
Abstract
Barriers to sustainable virologic suppression (VS) of HIV-infected adolescents and young adults include drug resistance mutations (DRMs) and limited treatment options, which may impact the outcome of second-line antiretroviral therapy (ART). We sequenced plasma viral RNA from 74 adolescents and young adults (16–24 years) failing first-line ART at Newlands Clinic, Zimbabwe between October 2015 and December 2016. We evaluated first-line nucleoside reverse transcriptase inhibitor (NRTI) susceptibility scores to first- and second-line regimens. Boosted protease inhibitor (bPI)-based ART was provided and viral load (VL) monitored for ≥48 weeks. Fisher's exact test was used to evaluate factors associated with VS on second-line regimens, defined as VL <1,000 copies/mL (VS1,000) or <50 copies/mL (VS50). The 74 participants on first-line ART had a median [interquartile range (IQR)] age of 18 (16–21) years and 42 (57%) were female. The mean (±standard deviation) duration on ART was 5.5 (±3.06) years and the median (IQR) log10 VL was 4.26 (3.78–4.83) copies/mL. After switching to a second-line PI regimen, 88% suppressed to <1,000 copies/mL and 76% to <50 copies/mL at ≥48 weeks. A new NRTI was associated with increased VS50 (p = .031). These 74 adolescents and young adults failing first-line ART demonstrated high levels (97%) of DRMs, despite enhanced adherence counseling. Switching to new NRTIs in second-line improved VS. With the widespread adoption of generic dolutegravir, lamivudine and tenofovir combinations in Africa, genotyping to determine NRTI susceptibility, may be warranted.
Introduction
Although there has been an increase in access to antiretroviral therapy (ART) in sub-Saharan Africa (SSA) and other low- and middle-income countries (LMICs), HIV and AIDS remain a major public health burden. Zimbabwe has an HIV prevalence of 14.6% among the adult population (15–64 years) and ∼4.7% among adolescents and young adults (15–24 years). 1 The roll out of ART has resulted in a significant reduction in HIV/AIDS-related morbidity and mortality 2,3 and has transformed the disease from being life-threatening into a chronic and manageable condition among individuals with good adherence. To meet the World Health Organization (WHO)/The Joint United Nations Programme on HIV/AIDS goals of universal access to treatment to eliminate HIV by 2030, Zimbabwe adopted a policy of test and treat in 2016. 4
Public health ART, as recommended by the WHO, is possible because of access to low-cost generic fixed dose combinations (FDC). 5 –7 ART, clinical support, and adherence counseling to maintain virologic suppression (VS; the third 90) are particularly challenging for adolescents and young adults living with HIV. 8 –11 In the last few years in Africa, single-dose daily combination therapy in both first- and second-line treatment has become more tolerable, acceptable, and effective than multipill regimens. 12 –14
A substantial change in public health ART in Africa is the roll-out of FDC of tenofovir, lamivudine, and dolutegravir (TLD) recommended by WHO for first- and second-line treatment. 15 Among adolescents and young adults, TLD may be a more economical, convenient, and better-tolerated regimen. However, the effectiveness of TLD as a FDC may be reduced by accumulated nucleoside reverse transcriptase inhibitor (NRTI) resistance mutations.
In this study, we evaluated adolescents and young adults who had received an enhanced adherence counseling (EAC) for virologic failure (VF) after treatment with recommended, available FDCs. Patterns of HIV drug resistance mutations (DRMs) and first-line NRTI drug susceptibility, which may impact virologic response to second-line protease inhibitor (PI)-based ART were estimated. As these adolescents and young adults were switched to second-line treatment and followed for ≥48 weeks, we evaluated the relationship between DRMs, genotypic susceptibility, and the impact of DRMs on viral load suppression (VLS).
Materials and Methods
Study design
This was a retrospective analysis of 74 adolescents and young adults failing recommended first-line treatment from a cohort of 726 HIV-infected adolescents and young adults receiving care and treatment at Newlands Clinic Harare, Zimbabwe between October 2015 and December 2016. Genotyping performed after VF (defined as viral load, VL >1,000 copies/mL) was recorded, following weekly enhanced adherence counseling group intervention (EACGI) for 12 weeks. Second-line treatment was initiated and 6 monthly VL measures were continued after the switch. (Fig. 1).
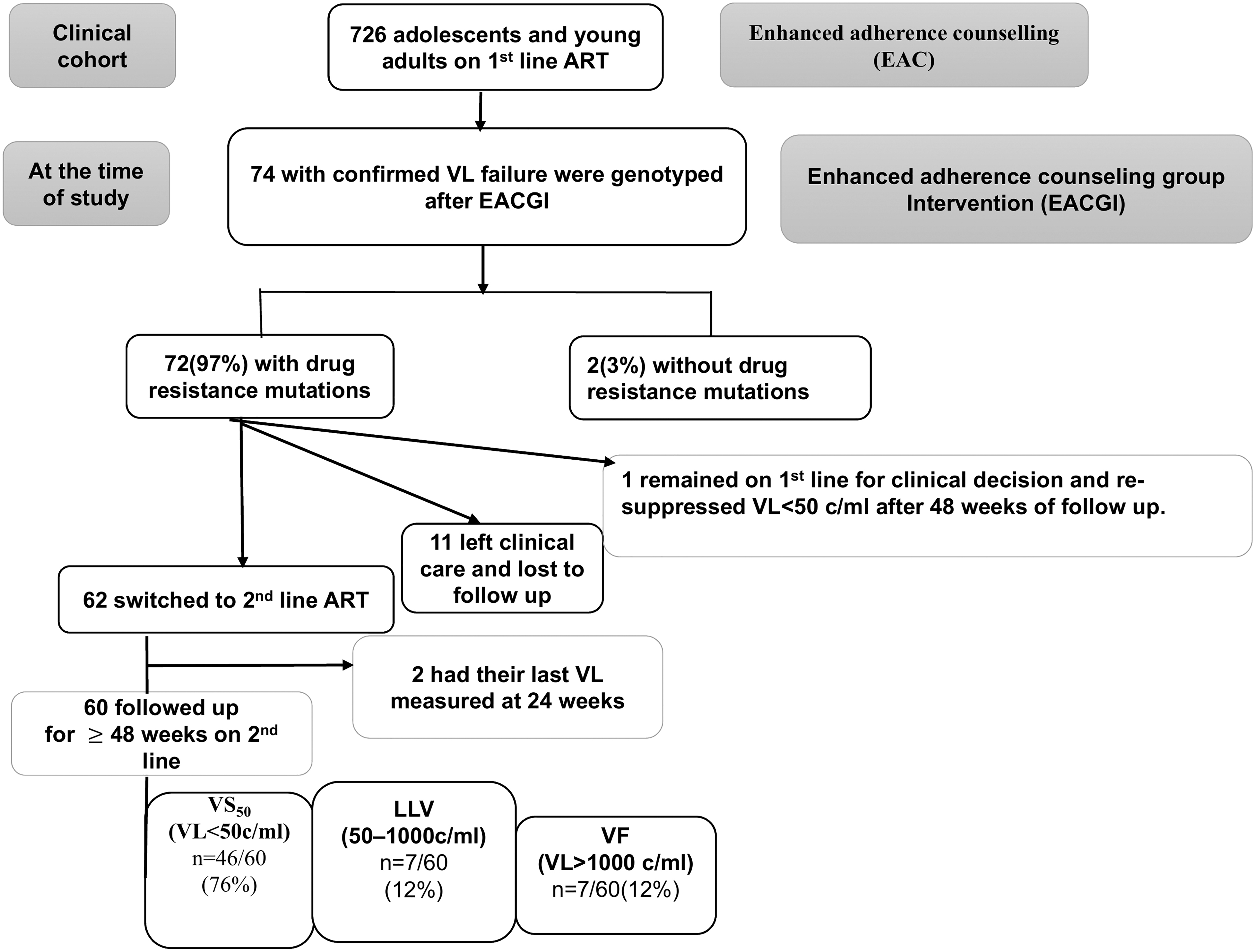
Summary of the participants at first-line ART and outcomes after switch to second-line ART, ART, antiretroviral therapy; EAC, enhanced adherence counseling; VL, viral load; EACGI, enhanced adherence counseling group intervention; bPI, boosted protease inhibitor; VS, virologic suppression; VS50, virologic suppression VL <50 copies/mL; LLV, low-level viremia; VF, virologic failure (VL >1,000 copies/mL).
Study setting
Newlands Clinic is a private voluntary organization founded in Harare, Zimbabwe in 2004 with the aim of providing comprehensive ART services to people living with HIV from poor communities in and around Harare. Nurses with counseling qualifications provide routine adherence and psychosocial counseling at each clinic visit. 16 For HIV-infected adolescents and young adults with VF on ART, an EACGI is provided through a psychological and mental health approach. The EACGI accommodates 8–15 young people as 12 weekly one and half hour-long sessions to facilitate adherence and provide peer support through weekly group meetings. The clinic provides first- and second-line ART as recommended by the Ministry of Health and Child Care ART program. First-line ART was provided as FDCs of tenofovir disoproxil fumarate/lamivudine (TDF +3TC), abacavir/lamivudine (ABC +3TC), or zidovudine/lamivudine (AZT +3TC). These were combined with either efavirenz (EFV) or nevirapine (NVP). Second-line treatment was with a PI, either ritonavir-boosted atazanavir (ATV/r) or ritonavir-boosted lopinavir (LPV/r) with TDF +3TC or ABC +3TC or AZT +3TC.
Laboratory methods
The plasma VL were obtained in real-time for clinical management with the COBAS AmpliPrep/TaqMan48 HIV-1 quantification system (Roche Diagnostics). For HIV-1 drug resistance genotyping, RNA was extracted using the QIAMP Viral RNA kit (Qiagen, Germany), as per manufacturers' instructions. The extracted RNA samples were reverse transcribed and amplified using the Southern African Treatment Resistance Network (SATuRN) protocol on the PTC-200 Peltier Thermal Cycler (MJ Research, Temecula, CA) at the University of Zimbabwe, College of Health Sciences. The SATuRN/Life Technologies genotyping method is a fully integrated protocol for surveillance and monitoring of drug resistance. The SATuRN protocol was designed to be an affordable protocol implementing mostly open source and open access bioinformatics resources for the interpretation of HIV drug resistance.
17
The amplicons generated were sequenced by Sanger sequencing at Molecular Cloning Laboratories, San Francisco, CA. The quality of the consensus sequences generated was verified by phylogenetic tree reconstruction in Geneious software, version 8 (
Virologic analysis and DRMs
VS was categorized as VL <50 copies/mL (VS50) and VL between 50 and 1,000 copies/mL [low-level viremia (LLV)] at ≥48 weeks. For clinical management of the participants, the WHO (Public Health ART) guidelines define VS, as VL <1,000 copies/mL (VS1,000) and VF as VL >1,000 copies/mL on two consecutive VL measurements within a 3-month interval with adherence support between measurements. 21
Genotypes were classified as wild type, nonnucleoside reverse transcriptase inhibitor (NNRTI) mutations only, or two-class resistance with mutations to both NNRTI and NRTI drugs. Susceptibility to second generation NNRTIs etravirine (ETR) and rilpivirine (RPV) was estimated based on detection of L100I, K101EP, Y181CIV, Y188L, G190EQ, and M230L as major resistance mutations. 22,23 Major NRTI, NNRTI, and PI mutation sites/codons were determined using the Stanford HIVdb. Total genotypic susceptibility scores were calculated for first-line regimens (GSS1). For each NRTI and NNRTI drug prescribed, a GSS value of 1 was assigned if resistance was not identified, a value of 0.5 was assigned to intermediate resistance and 0 was assigned when mutations predicted high-level resistance.
Total genotypic susceptibility scores were also calculated for second-line regimens (GSS2). For this, first-line NRTI genotypic results were used and a value of 1.5 was assigned to boosted PIs (bPIs). These GSS2 were based on ritonavir bPIs with two NRTIs; ABC or TDF or AZT and 3TC. Total genotypic susceptibility scores were calculated based on the number of ‘active’ drugs prescribed using the Rega Institute HIV algorithm on the Stanford HIVdb. 24 The arithmetic sum of the individual scores for the specific drugs prescribed provided the total GSS.
Statistical analysis
Descriptive statistics were used to summarize the baseline demographic and clinical characteristics as well as DRMs among the participants. Fisher's exact test, Kruskal-Wallis H test or analysis of variance test, and Student's t test were used to evaluate factors (age, ART duration, NRTI mutations on first-line failure, GSS and mean VL at 24 and 48 weeks on second-line ART) associated with VS on second-line ART, categorized as VL <50 copies/mL (VS50) and VL between 50 and 1,000 copies/mL (LLV). Significance levels were set at p = .05. All statistical analyses were performed using Stata version 14 (StataCorp LP, College Station, TX; 800-STATA-PC).
Ethics approval and consent to participate
Ethical approval was obtained from the Biomedical Research Training Institute-Institutional Review Board (AP142/2017) and the Medical Research Council of Zimbabwe (MRCZ/E/191). Permission to conduct the research was approved by the Newlands Clinic Research Board.
Results
Participant characteristics
Among 726 adolescents and young adults (16–24 years) who were receiving first-line ART at the Newlands Clinic between October 2015 and December 2016, 74 (10%) had a confirmed VL >1,000 copies/mL after 12 weeks of EACGI. The 74 participants, median [interquartile range (IQR)] age of 18 (16–21) years were receiving treatment with single daily dose regimens; TDF +3TC + EFV/NVP 54 (73%) and ABC +3TC + EFV/NVP 3 (4%), or twice daily regimens of AZT +3TC + EFV/NVP 17 (23%). Their demographic and clinical characteristics are shown in Table 1.
Participant Characteristics at the Time of the Study
IQR, interquartile range; SD, standard deviation; TDF, tenofovir disoproxil fumarate; 3TC, lamivudine; EFV, efavirenz; NVP, nevirapine; AZT, zidovudine; ABC, abacavir; ATV/r, atazanavir/ritonavir; LPV/r, lopinavir/ritonavir; ART, antiretroviral therapy.
Of the 74 participants failing NNRTI-based first-line ART, 62 (84%) were switched to a bPI-based second-line ART, one (1%) remained on first-line ART and suppressed at ≥48 weeks of follow-up. Among the 62 participants switched to a bPI-based second-line ART, 60 (82%) were followed up to ≥48 weeks, while two (3%) participants had their last VL measured at 24 weeks. The remaining 11 (15%) participants left clinical care and were lost to follow-up (Fig. 1).
Drug resistance at first-line failure
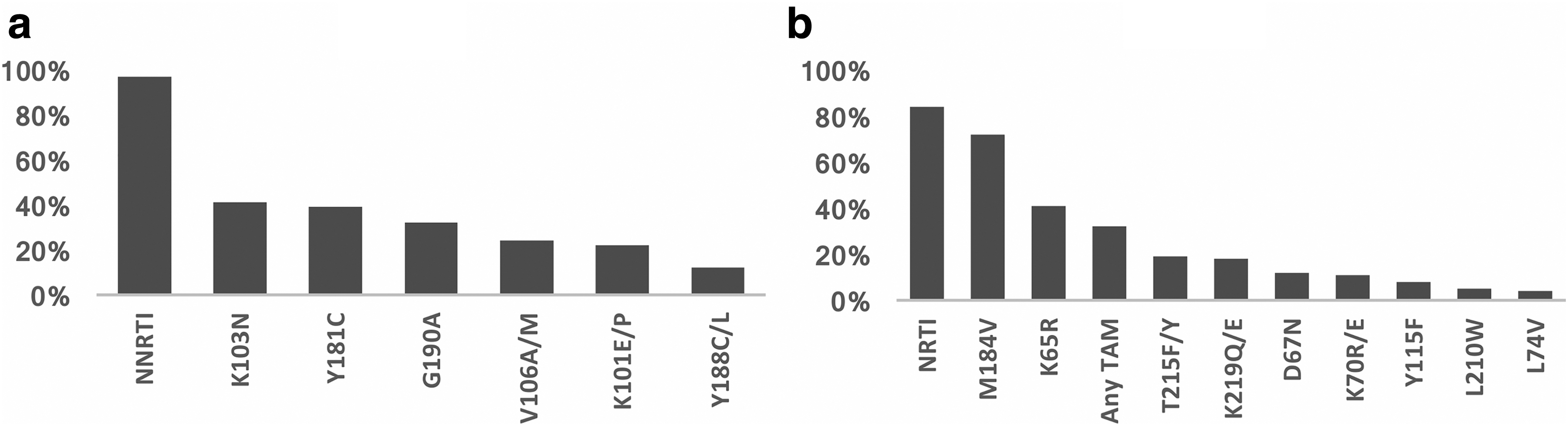
HIV DRMs were detected in 72/74 (97%) participants after EAC and confirmed VF. The frequency of NNRTI DRMs is shown in Figure 2a. NRTI DRMs were found in 84% with the most common being M184V (72%), K65R (41%), and thymidine analog mutations (32%) (Fig. 2b). Additional NRTI mutations, L74V and Y115F, were identified among all three participants on ABC at first-line ART failure (Fig. 2b). The combination of K65R and M184V, associated with ABC, TDF, and 3TC resistance was identified in 28/74 (38%) participants. NRTI and NNRTI DRMs (two class resistance) were detected in 62/74 (84%). Susceptibility to new second-generation NNRTIs, ETR and RPV, was reported as 31 (42%) to ETV and 19 (35%) to RPV.
(
NRTI drug switching from first- to second-line ART regimen
After first-line treatment failure, 62 of the 74 (84%) participants switched to a second-line treatment, which included continuation of 3TC and either a change to a new or recycled NRTI and ATV/r (54/62) or LPV/r (8/62). Genotyping results were not always available in real-time to health care providers. In 23/60 (38%) cases, participants remained on the same NRTI combination. This was based on a reluctance to use AZT +3TC (a recommended NRTI combination after failure of a TDF-based regimen). 25 The 37 who switched to a new NRTI backbone demonstrated VS50 in 86% (32/37) compared to 61% (14/23) who continued on the same NRTI backbone (p = .031) (Fischer's exact test). The 37 participants who switched to a new NRTI backbone were most often switching from TDF to ABC (Supplementary Fig. S1). Upon switching to a bPI regimen, significant differences were not observed in VS50 at ≥48 weeks; 58% (11/19) of the participants who remained on TDF compared to the 76% (19/25) who changed to a new NRTI backbone, respectively (p = .327) (Chi-Square test) (Supplementary Fig. S1).
The detection of M184V mutation at first-line treatment failure was significantly associated with VS50 (87%) on second-line treatment compared to LLV (57%) and VF (57%) (p = .038) (Kruskal-Wallis H test). The detection of K65R was more frequent in both VS50 (44%) and LLV (71%) categories compared to VF (14%) (p = .106) (Kruskal-Wallis H test).
Comparing genotypic susceptibility among these three categories on their first-line regimen, a significant greater susceptibility was seen among VF (median GSS1 of 1) compared to LLV (median GSS1 of 0.5) and those who achieved VS50 (median GSS1 of 0.5) (p = .042) (Kruskal-Wallis H test). No significant difference was seen on second-line regimens among VF (median GSS2 of 2.5), LLV (median GSS2 of 2), and those who achieved VS50 (median GSS2 of 2.25) (p = .154) (Kruskal-Wallis H test) (Table 2). Among the 46 who achieved VS50 on second-line ART, all eight (100%) participants on LPV/r achieved VS50 compared to the 38 (70%) who achieved VS50 on ATV/r (p = .10) (Fisher's exact test).
Characteristics Associated with Virologic Outcome After Switch to Second-Line Antiretroviral Therapy
M184V mutation causing high-level resistance to lamivudine (3TC) and emtricitabine (FTC), K65R Mutation causing high-level resistance to tenofovir (TDF) and decrease susceptibility to abacavir (ABC), Median viral load at 24 and 48 weeks while on second-line protease inhibitor-based regimen.
Statistically significant with p value < 0.05.
VS, virologic suppression (VS <50 copies/mL); LLV, low-level viremia (50–1,000 copies/mL); VF, virologic failure (VL ≥1,000 copies/mL); VL, viral load.
Discussion
Adolescents and young adults globally pose challenges to HIV treatment programs, particularly in LMICs where weak health systems, lack of support for adherence and retention and limited access to VL monitoring, contribute to VF. 26,27 While ART has been effective in decreasing AIDS-related deaths among adults, benefits among adolescents and younger adults have been limited. 21 In SSA, poor adherence and loss to follow-up among adolescents and young adults have been reported compared to older individuals living with HIV. 28 –30 In 2015 in Zimbabwe, VF rates were nearly 40% among 15–19-year-olds. 1,31 Policy and guidelines support service delivery to improve adherence, viral suppression, and clinical outcomes among adolescents. 32 Similarly, the WHO guidelines encourage EAC before switching to a new regimen. 21
In a clinic in Harare, we documented the patterns of DRMs and evaluated second-line treatment outcomes among HIV-1-infected adolescents and young adults who had failed a first-line ART regimen despite EAC for 12 weeks. Genotyping after failure demonstrated that 97% had at least one clinically significant HIV DRM and resistance to two drug classes (NNRTI and NRTI) was identified among 62/74 (84%). Although DRMs were common after first-line ART failure, switching to second-line bPI-based ART demonstrated suppression to <1,000 copies/mL in 53/60 (88%), consistent with studies among HIV-infected children and adults where VS in response to second-line regimens range from 70% to 95% after 48 weeks of follow-up. 33 –39
We observed that overall, first-line ART failures who changed to a new NRTI were more likely to achieve VS on second-line regimens compared to those who continued on the same NRTI (p = .031) (Fisher's exact test). Genotyping before the switch to second-line regimens demonstrated M184V (72%) and K65R (41%) at first-line ART failure. The WHO recommendations for NRTI switching suggest that first-line TDF recipients should be switched to AZT or ABC. 21 Based on the presence of a K65R mutation, AZT is the preferred NRTI. 40 –43 In this study, continuation of TDF from first- to second-line regimens resulted in 58% suppression, while switching from TDF to AZT or ABC demonstrated modestly higher VS50 in second-line regimens, 80% and 73%, respectively.
Our study identified a small but interesting subgroup with persistent LLV and with high levels of NRTI drug resistance. LLV (from 50 to 1,000 copies/mL) may be a precursor of VF, raising concerns about the long-term durability of second-line treatment. Hence, optimization of NRTI and intensification of treatment in patients with persistent LLV has been considered 44 –46 to achieve VS (VL <50 copies/mL). In a recent review, Ryscavage et al. concluded that resistance genotyping should be considered in patients with persistent LLV when feasible, and treatment should be modified if resistance is detected. 47
Alternatively, ATV/r in second-line regimens may also be linked to LLV and risk of VF. Recent systematic reviews of data comparing drugs used for second-line ART reported low- to very low-quality evidence for using ATV/r or DRV/r (once-daily) over LPV/r (twice-daily) as the preferred bPI option (
Genotypic assessment of drug susceptibility and the prediction of treatment outcome have been well studied in resource rich settings. 49 –51 However, in second-line studies in LMICs, increased genotypic susceptibility to NRTI drugs and fewer mutations have been associated with VF of second-line as documented in adults. 52 –56 This provides indirect evidence that those failing second-line regimens may be inconsistently adherent. The participants, studied here, who failed second-line regimens with high VL had a distinct lack of NRTI mutations. Additional barriers to VLS in adolescents include drug toxicity and intolerance, psychological problems (depression, anxiety, and trauma) and social barriers, including stigma, have been linked to poor treatment adherence in adolescents and young adults. 57 –60
Important limitations of the study are that genotyping results after first-line ART failure were not always available in real-time to health care providers for the optimization of ART before switching to second-line regimens. In addition, limited adherence and ATV/r as second-line ART may have reduced the rate of VS50. Hence, the contribution of first-line NRTI resistance to second-line treatment is only estimates. Other limitations of our study include the small sample size and the follow-up of second-line treatment for only ≥48 weeks. The results suggest that genotyping results after first-line ART failure are of limited value and that nonadherence most likely accounts for high-level VF. The presence of both K65R and M184V among those treated with TDF or ABC and 3TC does provide evidence for genotypic resistance and virtual PI monotherapy in many second-line recipients. Long-term follow-up is needed to confirm whether VS to <50 copies is sustained.
In African Public Health treatment programs, second-line PI-based daily FDC treatment is provided to a growing population of highly NRTI and NNRTI experienced patients. 15,25 Here, VS to levels <1,000 and <50 copies/mL was found in 88% and 76%, respectively, at ≥48 weeks. High rates of VS similar to those reported in other studies provide reassurance of effective VS on a PI-based second-line ART. 35 –37 However, when the NRTI backbone is not optimized after failure of first-line ART, concern is raised about the durability of second-line treatment, particularly with ATV/r as the sole active agent in a population where many decades of continued treatment are anticipated. The costs, long-term adherence to bPIs, together with the increasing prevalence of NNRTI DRMs support the recent recommendations to adopt Integrase Strand Transfer Inhibitors such as dolutegravir (DTG). 15 The single tablet lower-cost TLD with a high genetic barrier to resistance may be more acceptable and effective than the current bPI and NNRTI regimens. 15,61 –63 This may extend suppressive ART treatment, particularly among adolescents and young adults failing current first- and second-line regimens with multidrug resistance. However, second- and third-line ART, including DTG, require active adherence support and frequent VL monitoring to prevent selection of resistance to DTG, further limiting options for this vulnerable and hard to treat population.
Conclusion
Clinically significant HIV DRMs were frequently detected (97%) among adolescents and young adults failing first-line ART. When switched to second-line ART, VS was higher in participants who received a new NRTI backbone as expected. Genotyping adds little to the choice of second-line NRTI regimens, except that the absence of first-line NRTI resistance appears to be a predictor of poor adherence and subsequent ART failure. The roll-out of TLD may improve ART treatment success in LMICs particularly among this hard to treat population.
Sequence Data
HIV-1 drug resistance sequence data are available on GenBank (accession numbers MK893083–MK893156).
Authors' Contributions
D.K., C.C., T.S., T.M., J.M., and V.K. conceived the study. T.S., T.M., B.V., and V.K. supervised data collection and laboratory testing. J.M., D.K., V.K., and
Footnotes
Acknowledgments
The authors are grateful to all study participants, clinicians, and staff at Newlands Clinic.
Author Disclosure Statement
All authors have no reported conflicts of interest. All authors have submitted the ICMJE Form for Disclosure of Potential Conflicts of Interest.
Funding Information
This work was financially supported by Newlands Clinic, a HIV ART charitable clinic and was made possible through various collaborations, both local and international. These include the Department of Medical Laboratory Sciences at the University of Zimbabwe, the Biomedical Research and Training Institute and Stanford University School of Medicine, Division of Infectious Diseases.
Supplementary Material
Supplementary Figure S1
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.