%), and breast malignancies (4, 6%). The 40 AIDS-related causes were mainly non-Hodgkin's lymphoma (NHL) (21, 52.5% of causes of AIDS-defining illnesses), progressive multifocal leukoencephalopathy (6, 15%) and Pneumocystis jiroveci pneumonia (6, 15%). From the 34 deaths related to CVDs, stroke was reported in 14 (41%), ischemic heart disease in 8 (23.5%), and heart failure in 8 (23.5%). More than half (18, 54%) of non-AIDS-related infections were septic shock, followed by pulmonary infections (9, 27%). From the 21 deaths related to liver diseases, 11 (52%) were caused by cirrhosis (7 associated with HCV, 3 with HBV, 1 with HCV-HBV coinfection), 8 (38%) were the result of hepatocellular carcinoma (4 associated with HCV and 4 with HBV).
Cause of death was unknown for 75 individuals (25%). Characteristics of individuals with unknown cause of death were similar to the ones of individuals with known cause of death, regarding sex, age, HIV transmission group, geographical origin, CD4+ T cell count, HIV RNA, Center for Disease Control stage, previous ART, hepatitis coinfection, psychiatric disorders, arterial hypertension, metabolic disorders (data not shown). When data from two centers with >25% of unknown causes of death were excluded (17 and 21 deaths, 53% and 67% of unknown causes of death respectively), distribution of the causes of death was unchanged: NaNH-related malignancies (64, 25%), AIDS-related (38, 15%), CVDs (31, 12%), non-AIDS-related infections (32, 12%), liver related (20, 8%), and suicide (8, 3%). When we assumed that 19 individuals with CD4 cell count <200/mm3 and unknown causes of death had died from AIDS, NaNH-related malignancies were still the first cause of death.
AIDS and non-AIDS-related infections were the leading causes of death in 105 individuals who died before 50 years (n = 19, 18% for both) (Table 1). NaNH-related malignancies, CVDs, and AIDS were the leading causes in those dying after 50 years (54, 28%, 23, 12%, and 21, 11%). Individuals who died from AIDS had been diagnosed with HIV <6 months previously in 15% of cases (vs. 3% of individuals who died of non-AIDS causes) and their infection was less frequently controlled: median CD4 cell count, 92/mL (vs. 289/mL; p < .001), plasma HIV RNA <50 copies/mL in 26% of them (vs. 67%; p < .001).
NaNH malignancy was the main cause of death whatever the country of birth; CVD was the second cause of death in individuals born in other countries. The percentages of AIDS and of non-AIDS-related infection among the different causes of death were the highest in individuals born in SSA (20% and 16% vs. 11% and 11% in people born in France and 14% and 7% in people born in other countries). The main causes of death in 69 IVDU individuals were NaNH-related malignancies (14, 20%), liver disease (9, 13%), and CVDs (7, 10%), and rates of AIDS and non-AIDS infections were low (4, 6%, and 5, 7%, respectively).
The distribution of the main causes of death differed between individuals coinfected with HIV and hepatitis B and/or C and those not coinfected (p < .001): the second cause of death in coinfected individuals was hepatic disease (20, 17%) and CVD was a less frequent cause of death (8, 7%). The main cause of death in individuals with hypertension was CVDs (12, 25%).
Risk factors for death
In univariable analysis, nonhomosexual men born in France, nonhomosexual men from other country, IVDU men and IVDU women had a higher risk of dying than MSM born in France; women born in SSA had a lower risk of dying (Table 2). In multivariable analysis, men and women born in SSA had a lower risk of dying compared with MSM born in France (adjusted odds ratio [aOR] = 0.70, 95% confidence interval [CI] = 0.45–1.09; and aOR = 0.45, 95% CI = 0.28–0.73, respectively), whereas IVDU men had a higher risk of death (aOR = 2.24, 95% CI = 1.42–3.54).
Underlying Causes of Death in HIV-Infected Adults According to Age, Country of Birth, and Hepatitis B and/or C Infection
FRA, France; OTH, other countries; SSA, sub-Saharan Africa.
Other adjusted risk factors were older ages (aOR = 2.26, 95% CI = 1.36–3.77 for people 40–49 years of age and aOR = 2.91, 95% CI = 1.75–4.84 for people ≥50 years, compared with people 18–39 years of age), AIDS status (aOR = 2.75, 95% CI = 2.10–3.59), hepatitis B and/or C (aOR = 1.69, 95% CI = 1.23–2.30), and psychiatric disorder (aOR = 1.73, 95% CI = 1.27–2.38). Higher CD4 cell count nadir, recent period of ART initiation (aOR = 0.36, 95% CI = 0.17–0.74 for the period 2010–2015 compared with the period before 1996) and time since HIV diagnosis for <1 year were associated with a lower risk of dying. (Table 3).
Characteristics of the Patients and Risk Factors for Death in the North and East of Paris Area 2011–2015 Survey, Result of the Univariable and Multivariable a Logistic Regression Models
Adjusted for the care center.
aOR, adjusted odds ratio; CI, confidence interval; cp, copies; HBs Ag, hepatitis B virus surface antigen; HCV, hepatitis C virus; MSM, men having sex with men; OR, odds ratio.
Discussion
From January 1, 2011 to December 31, 2015, the 13 centers participating in the study reported 295 deaths in 14,403 HIV-infected adults. The main underlying causes of death were NaNH malignancy, AIDS, CVDs, non-AIDS infections and liver diseases. Compared with MSM born in France, men and women born in SSA had a lower risk and IVDU men had a higher risk of dying. Other adjusted risk factors for death were older age, AIDS status, lower CD4 cell count nadir, hepatitis B and/or C infection, and psychiatric disorders.
The percentage of included individuals who died was 2.0%, corresponding to ∼0.4 per 100 patient year (PY), in accordance with rates reported in other cohort studies in western countries. 9,13,14
From 2000 to 2010, the successive French national surveys showed a decrease in the proportion of AIDS deaths from 47% to 25% and an increase in NaNH malignancy from 11% to 22%, a slight increase in cardiovascular death (7% to 10%) and in non-AIDS infections (6% to 9%), and a stable percentage of liver disease (11%). 1,8,9 Our study confirms this trend, with AIDS being now the second cause of death in our study (14%), even if our study population had twice more people born outside France (56% vs. 27%), mainly from SSA, more susceptible to some AIDS infections. 15,16
One limitation of our study is the high percentage of unknown causes. Characteristics of individuals with unknown cause of death were similar to the ones of individuals with known cause of death. We can hypothesize that there was no difference in the percentage of unknown causes of deaths according to age, region of birth, or other studied categories. In addition, because centers participating to the cohort were centers with high expertise in HIV/AIDS care, we assume that under-notification of AIDS death was unlikely.
NaNH malignancy was the leading cause of death in our study. Taking into account the AIDS-defining malignancies, hepatocellular carcinoma, and NaNH-related malignancies, malignancies represent 34% of all causes of mortality in our study, comparable with the rate in the “Mortalité 2010” survey. Indeed, if the incidence of AIDS-defining malignancies has significantly fallen in the recent years in France, 17 the rate of hepatocellular carcinoma has increased over the past decades with HBV and HCV accounting for most cases. 18 More than half of NaNH malignancies were related to smoking, either bronchopulmonary, urogenital, ear–nose–throat, and gastrointestinal, the last (esophageal and colorectal) being related to smoking. From 2005 to 2009, in France, 5-year survival did not improve after lung cancers in PLHIV, 19 justifying screening for lung cancer in this population and cancer prevention, especially smoking cessation. 20
The slight increase in cardiovascular death overtime in France was confirmed in our study where CVD represented 12% of the causes of death. 1,8,9 Percentage of liver disease was lower than in the last French national survey, despite similar rates of hepatitis B and/or C infections. 9 In individuals coinfected with HIV and HBV or HCV, liver disease was the first cause of death in “Mortalité 2010” study and the second one in our study, probably reflecting a better management of HIV and of hepatitis B or C over time, with early detection of hepatocellular carcinoma and a better access to the most recent hepatitis C treatment. This trend was recently confirmed in the ANRS CO13 HEPAVIH nationwide cohort of HIV/HCV coinfected patients, showing HCV was the first cause of mortality before 2011 and between 2011 and 2014, but was the third cause after 2014. 21
Percentages of AIDS and of non-AIDS-related infection deaths were higher in people from SSA than in other people. It has been shown that migrants from SSA, both men and women, have a higher risk of AIDS events and of non-AIDS infections compared with people born in France. 22 Immunosuppression, even when moderate, is associated with an increased risk of infection. 23 Special attention should thus be paid to the prevention of infectious diseases among migrants, including screening of vaccination status and completion of vaccine schedules, and pretravel counseling to prevent bacterial and tropical diseases.
Compared with MSM born in France, IVDU people still have a higher risk of death in the most recent period as previously shown. 24,25 In Western European countries, HIV-infected women have a higher life expectancy than HIV-infected men with same AIDS-related mortality but lower non-AIDS mortality rates. 26 Migrants from SSA have lower mortality than native people, these differences appearing mainly attributable to a lower non-AIDS mortality typically attributed to the healthy migrant effect. 27,28 We show in this study that both men and women from SSA have a lower risk of dying compared with MSM born in France despite the usual worse social determinants of the formers. 29 Other risk factors for dying were age, lower CD4 cell count nadir, previous AIDS, ART initiation in earlier periods, and hepatitis B and/or C coinfections as previously shown. 14,24,25,30 Psychiatric disorders also lead to a higher risk for death, which could be explained by a lower adherence to cART and to follow-up visits and/or more suicides. 31,32
In conclusion, our study confirms the trends of a decrease in the percentage of AIDS and liver diseases in the causes of deaths and increase in NaNH malignancy and CVDs making necessary improvement in early diagnoses by active screening and treatment of cancers and cardiovascular risk factors in an aging HIV population. People from SSA are at a lower risk of dying than people born in France, and could benefit from an improvement in prevention of infectious diseases. Particular attention is needed for care of specific populations (HIV-infected individuals with psychiatric disorders, IVDU).
Footnotes
Acknowledgments
Members of the COREVIH Ile de France Est research group: N. De Castro, J. Miantezila, J.-M. Molina (Hôpital Saint-Louis, Paris); A. Brun, G. Hamet, A. Olier (Corevih Ile-de-France Est, Paris); G. Alexandre-Castor, M. Parrinello, P. Sellier, J.-F. Bergmann (Hôpital Lariboisière, Paris); S. Diamantis, N. Vignier (Hôpital Marc Jacquet, Melun); J. Cailhol, J.-F. Michel, O. Bouchaud (Hôpital Avicenne, Bobigny); S. Abgrall (Hôpital Antoine Béclère, Clamart); F. Changama (Hôpital Jean Verdier, Bondy); M.-A. Bouldouyre (CHI Robert Ballanger, Aulnay-sous-Bois); O. Patey (Hôpital de Villeneuve-Saint-Georges); A. Chabrol (Hôpital Sud-Francilien, Corbeil-Essonne); V. Garrait, L. Richier (Centre Hospitalier Intercommunal de Créteil); V. Grégoire (Centre hospitalier de Meaux); O. Son (Hôpital de Longjumeau); H. Bideault (Hôpital de Bligny).
Author Disclosure Statement
P.S. has received travel grants from MSD and Gilead. J.-M.M. has participated in advisory boards for Gilead, Merck, Janssen, ViiV, Bristol Meyers Squibb and Teva, and his institution has received grants from Merck and Gilead. S.A. has received fees for board membership from Janssen. The remaining authors have none to declare.
Funding Information
No funding was received for this article.