
Abstract

Editor: Recent data from clinical trials highlight the efficacy of a two-drug strategy with lamivudine (3TC) plus dolutegravir (DTG) as first-line regimen in treatment-naive HIV-infected people living with HIV (PLWH). 1 PLWH with transmitted resistance mutations, however, were not included in the two GEMINI trials and thus no data are available on the efficacy of such regimens in PLWH with primary resistances.
In a recently published report, 2 we described our initial experience in a small cohort of treatment-naive PLWH starting 3TC plus DTG in clinical practice. We would like to further analyze the case of a 23-year-old subject with Y188C and D232N resistance mutations starting 3TC+DTG.
The D232N mutation, in particular, is a nonpolymorphic mutation selected in patients previously exposed to raltegravir 3 and has been related to potential resistance to first-generation integrase inhibitors (INIs) raltegravir and elvitegravir.
The subject was diagnosed with HIV infection in March 2019, with a peak HIV RNA value of 114,866 copies/mL and a nadir CD4+ cell count of 328 cell/mm3. Genotypic test was also performed, showing the mentioned resistance mutations. He subsequently started the two-drug regimen with a rapid decline in HIV RNA, reaching 48 copies/mL after 3 weeks from treatment initiation. His HIV RNA load became undetectable after 8 weeks and as of today, after 24 weeks, it is still undetectable. We also observed a steady improvement in immunological parameters; after 24 weeks his CD4+ cell count was 1,091 cell/mm3.
Given the presence of the transmitted resistances, we further investigated the subject's virological status by evaluating total HIV-1 DNA levels, a marker of low-grade inflammation and viral reservoir dynamics. 4 In our patient, baseline HIV-1 DNA quantification was 3.00 log10 copies/106 leukocytes. Initial decay was sharp, as HIV DNA levels decreased to 2.69 log10 copies/106 leukocytes after 4 weeks of treatment and to 2.37 log10 copies/106 leukocytes after 8 weeks (Fig. 1).
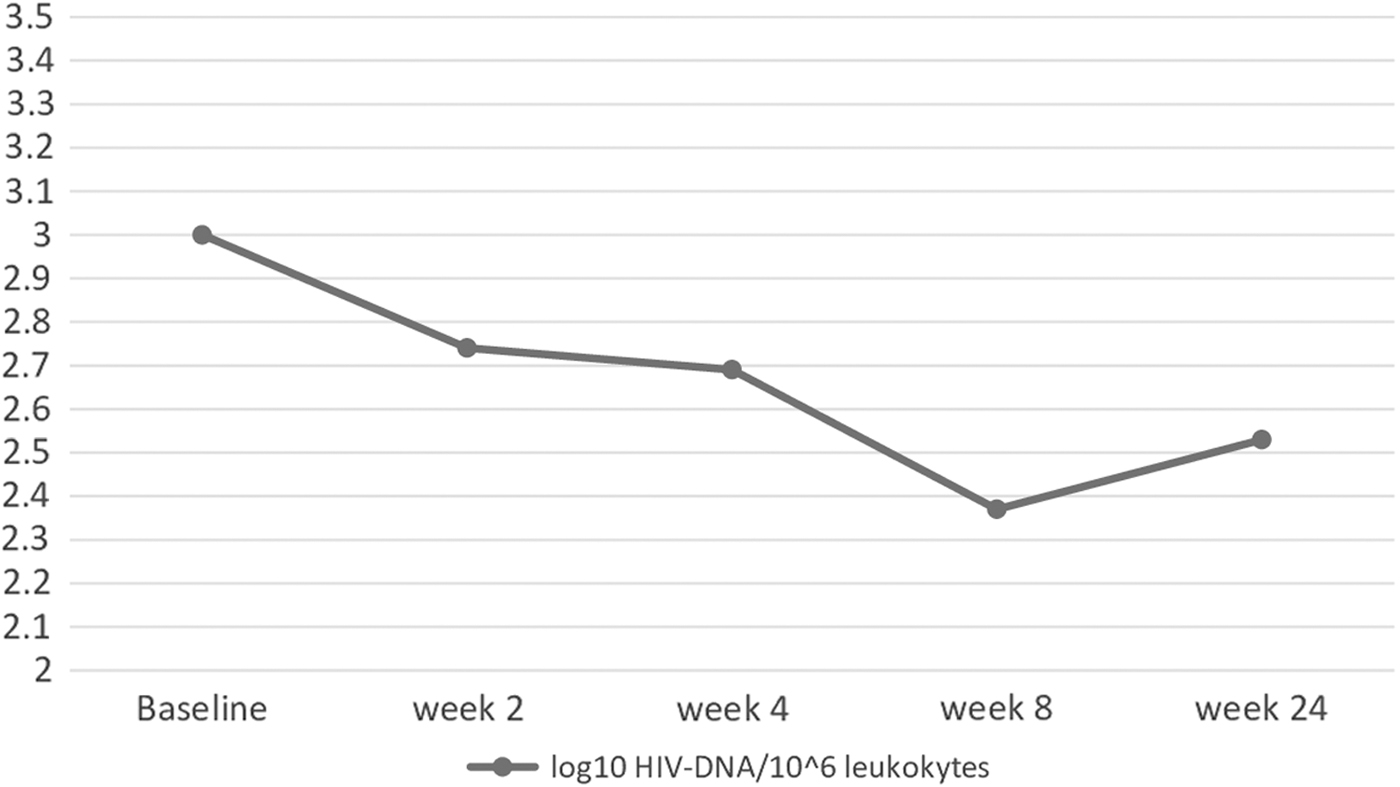
HIV-1 DNA decay in our subject.
After 24 weeks, patient's HIV-1 DNA load was 2.53 log10 copies/106 leukocytes.
3TC+DTG as first-line regimen resulted noninferior to a standard three-drug regimen in the GEMINI trials, 1 opening the door to a new era in the treatment of HIV infection. Clinicians, however, in their routine practice manage patients who rarely meet the trials' inclusion criteria.
It has been more than a decade since the introduction of the first-generation INIs, and resistance mutations to this class of antiretrovirals are no longer a rare finding. 3TC+DTG has already shown its high genetic barrier in treatment-experienced subjects and this case adds more evidence on the safety of this two-drug strategy. To the best of our knowledge, this is the first work describing the efficacy of a first-line regimen with 3TC and DTG in a subject with transmitted resistance to INIs.
Total HIV DNA represents a clinically relevant marker, independent of CD4+ cell count and HIV RNA; it also reflects treatment efficacy more exhaustively than HIV RNA, being related to residual viremia and low-level inflammation. No data are currently available regarding the decay of HIV DNA with 3TC plus DTG in treatment-naive PLWH; in our case, after treatment initiation, we observed a decrease of over 0.6 log10 copies after the first 8 weeks. Such a decrease is in line with what was observed in treatment-naive patients starting a “standard” three-drug regimen, 4 suggesting comparable efficacy in reducing the level of proviral HIV DNA. Further studies with a larger population and a longer follow-up are needed to fully understand the clinical implications of such finding.
Footnotes
Author Disclosure Statement
No competing financial interests exist.
Funding Information
G.B. received travel grant from Gilead. A.B. has received nonfinancial support from Bristol-Myers Squibb and ViiV Health care, and personal fees from Gilead Sciences. S.D.G. was a paid consultant or member of advisory boards for Gilead, ViiV Health care, Janssen-Cilag, Merck Sharp & Dohme and Bristol-Myers Squibb. A.C. declares no conflicts of interest. This study was performed as part of our routine clinical activity.