
Abstract
Pre-Exposure Prophylaxis (PrEP) has been widely accepted as an effective method to prevent HIV infections, but high costs precluded a widespread use in Germany. A novel distribution pathway of tenofovir-disoproxil fumarate and emtricitabine PrEP was implemented, which reduced monthly PrEP costs by 16-fold in Germany. Over a period of 6 months, we recorded prescription data, demographics, and sexual behavior of PrEP users, including self-reported sexually transmitted infections (STIs), alcohol and drug use. Within a month, prescriptions almost doubled from 585 to 1,009 and reached a cumulative number of 6,059 at the end of the 6-month observation period. Extrapolation of the data suggests an estimated maximal number of PrEP users of the order of 10,000. PrEP users demonstrated to be a population of well-educated men (407/686) who have sex with men (629/686), median age 38 (range:18–71), and of German descent (571/686). The majority used PrEP to compensate for risk of HIV infection when having condomless anal intercourse (372/686). At start of PrEP implementation, the majority perceived their own risk to acquire HIV as none to medium (78.6%; n = 539), while only a subset (18.8%; n = 129) considered themselves to be at high or very high risk for HIV infection. In contrast, within the last 6 months, 28.4% of the PrEP users had an STI diagnosis and over 70% had condomless anal intercourse with more than 6 partners. Taken together, our data from PrEP implementation in Germany demonstrate a large uptake once it became affordable in individuals who wish to compensate for HIV risk when having condomless anal intercourse.
Introduction
HIV Pre-Exposure Prophylaxis (PrEP) rapidly became a pillar of HIV prevention strategies in many countries worldwide after clinical trials have shown up to 86% reduction in HIV incidence, further corroborated by HIV incidence declines reported from countries and cities that implemented PrEP. 1 A population-level impact of PrEP together with treatment as prevention (TasP) is particularly seen in populations of men who have sex with men (MSM) in regions such as New South Wales (25.1% reduction of new HIV diagnoses), in cities such as San Francisco (over 51% reduction of new HIV diagnoses), and at single care providers such as Dean Street, London (80% reduction of new HIV diagnoses). 2 –4
PrEP was approved as a prevention method in Europe by the European Medical Agency (EMA) in 2016, but demand for PrEP in Germany was limited. 5 Reasons for this were multifactorial, including lack of knowledge about this new prevention method among MSM and physicians, as well as uncertainty about potential side effects. However, the primary limitation of widespread PrEP use was the high cost of PrEP of about 800Euro/month in the absence of health insurance reimbursement. 6 While the patent on tenofovir disoproxil fumarate and emtricitabine expired in 2017, generic drug prices still remained unaffordable at about 500Euro/month.
A novel distribution pathway was therefore established in a collaboration between German pharmacists specialist on HIV treatment (DAH2KA) and Kölsche Blister GmbH to provide PrEP at a 16-fold reduced monthly price from over 800€ to 50€, which allowed broader access to PrEP in at-risk communities.
The new distribution pathway of PrEP provided a unique opportunity to understand and track PrEP access in Germany for the first 6 months. Our aim was to describe demographics and sexual behavior of current PrEP users, which could help to formulate hypotheses for further research into potential groups of people at an increased risk for HIV, who are still not obtaining PrEP. We also aimed at predicting the number of future PrEP users and PrEP usage in the context of current recommendations. 7
Materials and Methods
Study characteristics
The study was reviewed and approved by the local ethics committee of the University Duisburg-Essen (17-7749-BO). The study was designed to obtain data on PrEP use frequency, as well as population characteristics and demographics from two sources. First, the main provider of low-price generic PrEP (Kölsche Blister GmbH) at that time produced individualized PrEP packages for people who had a prescription from their treating physician. For our analysis, we obtained anonymized information from these prescriptions. We inferred the number of prescriptions and the quantity of PrEP pills for each individual from the orders received from the DAH2KA pharmacies. Here, individual unit-dose blister packs containing emtricitabine/tenofovir-disoproxil (200 mg/245 mg) were produced and production time for each ordering pharmacy was recorded. Only anonymous data were analyzed for this study.
In addition, the pharmacies handed out a questionnaire to PrEP users when they picked up the order. They were asked to fill it out either directly or online. Every participant was provided with the information about the background and aim of the study before answering the questions. Moreover, the individuals were informed that participation in the study is voluntary and anonymous. Depending on the prescription, individuals would pick up their PrEP every month, every 2 months, or every 3 months. The questionnaire was also accessible online to users who received PrEP from other sources.
In the questionnaire, PrEP users were asked to give anonymous data on demographics, previous experience with PrEP, their perceived risk behavior, alcohol consumption, drug use, and sexually transmitted infections (STIs) over lifetime and within the last 6 months. The latter included the following infections: syphilis, Chlamydia trachomatis, Neisseria gonorrhoeae, Mycoplasma genitalium, Trichomonas vaginalis, genital warts, and hepatitis viruses. The data on demographics were compared with other publicly available data to determine if PrEP users differ from the German society in income and education level. 8,9
Statistical analysis
The results of the questionnaires underwent thorough quality control. To exclude potential duplications, we used a self-generated subject number and also removed all answers with an incorrectly generated subject number. Answers from the survey were deemed ineligible for analysis if they did not contain an answer to the question about previous completion of the survey, did not live in Germany, or were not a PrEP user.
Selected characteristics were compared between the group with prior PrEP experience and the group naive to PrEP with a Mann–Whitney U Test, Chi-square test, or Fisher's exact test as appropriate. In addition, associations between self-reported lifetime incidence of STI, sexual behavior, and sociodemographic covariables were analyzed in univariable and multivariable Poisson regression models. The latter was used to adjust the analyses for potential confounders and was performed excluding variables with a p-value >.2 in the univariable analysis. Incidence rate ratio (IRR) and 95% credible intervals (CI) were reported to measure the strength of association. All p-values <.05 were considered statistically significant. The analyses were compiled by using Stata (Stata Statistical Software: Release 14, College Station, TX).
The number of PrEP users taking PrEP regularly or “on demand” was determined by calculating the longest time between orders and comparing this to the observed time between the orders. If the observed time was longer than the expected time, the user was considered an “on demand” user. Since Kölsche Blister GmbH was the largest PrEP distribution center in Germany during the first 6 months, all analyses were derived from this data set.
To predict the number of PrEP users, a model was used, which assumes exponential convergence to a saturation value of PrEP users (“exponential convergence model”). Using the dates at which users received packages of different sizes (n × 28 pills with n = 1, 2, and 3) and assuming that PrEP is taken daily, the number of actual users (u) for each day was computed. We observed a dip around New Year (between 21st December 2017 and 1st March 2018), an effect that cannot be accommodated by a simple growth model. Therefore, two different subsets of data models were fit: Model 1 was formed to exclude the dip. Model 2 uses only data after the dip from 1st March 2018 to 29th March 2018. Both models assume that growth starts with zero users. The models were fitted by Bayesian inference, implemented with the R-package rethinking, 10 and sampled with Stan. 11 Sufficiency of sampling was checked by inspecting Stan output, and the model was validated by posterior predictive checks.
Results
Demographics and behavior of PrEP users in Germany
Between 1st October 2017 and 31st March 2018, 935 participants residing in Germany completed the questionnaire, of which 826 passed quality control. A total of 140 questionnaires were excluded as participants chose not to answer over a third of the questions or were filled out incorrectly using internal validation methods. Six hundred eighty six baseline questionnaires were used in our analyses.
The reported median age was 38 years (interquartile range 32–44) (Table 1). Most of the individuals were male at birth and of German origin. Overall, 59.3% (n = 407) had at least a bachelor's degree. In addition, 54.8% (n = 376) of the PrEP users had an annual income more than 40,000€, were in full-time employment (79.9%; n = 548), and had statutory medical insurance coverage (92.6%; n = 635). PrEP users identified themselves almost exclusively as gay men and only few referred to themselves as bisexual (4.2%, n = 29) or heterosexual (0.4%; n = 3). About half of the individuals (46.9%; n = 322) indicated that they currently had no steady partner.
Baseline Characteristics of Individuals (N = 686) with a Previous Pre-Exposure Prophylaxis Use and Before Pre-Exposure Prophylaxis Use
Data are no. (%) of patients, unless otherwise indicated. * p values (< 0.05) in bold depict significant results from Chi-square test or Fishers exact as appropriate. †At least once per month, ‡GHB/GBL, mephedrone, crystal meth, cocaine or ketamine.
The most commonly diagnosed STIs were gonorrhea (51.2%, n = 351), followed by chlamydia (36.2%, n = 248), genital warts (31.3%, n = 215), and syphilis (28.1%, n = 193). All participants were asked about their previous experience with medication-based HIV prophylaxis, and 20.3% (n = 139) reported having taken HIV post-exposure prophylaxis (PEP) once, while 7.4% (n = 51) reported obtaining PEP multiple times. When asked about the motivation to start PrEP, the majority chose the minimization of the risk of HIV infection when having condomless anal intercourse (54.2%; n = 372) and additional protection in case of a condom failure (51.3%; n = 352) or nonavailability of a condom (50.1%; n = 344). The majority of PrEP users reported to be adherent to PrEP (80.8%; n = 249) with no omission of a pill in the last month.
As we asked users whether they had already used PrEP before, we were able to compare differences between self-reported sexual behavior in individuals before initiating PrEP (n = 378) and those who had already been on PrEP (n = 308).
When asked about their self-assessed risk levels, we found that individuals on PrEP felt overall safer and less at risk for HIV infection than before taking PrEP (p = .01) (Table 1). This was despite substantially more self-reported condomless anal intercourse (p < .001). Just 5.2% (16/308) of participants always used a condom with PrEP and 17.9% (55/308) did not do that at all. Around 65.26% (201/308) of all individuals who started or had already taken PrEP had previously obtained PrEP at least once from other source than a pharmacy. This percentage increased to 90.95% (201/221) after exclusion of subjects who had started PrEP with the here described distribution pathway. Only 3.57% (11/308) obtained original or high-priced generic PrEP. This population represents as few as 1.60% (11/686) of all subjects.
Overall, we noted high levels of recreational drug intake in PrEP users. While 30% of PrEP users (n = 206) indicate regular alcohol consumption defined as at least one alcoholic beverage a month, 84.4% reported using recreational drugs and substances such as alkyl nitrites, also known as poppers (59.5%; n = 408), or drugs for erectile dysfunction (49.9%; n = 342). Almost one third of participants (31.5%, n = 216) took at least one drug out of the group of chemsex drugs: GHB/GBL, mephedrone, crystal meth, cocaine, or ketamine. 12 Overall, we observed also a significantly higher self-reported drug use in the group with PrEP experience compared to the group before initiating PrEP (p = .001).
Three quarters of all subjects (75.1%, n = 515) had at least one STI in their lifetime and 37.9% (n = 195) of them had been diagnosed with an STI in the last 6 months (28.4% of all subjects) (Table 2). We also compared the number of individuals with at least one STI over lifetime and within last 6 months in the group before PrEP to the group that had indicated previous PrEP use. Considering demographics, we found that these groups do not significantly differ with the exception of individuals having a health insurance (Table 2). However, the number of subjects without a health insurance was rather low.
Comparison of the Number of Individuals (N = 686) Who Indicated Previous Pre-Exposure Prophylaxis Use and Before Pre-Exposure Prophylaxis with at Least One Reported Sexual Transmitted Infection Within Last 6 Months and Over Lifetime
Data are no. (%) of patients, unless otherwise indicated. * p values (< 0.05) in bold depict significant results from Chi-square test or Fishers exact as appropriate.
To examine correlation between recent STI and various characteristics, we conducted univariable and multivariable Poisson regression analyses in individuals before PrEP and with a previous PrEP use (Table 3) as well as for each of those groups separately (Tables 4 and 5). Both univariable and multivariable model demonstrated a lower STI risk in individuals 50 years or older (univariable IRR = 0.78 (95% CI: 0.62–0.99) p = .040 and multivariable IRR = 0.76 (95% CI: 0.58–1.00) p = .048), those currently living in a relationship [univariable IRR = 0.86 (95% CI: 0.76–0.98) p = .019; multivariable IRR = 0.87 (95% CI: 0.76–1.00) p = .047] (Table 3), or those who previously used PrEP reporting use of erectile dysfunction medication (EDM) [multivariable IRR = 0.54 (95% CI: 0.30–0.98) p = .041] (Table 5). Among subjects who indicated previous PrEP use and whose annual salary was more than €60 000, we identified an increased STI risk [univariable IRR = 1.31 (95% CI: 1.03–1.66) p = .030) (Table 4). However, this finding did not remain significant in the multivariable model [IRR = 1.26 (95% CI: 0.97–1.63) p = .080].
Univariable and Multivariable Poisson Regression of Sexual Behavior and Sociodemographic Covariables Potentially Affecting the Risk of Developing Sexual Transmitted Diseases in Individuals with a Previous Pre-Exposure Prophylaxis Use (n = 308)
Adjusted model for PrEP use, self-assessed risk behavior, anal sex without condom use, health insurance, relationship status, drug use, receiving payment for sex, and region of origin. Data are no. (%) of patients, unless otherwise indicated. * p values (< 0.05) in bold depict significant results. †At least once per month, ‡GHB/GBL, mephedrone, crystal meth, cocaine or ketamine.
Univariable and Multivariable Poisson Regression of Sexual Behavior and Sociodemographic Covariables Potentially Affecting the Risk of Developing Sexual Transmitted Diseases in Individuals Before Pre-Exposure Prophylaxis (n = 375)
Adjusted model for PrEP use, self-assessed risk behavior, anal sex without condom use, health insurance, relationship status, drug use and receiving payment for sex. Data are no. (%) of patients, unless otherwise indicated. * p values (< 0.05) in bold depict significant results. †At least once per month, ‡GHB/GBL, mephedrone, crystal meth, cocaine or ketamine.
Univariable and Multivariable Poisson Regression of Sexual Behavior and Sociodemographic Covariables Potentially Affecting the Risk of Developing Sexually Transmitted Diseases in Individuals with a Previous Pre-Exposure Prophylaxis Use and Before Pre-Exposure Prophylaxis (n = 686)
Adjusted model for relationship status, sexuality, PrEP use, self-assessed risk behavior, anal sex without condom use, receiving payment for sex, and health insurance. Data are no. (%) of patients, unless otherwise indicated. * p values (< 0.05) in bold depict significant results. †At least once per month, ‡GHB/GBL, mephedrone, crystal meth, cocaine or ketamine.
Estimation of PrEP users in Germany
To understand the level of PrEP uptake in response to accessible and affordable PrEP in Germany, we used data from Kölsche Blister GmbH. Overall, between 1st October 2017 and 31st March 2018, 3,447 individual users with one or more Blister-PrEP prescriptions were identified. This enabled us to assess in which city the largest PrEP demand was recorded. When comparing the cities, the largest request for PrEP was in Berlin (47.4%), followed by Cologne (11.3%) and Munich (11.2%), which is in line with previous estimates on MSM inhabitants in these cities. 13 In other big cities, such as Hamburg and Frankfurt (Main), the request for PrEP was much lower, that is, 6.9% each. In the remainder of German cities, the request was below 3%. The most participants of the questionnaire also lived in Berlin (36.6%), Cologne (9.0%), and Munich (7.3%). Only 31.9% lived outside the 10 biggest cities in Germany. 14
We next assessed changes of PrEP uptake in Germany over time. Based on prescription requests sent by the pharmacies, we observed that the number of PrEP users (u 1) who have acquired at least one PrEP package linearly increased during the whole period of the study (Fig. 1). We recorded only one exception to the linearity at the end of December coinciding with Christmas and New Year's Eve (days 90–110), where we observed a slight dip. Overall, there was an increase of 18.51 ± 0.09 new persons on PrEP per day with no signs of slowing down in the first 6 months. This indicates that there is no perceptible tendency of u 1 to reach a maximum value and thus no total number of PrEP users for the population of Germany or within MSM can be predicted accurately.
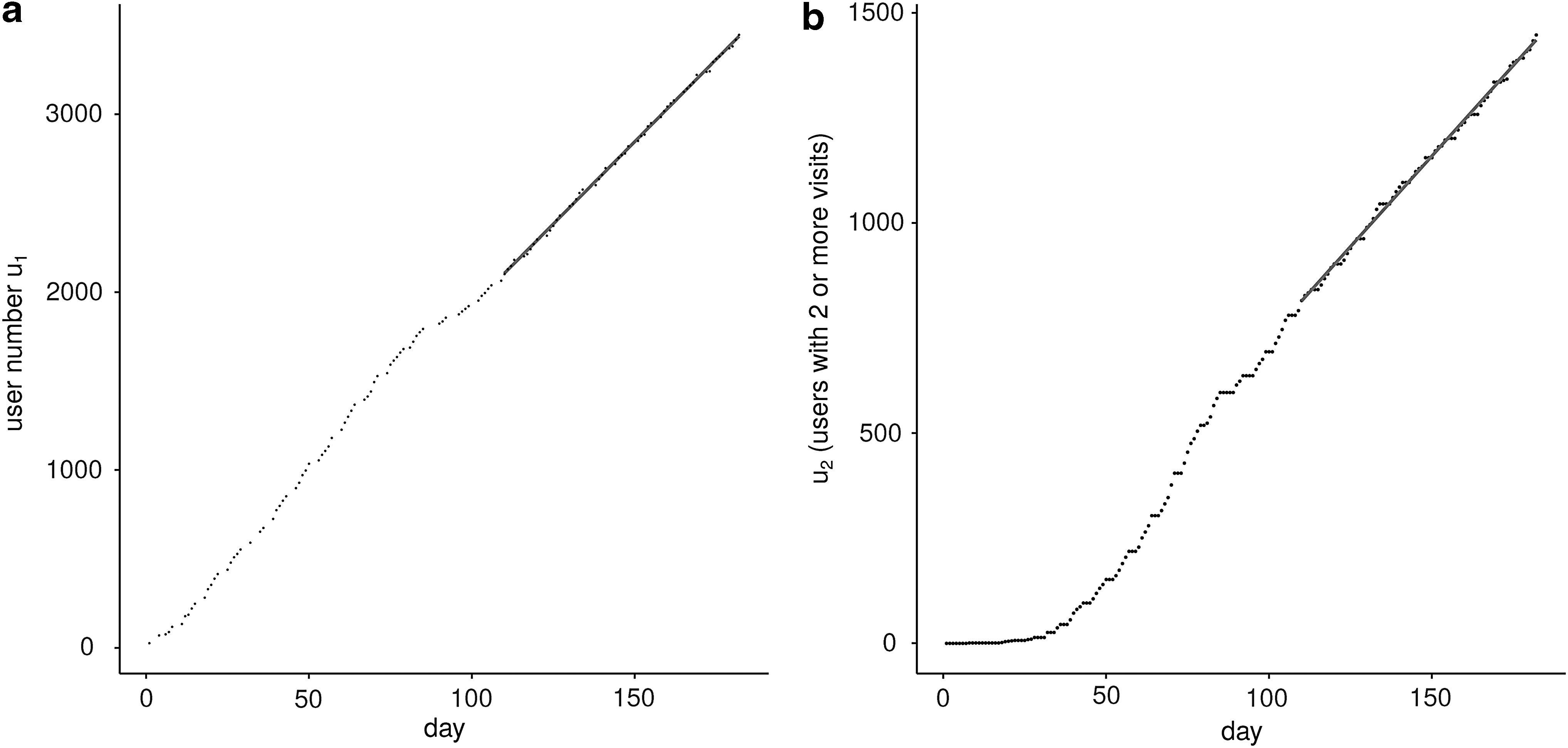
We investigated how PrEP use for each individual changed over time using the time of prescription refill information, which was anonymously collected at the Kölsche Blister GmbH. Using these data, we observed that 38.4% (n = 1,325) of all PrEP users obtained PrEP only once during the period of the study and did not refill their prescription a second time. Only a minority of 11.1% (n = 384) refilled their prescriptions without any interruption. In addition, 29.8% (n = 1,027) of PrEP users refilled PrEP at least twice, but not as often as a continuous PrEP use would require.
Using all the available data, we next estimated the potential future number of PrEP users in Germany. To address this, we first excluded the described dip and used only data after the dip as the data overall appear to better describe the tendency of PrEP user development (Fig. 2) assuming that every PrEP user took a dose on a daily basis.
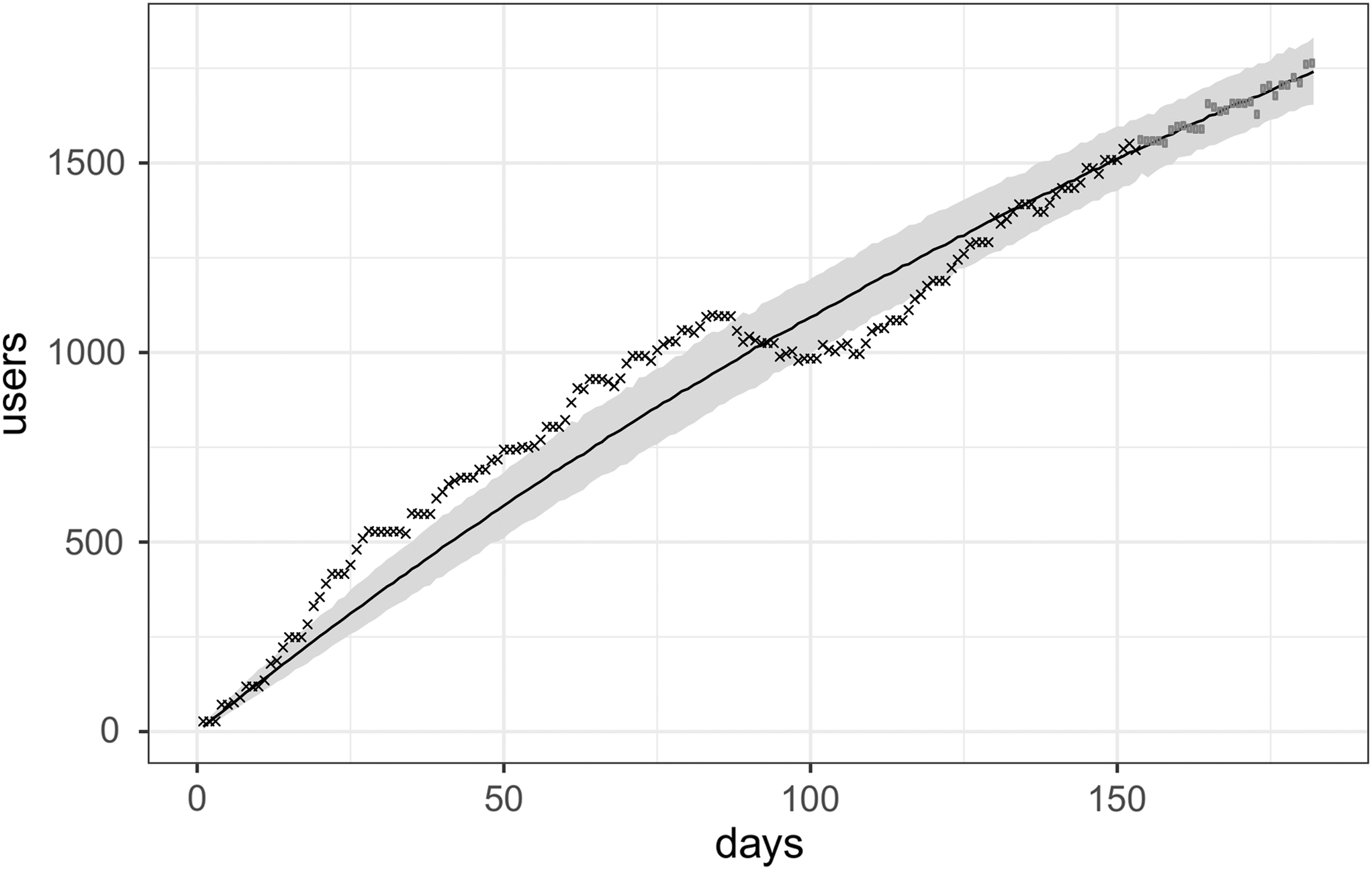
Fit of exponential convergence model exclusively using data (gray points) after the dip region. Data up to the dip region (black crosses) are not considered in this second model. The black line is the median of the probability distribution of u(t). The gray area covers 95% of the probability of u(t).
While the increase in PrEP users was linear and future use of PrEP users could only be estimated cautiously, we found a maximal PrEP user value of n = 3,887 (95% CI: 2,518–7,616) using an exponential convergence model. However, this model assumes a daily PrEP intake. The value also should not be mistaken with 3,447, which is the number of all PrEP users registered in the Kölsche Blister GmbH (continuous and on-demand PrEP use). To determine the time a plateau of PrEP users would be reached, we estimated the time t 0.95, defined as time when number of PrEP users crosses 0.95 umax, which was 299 days (95% CI: 160–692). However, observed irregular PrEP usage and wide credible intervals warn against being overly confident in our estimates.
Discussion
In this study, we followed PrEP uptake in Germany in the first months after PrEP became affordable. We also assessed differences of reported sexual behavior of individuals before and after taking PrEP and estimate current and future number of PrEP users in Germany.
Our study demonstrates that PrEP users in Germany were predominantly MSM, which indicated substantial level of self-assessed risk. This suggests that this study covered a substantial proportion of people eligible for PrEP. Many of the individuals reported behaviors that might put them at risk for HIV infection such as previous PEP use, condomless anal intercourse with multiple partners, and high self-reported STI diagnoses. Low self-reported risk of HIV infection when taking PrEP indicates that PrEP itself was considered an effective prevention method.
We also found a relatively high portion reporting consumption of drugs, including poppers, ecstasy, GHB/GLB, ketamine, amphetamine, or cocaine. This confirms previous findings that PrEP generally attracts those men who are most likely to benefit from it. 1
The individuals who were obtaining PrEP were overwhelmingly well-educated MSM (with at least bachelor's degree) of German descent with above the German median gross income of 39,612€ for males in 2016. 8,9 Only 18.7% (n = 128) had a low annual income, which was categorized as earning less than 30,000€, since the minimum wage in Germany in 2018 was 23,242€ and the lowest amount to choose in our questionnaire was “below 30,000€.” 15 Moreover, despite much lower costs of PrEP comparing to the original (over 90% reduction), mostly individuals with above median income have obtained PrEP, suggesting that at the time of the study, there was a substantial number of MSM who did not obtain PrEP possibly due to financial reasons, even though they would have benefited from the prevention method.
Estimates suggest that 3.5% of the German sexually active men are MSM, 13,16 of which about 10% would probably benefit from PrEP. 17 The estimate of the ministry of health suggests that about 10,000 individuals will make use of PrEP, which is well below the number of individuals who could benefit from PrEP. Thus, one important issue is that individuals who are marginalized, stigmatized in their sociocultural environment, or economically not able to obtain PrEP will not make use of this prevention method. 18 –20 Indeed, despite the fact that about 25,000 transgender people live in Germany, 21,22 none has finished our questionnaire. Their substantial risk of HIV infection was proven in many studies, 20 which could suggest that it is an underrepresented at-risk group. However, none of these studies was conducted in Germany. These show a medical need that other high-risk groups still need to be reached.
In our Poisson regression analyses, we did not find any important correlation between recent STIs and selected characteristics. Only age of 50 or higher, a relationship, and use of EDM were correlated with a lower STI risk, which is suggestive of potentially lower frequency of sex in individuals with these characteristics. Moreover, the lower STI risk reported by EDM users might also be related to a lower risk of STI acquisition during insertive compared with receptive intercourse. Although both were not directly assessed in the questionnaire, an interesting finding is the increased STI risk among individuals who indicated previous PrEP use and had an annual salary more than €60,000. However, these findings may be due to a reporting bias. Indeed, we observe an overrepresentation of individuals with higher salary and higher education compared to the general population in our study. Furthermore, before PrEP became available at affordable costs in Germany, a fraction of individuals had obtained PrEP from outside sources in the past, such as online pharmacies from the United Kingdom or others. We were able to demonstrate a considerable demand for PrEP based on the rapid growth of the number of prescriptions. This finding reinforces the importance of a feasible distribution system. Given the large increase of PrEP use in Germany once it became available at lower costs supports the idea that costs may be an important barrier for widespread implementation of PrEP in Germany. 23 The German ministry of health can therefore be applauded, as it has reacted and made PrEP reimbursable through the statutory health insurance from autumn 2019 onward. 24
In 2017, a reduction of estimated new infections in MSM from 2,100 (in 2016) to 1,700 was seen and it has been suggested that this was mainly due to TasP efforts. 25,26 It will be therefore interesting to see how additional HIV prevention methods will change the German HIV epidemic.
A concerning finding of the PrEP rollout in Germany is that only 11.1% of all individuals appear to take PrEP continuously. In contrast, however, 80.8% PrEP users claim to have taken all pills as planned. Even though the current German guidelines suggest taking PrEP daily, many PrEP users do not appear to follow these recommendations. 7 The exact explanation of these discrepancies requires further research. However, this could explain why we found in our estimates that 3,887 (95% CI: 2,518–7,616) people could be using PrEP in the future. Since this was based on the assumption of a daily PrEP use, the real future number of PrEP users might be much higher.
Our study has some limitations. As with every survey-based study, recall bias, social desirability bias, or participation bias could have occurred. Moreover, our results on STIs are based on voluntary self-report, not clinical tests, and included STIs diagnosed over lifetime. We used this method to reduce the recall bias, but it may have blunted the results. Moreover, the amount of pharmacies that distributed PrEP from Kölsche Blister GmbH (DAH2KA pharmacies) was limited at the beginning of the study and not present in some parts of the country. However, they covered the most relevant cities for this study, where MSM communities are the largest. An important disadvantage regarding PrEP users of non-German origin living in Germany is that our questionnaire was available only in German.
Despite these limitations, this study contributes to a better understanding of the importance of an affordable PrEP distribution system for PrEP rollout, which will have a positive effect on the efforts to decrease the number of new HIV infections in Germany and hopefully other countries.
Footnotes
Acknowledgments
We are grateful to the DAH2KA e.V. and all pharmacies that helped us in collecting the data.
Author Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was received for this article.