
Abstract
We assessed bone mineral density (BMD) in a cohort of human immunodeficiency virus (HIV)-positive patients after a median of 11 years of combination antiretroviral therapy (cART) and evaluated the respective role of HIV infection and antiretroviral drugs (ARVs). A cross-sectional study of 162 participants (131 male) from the ANRS-C08 cohort was performed with bone dual-energy X-ray absorptiometry (DXA) scans and renal assessment. The window of exposure to ARVs was defined as an exposure of more than six cumulative months during the last 3 years before the DXA evaluation to account for a cumulative exposure that could affect bone remodeling. The association with low BMD (Z-score < −2) was assessed by a multiple logistic regression model. The study population was 50 years (median), hepatitis C virus (HCV) (18%), and hepatitis B virus (HBV) (8%) coinfection with HIV-RNA <50 c/mL in 89%, median CD4 of 619/mm3. Prevalence of low BMD was 18% in males and 6% in females. The factors associated with a Z-score < −2 in males were uric acid renal loss [adjusted odds ratio (aOR): 6.1; 95% confidence interval (CI): 1.2–31.5; p = .03], HCV coinfection (aOR: 4.0; 95% CI: 1.3–12.2; p = .02), and less frequent window of exposure to nevirapine (NVP) (aOR: 0.1; 95% CI: 0.02–0.6; p = .01). For the full study sample, there was a strong positive association between duration of exposure to NVP and lumbar spine Z-score (p = .004). HIV-positive patients exposed to long-term cART have a high incidence of low BMD. Tenofovir disoproxil fumarate and ritonavir-boosted protease inhibitors did not seem to be associated with increased risk of low BMD, whereas NVP exposure appeared to have an independent positive association.
Introduction
Human Immunodeficiency Virus (HIV) treatment has made tremendous progress in the past years leading to a major improvement in the life span of HIV-positive patients. Concerns persist on long-term adverse effects of chronic HIV infection as well as antiretroviral drugs (ARVs), including metabolic, cardiovascular, hepatic, renal, and bone complications. 1 Low bone mineral density (BMD) measured by dual-energy X-ray absorptiometry (DXA) is a common finding in HIV-positive patients, and in a literature meta-analysis, prevalence of osteoporosis, and of low BMD has been estimated to be more than three times and six times higher than in HIV-negative controls. 2 Although tenofovir disoproxil fumarate (TDF) and ritonavir-boosted protease inhibitors (PI/r) are associated with progressive bone loss, many other factors contribute to low BMD, HIV itself, low body weight, smoking, alcohol and drug abuse, and hepatitis C virus (HCV) coinfection. 3 –5 In a prospective HIV-negative matched cohort, there was a significant positive association between current use of nevirapine (NVP) and BMD. 6 To provide further knowledge on low BMD prevalence and associated factors in long-term treated HIV-positive patients, and to assess the impact of the different ARVs, we performed a cross-sectional analysis of BMD status among volunteer patients from the ANRS-C08 cohort after 10 years of follow-up under combination antiretroviral therapy (cART). 7
Patients and Methods
Study population of ANRS-CO8 cohort
This prospective multicentric ANRS-C08 cohort of HIV-positive individuals, with continuous ascertainment of relevant variables and collection of detailed information on ARV usage, is also representative of patients who started potent ARV therapy with a PI in the early years (1997–1999), who were in the vast majority subsequently switched to non-nucleoside reverse transcriptase inhibitor (NNRTI) and exposed to more than 10 years of ARVs. Eligibility criteria included informed consent, follow-up with standardized clinical and biological assessments of more than 10 years in the cohort. 8 The Ethics Committee of Cochin Hospital, Paris, France, approved the study and informed consent was obtained for all participants. Among the 511 eligible patients of the ANRS-C08 cohort, after a median duration of 11 years of follow-up [interquartile range (IQR) 10–12], a cross-sectional last visit was conducted, which included concomitant clinical and ART assessment, CD4, and HIV RNA measurement. 9 During this visit, 162 patients specifically consented to take part in the bone substudy that included DXA and renal tubular marker assessment. There were no differences between the bone substudy group and the group that did not undergo the bone evaluation, with mean age of 50 years versus 49.4 years, male 81% versus 82%. None of the other characteristics (weight, HCV, smoking status, AIDS stage before inclusion, CD4 level, CD4/CD8 level, and VL) differed between the two groups.
Measurement of BMD
BMD (g/cm2) was measured at the lumbar spine (L1–L4) and hip by DXA devices (Hologic, Inc., Waltham, MA) or GE-Lunar (GE Healthcare, Madison, WI). As a 97 quality assurance procedure, all scans were reviewed by central reading to ensure the good positioning of the patients and the respect of the manufacturer's recommendations for the scan analysis. Since the population included males above and below 50 years, premenopausal and postmenopausal females, Z-score and not T-score was used to define low BMD, with a threshold below −2.0 standard deviations (−2SD) at the spine and/or hip. Because BMD values were obtained from two softwares, they were converted into standardized BMD (mg/cm2) using published formulae. 10,11
Measurement of renal tubular markers
Renal function was evaluated by estimating glomerular filtration using the Modification of the Diet in Renal Disease equation, mL/min/1.73 m2, 12 serum phosphorus, maximum tubular phosphate reabsorption (TmPi), 25(OH) vitamin D, urine phosphorus, urine uric acid, and urinary pyridinoline. History of renal colic was also collected. All biologic samples were centralized and analyzed in a single reference laboratory.
Statistical analyses
To assess the ARVs exposure for each patients, two surrogate markers of exposure were defined: the first “window of exposure” as an exposure of more than six cumulative months during the last 3 years before the DXA evaluation to account for a cumulative exposure that could affect bone remodeling, the second “current exposure” as a cross-sectional exposure at the date of DXA evaluation. These two markers were expressed in numbers (and proportions) of patients.
Categorical and continuous variables between groups were compared using Fisher exact test and Wilcoxon rank-sum test, respectively. Continuous variables were presented as median and 25th–75th percentile values (IQR). Categorical variables were presented as numbers and proportions.
To study the factors associated with low BMD, a multiple logistic regression analysis was performed with first a univariate selection at the threshold of 10% of the full set collected data and the window exposure to ARV then a backward selection. For the factors significantly associated, the adjusted odds ratio (aOR) was estimated with the 95% confidence interval (95% CI). Post hoc analysis was performed. Due to the higher proportion of male in our studied sample, a multiple logistic regression analysis was performed for this subgroup, also for the major group of age (45–60 years). The window of exposure to the two NNRTI, NVP, and efavirenz (EFV), was further explored with the different markers of BMD.
Statistical analyses were performed using SAS, version 13.2 (SAS Institute, Inc., Cary, NC) by a dedicated statistician. All tests were two sided with a 5% type I error.
Results
A low BMD (Z-score < −2) was evidenced in 18% (95% CI: 12–26) of males versus 6% (95% CI: 0–21) of females. Main characteristics, bone and renal status, as well as window of exposure to ARVs and current exposure to ARVs of the 162 patients, according the gender and the Z-score < −2, are shown in Table 1. Median total duration of exposure to PI was 4.3 (IQR: 1.8–7.8) years. Median total duration of exposure to PI (n = 90) and to TDF (n = 91) was 6.8 (2.8–9.6) and 3.8 (1.7–5.5) years, respectively, for patients exposed during the window of exposure to PI and TDF. Of the 50 patients on window of exposure to NVP, 24 had a backbone with TDF and 23 with abacavir (ABC). The total duration of exposure to PI and to ABC were no differences in patients with or without window of exposure to NVP (p = .83 and p = .26, respectively).
Characteristics of the 162 Patients for Demographic Data, Human Immunodeficiency Virus Status, Bone and Renal Assessment, and Treatment According to the Gender and the Bone Status (Z-score < −2)
Data are presented as median (interquartile range).
Exact values are presented for the two women patients with a Z-score < −2.
nmol/mmol of creatinine.
Window of exposure in last 3 years with at least 6 months of cumulative treatment prior the DXA evaluation.
Current exposition at the date of DXA evaluation.
3TC, lamivudine; ABC, abacavir; ART, antiretroviral therapy; ARV, antiretroviral drug; AZT, zidovudine; BMD, bone mineral density; d4T, stavudine; DXA, dual-energy X-ray absorptiometry; EFV, efavirenz; FTC, emtricitabine; HBV, hepatitis B virus; HCV, hepatitis C virus; HIV, human immunodeficiency virus; IDV, indinavir; LPV, lopinavir; MDRD, Modification of the Diet in Renal Disease; NA, data not available; NFV, nelfinavir; NVP, nevirapine; PI, protease inhibitor; sBMD, standardized bone mineral density; SQV, saquinavir; TDF, tenofovir; TmPi, maximum tubular phosphate reabsorption.
Multivariate analysis
Based on the univariate selection of the full set data as shown in Table 1 (eight factors at 10% threshold HCV coinfection, renal colic history, uric acid renal loss, body weight, and window of exposure to NVP, EFV, saquinavir, and nelfinavir), the multiple logistic regression model identified two factors associated with a Z-score < −2, uric acid renal loss (aOR: 5.7; 95% CI: 1.4–22.7; p = .013) and window of exposure to NVP (aOR: 0.11; 95% CI: 0.02–0.5; p = .006) with the same result adjusted on age. Based only on the male population (81% of our study sample), with the same univariate selected set, three variables were associated with a Z-score < −2: uric acid renal loss (aOR: 6.1; 95% CI: 1.2–31.5; p = .029), HCV coinfection (aOR: 4.0; 95% CI: 1.3–12.2; p = .016), and window of exposure to NVP (aOR: 0.1; 95% CI: 0.02–0.6; p = .010). For the group 45–60 years, representing two-third of the full study sample, Z-score < −2 was associated to HCV coinfection (aOR: 4.23; 95% CI: 1.20–14.92; p = .025) and window of exposure to NVP (aOR: 0.093; 95% CI: 0.011–0.77; p = .028) but not to uric acid renal loss. The positive association between window of exposure to NVP and high BMD was independent of window of exposure or current exposure to TDF or to PI(±r) or to their combination during the past 3 years (no relevant clinical association for TDF or PI).
Bone mineral density and non-nucleoside reverse transcriptase inhibitor exposure
The two NNRTIs (EFV and NVP) were prescribed for 53% (86) patients (only one patient received both drugs during the last 3 years), with always 43% patients on current exposure at DXA evaluation. Of the 50 patients on window of exposure to NVP, 24 had a backbone with TDF and 23 with ABC. Median total exposure (since the 10 years of follow-up) to PI (n = 90) and to TDF (n = 91) was 6.8 (2.8–9.6) and 3.8 (1.7–5.5) years, respectively, for patients exposed during the window of exposure to PI or TDF, with no differences in patients with or without window of exposure to NVP (p = .83 and p = .26, respectively). The total duration of NVP and EFV exposure (since the 10 years of follow-up) was categorized in four classes, no exposure to NVP or EFV, less than 5 years, 5–10 years, and more than 10 years. This total duration of exposure to NVP and BMD assessed by L1–L4 Z-score was significantly associated (p = .004), with a median L1–L4 Z-score of −1.0 (IQR −1.8 to 0.2) and of 0.2 (−0.7 to 0.8) for the no exposure and the more than 10-year exposure groups, respectively (Fig. 1), not observed with total duration of exposure to EFV (p = .84). No significant association was estimated between window of exposure to NVP and hip Z-score. Spine Z-score < −2 was associated to window of exposure to NVP (logistic regression model, aOR: 0.1; 95% CI: 0.02–0.6; p = .006).
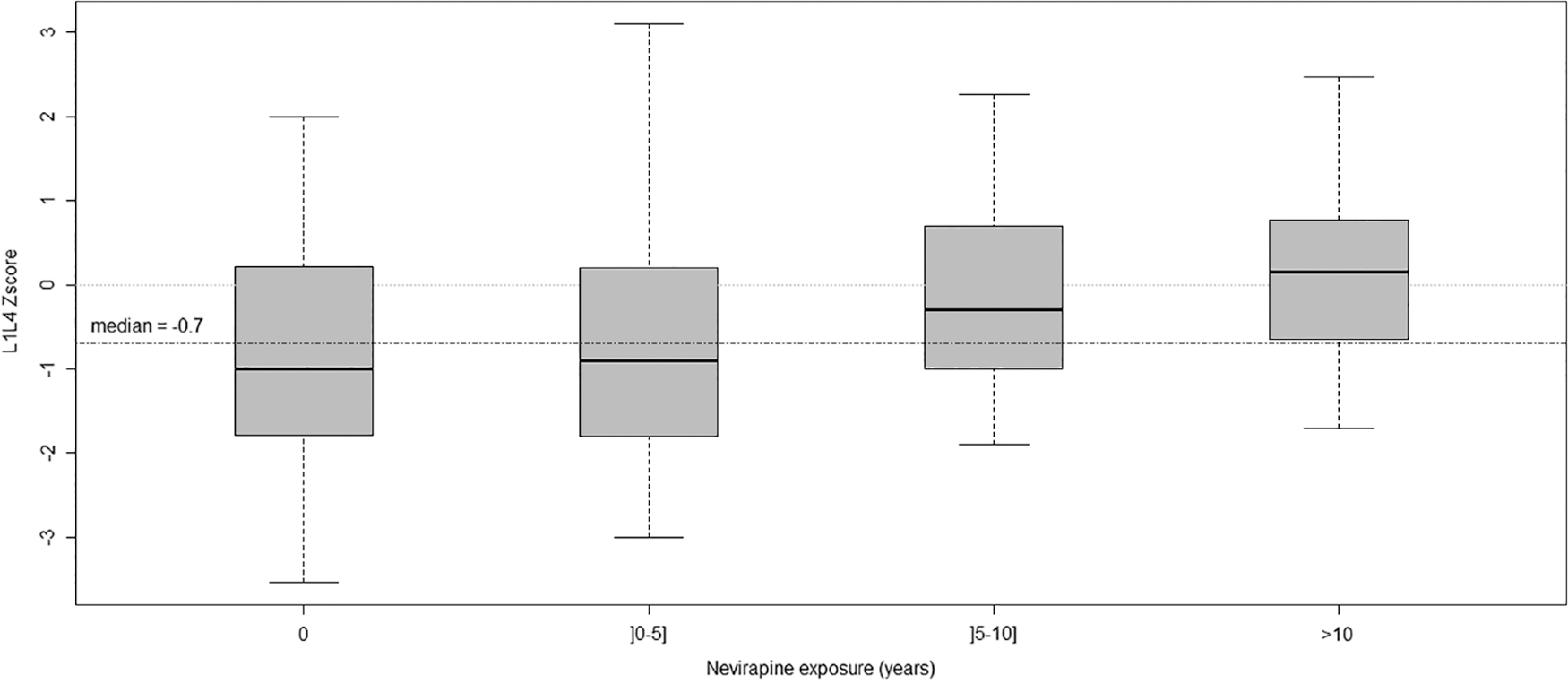
L1–L4 Z-score according to the total nevirapine exposure of the 162 bone substudy patients for the 10 years of follow-up [no exposure to nevirapine: 81 patients (50%); 0–5 years: 36 patients (22%); 5–10 years: 21 patients (13%) and >10 years: 24 patients (15%)] with p = .004 of Wilcoxon rank-sum test. Boxes represent median with 75th percentile (top line of box), 25th percentile (bottom line of box), minimum and maximum (bars projecting up and down from the box). Dashed line represents common median L1–L4 Z-score as median = −0.07 on 10 years.
Discussion
Loss of bone mineral density in HIV-1 positive subjects
In this cross-sectional study of predominantly male HIV-positive adults 50 years of age with more than 10 years of ART therapy and well-controlled HIV infection for the vast majority, we observed high prevalence of low BMD and osteoporosis, 16% (95% CI: 10–22) and 17% (95% CI: 11–23), respectively. Studies evaluating similar population found similar results. 6,13 In the Amsterdam AGeHIV cohort, prevalence of osteoporosis was nearly twice as high in HIV-positive middle-aged persons, in a predominantly MSM (men who have sex with men) population 45 years of age and treated with ARV for a median of 9.9 years, than in HIV-negative individuals (13.3% vs. 6.7%). 6 In a meta-analysis, including 11 published studies with various duration of ARV exposure, the overall prevalence of osteoporosis in HIV-positive patients was 15%. 2 Interestingly, a longitudinal study, with 7.5 years follow-up, suggested that, after a rapid decline during the first 2 years of ARV therapy, BMD loss stabilizes or continues to decline, although at a much slower rate, especially at the lumbar spine. 14 Furthermore, in this longitudinal study, there was no relationship between cumulative TDF or PI exposure and BMD decline during the late period, from year 2 to 7. 14 Moreover, always in this longitudinal study, lower lean body mass and HCV coinfection are associated with lower BMD, while HIV treatment characteristics are not also illustrated by Bedimo et al. and Kooij et al. 6,14,15
Bone mineral density loss and ARV exposure
In our study, HCV coinfection but not body weight was associated with lower BMD, while HIV-related factors (CD4 cell count or HIV-1 RNA) were not. Although TDF and PI are associated with BMD loss in the first 2 years of therapy, 2,14,16 it has been suggested that continuous exposure to these ARV do not play a role in the subsequent slow BMD loss over time. 6,14 Similar to the Amsterdam cohort, window of TDF exposure was not associated with low BMD in our study. 6 In a recent meta-analysis covering 7,198 patient-years of follow-up, higher risks of bone and renal adverse events with TDF were only seen when TDF was used in combination with ritonavir or cobicistat. 17 In the Amsterdam AGeHIV cohort, a significantly positive association was observed between current use of NVP and BMD, and a significantly negative association between the duration of exposure to high-dose (≥400 mg/day) ritonavir and BMD. 6 We confirm in this study the positive association between BMD and use of NVP for more than six cumulative months during the last 3 years; further analysis showed that there was significant and linear trend between cumulative NVP exposure and unaltered BMD 11 years after initiation of potent ARV therapy. A similar positive effect on BMD among NVP-treated HIV adults and infants has been reported. 18,19 Lack of positive association between EFV exposure and BMD might be explained by increased risk of vitamin D deficiency on EFV.
Study limitations and strength
Our study, like other cross-sectional ones, has limitations: absence of a control group, absence of baseline and repeated BMD measurement due to its cross-sectional design, limited power due to sample size which could explain lack of association with certain factors, low representation of women, with few postmenopausal women, absence of collection of other variables that could be related to osteopenia such as steroid use, diabetes mellitus, hyperthyroidism, methadone and hypogonadism, no analysis of fractures, and the calcium and vitamin D supplementation. But consistency of NVP-positive effect on BMD and positive effect of prolonged NVP exposure raise interesting questions. Association does not mean causation. There are no in vitro or animal studies on the effect of NVP on bone biomarkers and bone density turnover, precluding any hypothesis on the mechanism, either direct or indirect, underlying the positive effect of NVP on BMD. NVP effect was not a NNRTI class effect nor solely a PI-sparing effect, as EFV was not associated with BMD. We have previously published, on the same cohort that the incidence of fractures is relatively low (3.3/1,000 patient-years), with most fractures being posttraumatic. 20 Very large cohorts would be needed to assess role of the various antiretrovirals on the risk of fractures. Despite these limitations, our cohort is representative of patients who started potent triple ARV therapy in the early years (1997–1999), with 100% starting on a PI-containing regimen and the majority being later switched to a NNRTI regimen, TDF being introduced much later on as an alternative NRTI backbone.
Summary and conclusions
In summary, in males, uric acid renal loss, HCV coinfection, and window of NVP exposure were associated with BMD status. For the full study sample, there was a strong positive association between duration of exposure to NVP and lumbar spine Z-score. Although NVP is nowadays much less used, our data added a favorable element on the long-term tolerance of this antiretroviral medication. Further studies are needed to investigate the mechanism by which NVP could be associated to high BMD, and to determine whether this is also seen in patients never exposed to PI and/or starting upfront NVP-based ART.
Footnotes
Acknowledgments
The authors would like to thank all participating patients, nurses, and physicians in clinical sites.
The ANRS CO8 APROCO-COPILOTE Cohort Study Group is composed of the following:
Scientific committee:
Steering committee: C. Leport and F. Raffi (principal investigators), G. Chêne and R. Salamon (methodology), J. P. Moatti, J. Pierret, and B. Spire (social sciences), F. Brun-Vézinet, H. Fleury, and B. Masquelier (virology), and G. Peytavin and R. Garraffo (pharmacology).
Other members: D. Costagliola, P. Dellamonica, C. Katlama, L. Meyer, D. Salmon, and A. Sobel.
Events validation committee: L. Cuzin, M. Dupon, X. Duval, V. Le Moing, B. Marchou, T. May, P. Morlat, C. Rabaud, and A. Waldner-Combernoux.
Project coordination: L. Hardel, P. Reboud.
ANRS representatives: S. Couffin-Cadiergues and L. Marchand.
Methodological, statistical, and other contributions: A. Assuied, P. Carrieri, S. Habak, F. Couturier, C. Jadand, A. Perrier, M. Préau, and C. Protopopescu.
Clinical centers (investigators): Amiens (Pr. J.L. Schmit), Angers (Dr. J.M. Chennebault), Belfort (Dr. J.P. Faller), Besançon (Pr. N. Magy-Bertrand, Pr. C. Chirouze and Pr. P. Humbert), Bordeaux (Pr. M. Dupon, Pr. Longy-Boursier, Pr. P. Morlat and Pr. D. Neau), Bourg-en-Bresse (Dr. P. Granier), Brest (Pr. S. Ansart), Caen (Pr. R. Verdon), Compiègne (Dr. D. Merrien), Corbeil Essonnes (Dr. P. Chevojon), Créteil (Pr. A. Sobel, Pr. Y. Levy), Dijon (Pr. L. Piroth), Garches (Pr. C. Perronne), Lagny (Dr. E. Froguel), Libourne (Dr. J. Ceccaldi), Lyon (Pr. C. Chidiac), Meaux (Dr. V. Grégoire), Montpellier (Pr. J. Reynes), Nancy (Pr. T. May), Nantes (Pr. F. Raffi), Nice (Pr. J. G. Fuzibet and Pr. P. Dellamonica), Orléans (Dr. P. Arsac), Paris (Pr. E. Bouvet, Pr. F. Bricaire, Dr. J. Monsonego, Pr. P.M. Girard, Pr. L. Guillevin, Pr. S. Herson, Pr. C. Leport, Pr. J.M. Molina, Pr. G. Pialoux, Pr. O. Sain, Pr. D. Salmon, and Dr. P. Sellier), Poitiers (Pr. F. Roblot), Reims (Pr. F. Bani-Sadr), Rennes (Pr. C. Michelet), Saint-Etienne (Pr. F. Lucht), Saint-Mandé (Pr. C. Debord), Strasbourg (Pr. T. Martin), Toulon (Dr. J.P. De Jaureguiberry), Toulouse (Pr. B. Marchou), and Tours (Pr. L. Bernard).
Author Disclosure Statement
No competing financial interests exist.
Funding Information
The French National Institute for Health and Medical Research–France Recherche Nord&Sud Sida-HIV Hepatites (INSERM-ANRS) was the sponsor and a funder of the APROCO-COPILOTE CO8 cohort. The cohort was also supported by CMIT (Collège des Universitaires de Maladies Infectieuses et Tropicales), Sidaction Ensemble contre le Sida, and associated pharmaceutical companies: Abbott, Boehringer-Ingelheim, Bristol-Myers Squibb, GlaxoSmithKline, Gilead Sciences, Pfizer, and Roche.