
Abstract
Human immunodeficiency virus (HIV) infection results in gut microbiota alteration and this is associated with immune activation and chronic inflammation. The gastrointestinal tract is a primary site of viral replication and thus HIV-induced loss of T-helper (Th) cells in the gut causes impairments in intestinal barriers, resulting in disruptions in intestinal immunity and precipitating into gut dysbiosis. Here, we show that late HIV diagnosis can negatively affect the immunological, virological, and clinical prognosis of the patients with its higher implication at an older age. Further, the review indicates that antiretroviral therapy affects the gut microbiota. We discussed the use of probiotics and prebiotics that have been indicated to play a promising role in reversing gut microbiota alteration in HIV patients. Though there are
Introduction
More than 36.9
General Characteristics of Included Studies in Gut Microbiota Alteration Among HIV Patients
Values are shown as amean (SD), bSD, cmedian (IQR) for age.
BPB, butyrate-producing bacteria; CD, cluster of differentiation; HC, healthy control; HIV, human immunodeficiency virus; INR, immune nonrespondent; IQR, interquartile range; IR, immune respondent; oIR, optimal immune responder; RA, relative abundance; SD, standard deviation; sIR, suboptimal immune responder; VU, untreated.
Alteration of gut microbiota among HIV patients
Human GIT is a crucial regulator of T cell homeostasis and is intricately involved in the maturation of the immune system and maintaining the mutual co-existence of host and microbe. 9 However, changes in their diversity and population were associated with CD4+ T cell counts and immune activation in HIV patients. 10,11 Lu et al. investigated the association between microbiota and CD4+ T cells recovery in HIV patients, and they showed the relative abundance of Faecalibacterium prausnitzii and Subdoligranulum spp. to have a connection with CD4+ T cell counts as evident by persistent depletion of CD4+ T cells with subsequent immune unresponsiveness. 11
In HIV patients, the viral level has an impact on the gut microbiota dysbiosis 3 as suggested during acute and early HIV infection, when there was a CD4+ selective depletion of T cells in the distal GIT with its mucosa serving as a site of active HIV replication. 12 Further, a study on the effects of HIV viremia on the gastrointestinal microbiome of young homosexual men identified variations in the microbial composition depending on the level of viremia. It was indicated that low levels of viremia (HIV RNA <200 copies/mL) had distinct microbial signatures from those who were HIV patients, but there was an undetectable viral load (HIV RNA <20 copies/mL). However, those with low-level viremia can still have microbial translocation and inflammation. In this group, depletions in Brachyspira, Campylobacter, and Parasutterella were noticed. However, HIV viral load-suppressed participants (HIV RNA ≤200 copies/mL) had depletions in Barnesiella, Helicobacter, and Brachyspira relative to HIV-negative subjects. 3
It is, therefore, not surprising that different patterns emerge when considering gut microbiota of HIV patients and healthy controls. Recently, a cohort study on the diversity of gut microbiota between HIV patients and healthy controls demonstrated that HIV patients have a significant decrease in Clostridia class and an increase in Gammaproteobacteria class. 13 Lu et al. also investigated the changes in mucosal microbial composition and reported more Prevotella and fewer Bacteroides in HIV patients. 11 In addition, during the bacterial profile from fecal microbiota by pyrosequencing the gene encoding 16S ribosomal ribonucleic acid (16S rRNA) in 21 of chronic HIV patients and 16 seronegative individuals, the relative abundance of Gammaproteobacteria, Enterobacteriales, and Enterobacteriaceae in the Proteobacteria phylum; Erysipelotrichi, Erysipelotrichales, and Erysipelotrichaceae in the Firmicutes phylum was significantly enriched in cases, whereas that of Alistipes and Rikenellaceae was depleted. 14
A difference has been also observed in the operational taxonomic unit abundance between healthy controls and HIV patients, with the most abundant families showing Ruminococcaceae and Prevotellaceae in healthy controls and HIV patients, respectively. An increased proportion of Preovtella copri (the most prevalent Prevotella species in the human gut associated with diet and disease) in HIV patients could indicate a dysbiosis of the microbiota. 15
On the other hand, gut microbiota and/or age-related microbial changes were linked to an increased gut permeability with age that results in age-associated inflammation. 16,17 Thus, an increase in the permeability of the intestinal mucosa, which could allow bacteria, bacterial toxins, and small molecules to leak into the bloodstream, 18 is considered a major driving force of chronic immune activation. 19 In late-treated HIV patients, the intestinal permeability pointed toward increased absorption of high-molecular-weight molecules. Concomitantly, study participants also showed lipopolysaccharide (LPS), endotoxin core antibodies, soluble CD14 (sCD14), and interleukin (IL)-6 in their plasma. Notably, gut epithelial damage, microbial translocation, and systemic inflammation were major events reported in HIV patients in relation to their old age coupled with late HIV treatment. 20
Interestingly, HIV and age were independently associated with distinct changes in the stool microbiome, with age-related microbiome changes varying on the HIV serostatus of an individual. In a study involving older HIV seropositive people (median age 61.5 years, N = 14) and seronegative controls (median 58 years, n = 22), the abundances of Allisonella and Anaerovibrio (p < .0001) were higher and Oscillospira (p = .001) and Eggerthella (p = .047) were lower among cases compared with seronegative controls. Consequently, age-related changes in microbiome profile have been shown to be exemplified by Leptotrichiaceae, Escherichia, and Oxalobacter and the genera Butyricimonus has been shown to be significantly increased with age in HIV patients but lower with age in control groups. 21 Major findings in gut microbiota alteration are shown in Table 2.
Alteration of Gut Microbiota Among HIV Patients
16S rRNA, 16S ribosomal ribonucleic acid; FDR, false discovery rate.
Alpha and Beta Diversity
Several studies have reported HIV-related gut microbiota diversity by using alpha (α) and beta (β) diversity indicators. Alpha diversity measures species richness and evenness within samples by using different measures, such as observed species, the Shannon diversity, and the Chao1 index. 22,23 A study from Marseilles in France revealed that significant diversity changes occurred during HIV infection. The α diversity was significantly reduced in HIV individuals compared with controls as assessed by the Shannon index 13 ; however, the study by Zhou et al. showed that the α-diversity of fecal microbiota was markedly reduced compared with healthy controls and this is termed dysbiosis and is characterized by low mean counts of prevotella and Bacteroides vulgatus. 24 A prospective cohort study revealed that baseline CD4+ T cell counts were closely associated with α diversity indices of the intestinal microbiota in HIV patients. Besides, in subgroup comparisons, significantly lower α diversity indices were observed in subjects with CD4+ T cell counts <300/mm3. However, in this group, the increase in α diversity indices was significant after combination antiretroviral therapy (ART) for 15 months. On the other hand, in subjects with CD4+ T cell counts >300/mm3 and at baseline, the α diversity of the gut microbiota was slightly decreased. 25 On the contrary, a study on alterations involving α diversity using Shannon and Simpson indices in the fecal microbiota of HIV patients showed no significant difference among cases and controls, despite the higher Shannon index and lower Simpson index in patients with HIV. 26
Moreover, the β diversity, an analysis of inter-individual variability within the samples of study groups, 27 showed substantial difference in the microbiota of HIV patients from healthy individuals using principal component analysis and principal co-ordinate analysis. 24 In a study on the gut microbiota profile among HIV patients with diverse immune recovery profiles and in the relationship between the altered bacteria and markers of immune dysfunction, using unweighted UniFrac distance metric (p < .05), and β diversity indicated a significant change in the microbial composition among the groups. Enrichment of gut-derived Fusobacterium was associated with suboptimal immune recovery in HIV patients. 28 However, Ling et al. reported, in HIV-treated and -untreated groups by the unweighted UniFrac analysis, that the diversity of fecal microbiota in HIV patients was unaltered. 26 This might suggest the magnitude and level of significance of HIV infection compared with its treatment regarding alteration of the gut microbiota diversity. Further, one could also speculate on ART having general and yet microbial population-level effects compared with HIV infection-mediated immune response effects on the microbial diversity.
Further, β diversity analysis among homosexual HIV patients and healthy controls indicated significant differences between bacterial compositions due to HIV infection-driven gut microbiota dysbiosis. 11 A study by Dinh et al. comparing the gut microbiota of HIV patients with healthy controls using pyrosequencing technology revealed significant differences in the community composition of the microbiota assessed by β diversity (p < .05) measures. 14
Inflammation and Translocation Markers
Persistent immune activation is one of the main predictors of HIV disease progression. 26 This can be explained by the fact that the gut microbiota is essential for immune homeostasis; so disruptions in intestinal immunity can precipitate gut dysbiosis, which may create an opportunity to induce chronic inflammation in the mucosa and periphery. 29 Moreover, the microbial diversity was shown to be compromised in HIV infection and this is associated with immune dysfunction and chronic inflammation. 30 As a fact of advanced disease and AIDS that are associated with immunodeficiency, which can result in opportunistic infections and alterations in the microbiome, 31 inflammation, immune activation, and opportunistic infection in HIV patients remain as common clinical problems, which is in spite of the available ART. 5
A cross-sectional study on butyrate-producing bacterial (BPB) species in colonic biopsies and stool involved 18 untreated chronic HIV patients and 14 uninfected as a control. In this study, it was identified that colonic mucosal BPB species were lower in abundance among untreated HIV patients compared with controls. In untreated groups, the abundance of Roseburia intestinalis, a dominant BPB, was decreased. It is known that the relative abundance of R. intestinalis is inversely correlated with levels of plasma LPS and sCD14—indicators of microbiota translocation and monocyte activation—as well as with plasma tumor necrosis factor alpha (TNF-α) and IL-10 levels, which are known as inflammation markers. 32 Dinh et al. examined possible correlations between the relative abundance of taxa and markers of microbial translocation and systemic inflammation, and they reported significant positive correlations between the relative abundance of both Enterobacteriales and Enterobacteriaceae and sCD14 levels (p < .01). 14
The microbiota has impact on shaping the development of the gut immune system whereas its alteration is closely associated with immune dysfunction in HIV patients. Increased immune activation and inflammation are characteristics of HIV infection. Nonetheless, studies on the concentration of plasmatic inflammatory cytokines and LPS binding protein (LBP) demonstrated no significant differences among HIV patients and uninfected, HIV patients showed increased sCD14 plasma levels when compared with uninfected groups (p = .02). 15
Gut microbiota is related to the translocation marker and systemic immune inflammation. A study from Zhejiang, China, revealed that the systemic inflammatory cytokines, such as TNF-α, interferon gamma (IFN-γ), and IL-6, were correlated with the abundance of genera Phascolarctobacterium (p = .014), Megamonas (p = .006), Dialister, and Clostridium XIVb, except for Prevotella. For prevalent genera in the healthy controls, Dialister was positively correlated with IL-22 (p = .000) and IFN-γ (R = p = .035), and Clostridium XIVb was negatively correlated to IFN-γ (p = .004). 26
HIV infection causes impairments in intestinal barriers, which results in an imbalance between aerobic and anaerobic gut microbiota. Dubourg et al. also concluded with dysbiosis in the association between the relative abundance of bacteria families or species (anaerobic and aero tolerant) and levels of biomarkers in HIV patients. The study group revealed that Ruminococcaceae and Faecalbacterium, especially Ruminococcus bromii and F. prausnitzii, were inversely correlated with inflammation or immune activation markers when depleted. On the contrary, Enterobacteriaceae and Entrobacteria (especially Escherichia coli and Enterobacter aerogenes) and the Enterococcaceae family (Enterococcus faecalis and Enterococcus faecium) were positively correlated with these markers when enriched 13
Up to date, CD4+ T cell count remains the primary laboratory marker used in the follow-up of disease progression in HIV. 29 Lee et al. identified that CD4+ T cell activation (canonical loading, CL = 0.923) and CD4+ Tregs (CL = 0.639) were positively correlated with an increase in the abundance of Fusobacterium (CL = 0.951) but negatively correlated with Lactobacillus (CL = 0.361). In addition, the proportion of naive CD4+ T cells (CL = 0.509) was negatively correlated with Fusobacterium (CL = −0.951) whereas it was positively correlated with the relative abundance of Lactobacillus (CL = 0.361). 28
Moreover, a recent study revealed that old age categories are the prominent factors on inflammation and immune activation markers, which is supported by a recent study. The results show that HIV old aged patients had higher levels of sCD163 (p = .019), sCD14 (p = .0006), and soluble tumor necrosis factor (sTNF)R2 (p = .0034) compared with uninfected controls. The major differences were noted in patterns of associations of microbiota and inflammatory biomarkers. For example, among HIV patients, Escherichia and Subdoligranulum were positively correlated with sTNFR1 and sTNFR2; whereas Bifidobacterium with TNFR1 and IL-6, and Prevotella inversely correlated with sTNFR1 levels. 21 Moreover, in the older patient populations (≥55 years), recent findings showed that the levels of anti-inflammatory cytokines IL-1RA, T cell cytokine IL-2, and eosinophil maturation factor IL-5 inhibitors were reduced in long-term controlled HIV patients. 33
Associated Factors Affecting Microbiota in HIV Patients
A number of studies showed the possible factors associated with alteration of microbiota among HIV patients, and they are presented herein along with a discussion of the two main factors: late diagnosis in old age and ART on the composition and diversity microbiota among HIV patients.
Late diagnosis of HIV in old ages
According to the United States Centers for Disease Control and Prevention (CDC) report in 2016, 35% of people aged 50 and older received a diagnosis late in the course of the infection. 34 The late diagnosis in HIV can affect the immunological, virological, and clinical status of patients. In such a condition, management of patients is challenging and carries a less favorable outcome. 35 In a study done in India, the majority, 21 (47.7%) of deaths were reported within 3 months of starting ART. 36 In Ethiopia, patients who started ART after they developed AIDS-related illness were 1.4–11.2 times more likely to die than patients who started as early as WHO stage I or II. 37 Moreover, a study by Luma et al. showed mortality and opportunistic infections to remain significantly higher in lately diagnosed patients. 38 Older HIV patients, defined as HIV-infected individuals aged 50 years and older, carry the higher risk of late diagnosis, for example, a prospective multicenter cohort study in older HIV-infected people was able to show that 965 (68.2%) patients were diagnosed at age 50 or older. 39,40
The incidence of infection and noninfectious comorbidity is also higher in HIV-infected people compared with HIV-negative groups, where the duration from infection to diagnosis in HIV is a strong predictor. 41 In addition, late presentation for HIV diagnosis exhibits an increased risk for age-related noninfectious comorbidity and multiple morbidity compared with individuals with early presentation for HIV diagnosis and matched HIV-negative individuals. This is also relevant in patients older than the age of 50 years. 42 In this regard, a retrospective cohort study revealed that HIV-positive older patients were more likely to have hepatitis C coinfection (p = .001), hypertension (p < .001), diabetes mellitus (p < .001), higher hepatitis B concentration (p = .008), and higher serum creatinine (p < .001) compared with young HIV-positive patients. 43 Asher et al. demonstrated that the older patients had a higher mortality rate (21% vs. 3.5%; p < .001), lower CD4+ cell counts (381–228 vs. 483–261 cells/mL; p < 0.001), higher viral load above 100,000 copies/mL, and higher AIDS-defining illness compared with younger patients at the time of diagnosis. 35
In old age, the manifestation of age-related chronic inflammation and dysregulated immune activation are reflected as primary evidence and constitute an expected mechanism of immunosenescence (a biological phenomenon of gradual deterioration of the immune system occurring in elderly individuals). 44 Different scholars reported that old age population groups have decreased intestinal function compared with younger age groups. As a result, digestion, nutrient absorption, and immune activity are impaired. 45 In addition, aging has been associated with decreased production of IL-2 and its receptors, which results in compromised T cell functionality, reduced memory T cell population with an underlining reason of reduced CD4+ T cells response in elderly patients to be a result of involution of the thymus gland with decreased productivity. 35 Apart from aging, changes in the composition of gut microbiota of the old age population could be associated with the decline of the general state of health with malnutrition and an increased need for medication, such as antibiotics and nonsteroidal anti-inflammatory drugs. 46
Immunologically, older ages manifest as elevated serum levels of neopterin, C-reactive protein (CRP), IL-6, sTNFR-1, and sTNFR-2, which are associated with frailty, disability, and mortality. 16 The immune system at the time of HIV diagnosis was also shown to be significantly impaired in older patients, with 31% of older patients tested having a CD4+ cell count of less than 50 cells/μL compared with 15% of younger patients. 35 In HIV, infection through direct immune activation in both innate and adaptive immunologic pathways was considered responsible for accelerated immunosenescenc. 41,47 The main target cell categories in HIV infection were shown to be CD4+, dendritic cells, monocytes/macrophages, thymocytes, and microglial cells. 44
As shown in Figure 1, change in the composition of gut microbiota is affected due to multitude of factors including old age, HIV infection, late HIV diagnosis, ART and poor immune prognosis. 33,48 This could be due to the loss of crucial immune cells because of HIV infection and changes in the composition of microbial communities, for example, the mouth colonizing genera Fusobacteria, Lactobacillus, and multiple Bifidobacteriales were present in gut microbial communities among long-term controlled HIV patients. 33
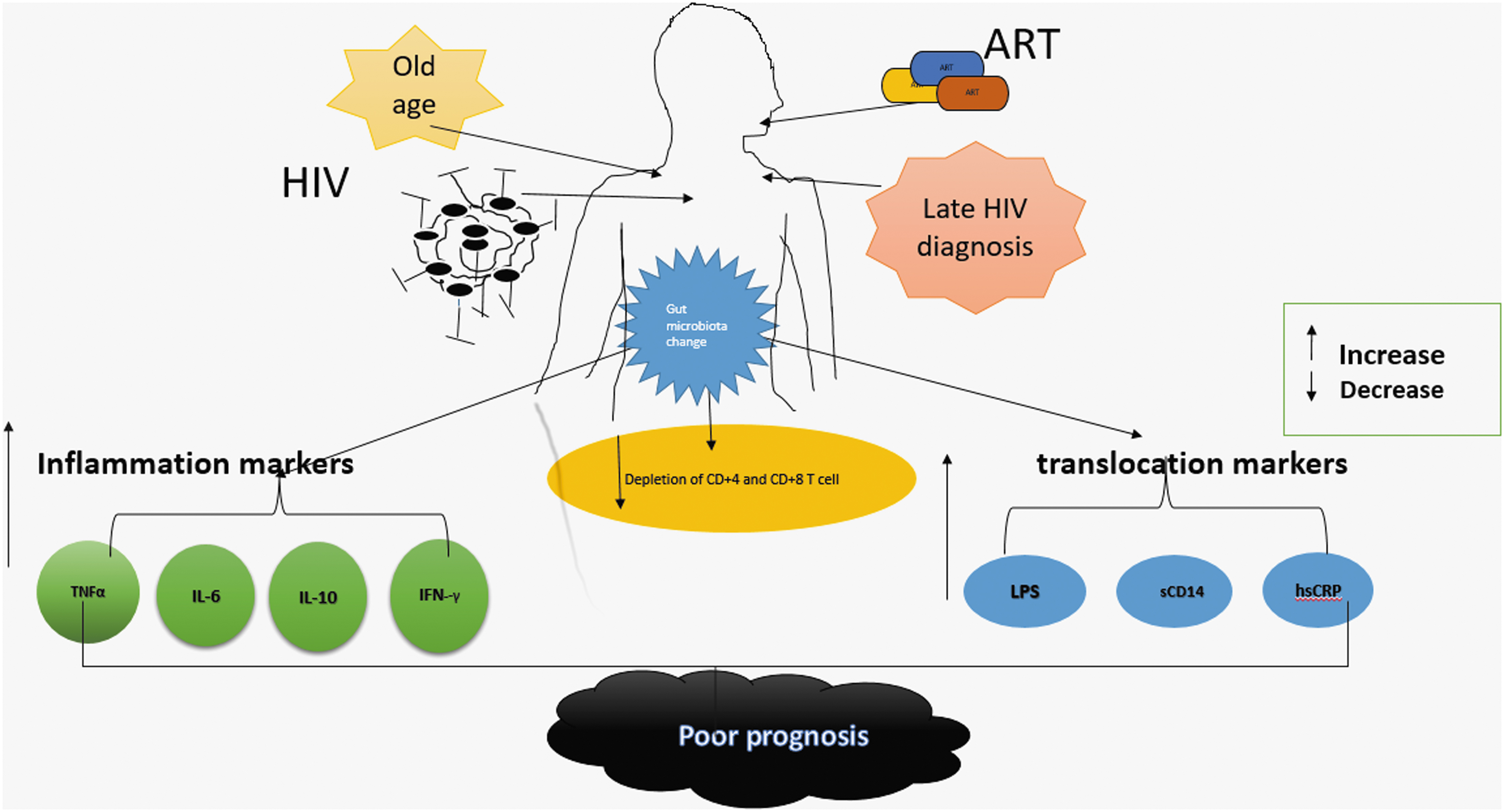
HIV infection weakens the wall of the intestine and this could create opportunities for bacteria, bacterial toxins, and small molecules to enter into the bloodstream, which may cause systemic inflammation. In addition, HIV damages the GALT and causes depletion of T cells (CD4+ and CD8+). Although ART affects the gut microbiota diversity, late HIV diagnosis and old age are exacerbating factors for the disturbance of the gut community. Subsequently, translocation of gut microbiota takes place and evidence shows that probiotics and prebiotics have some promising effect on the restoration of gut microbiota as well as in the decrease of inflammation markers and immune cell activation. ART, antiretroviral therapy; CD, cluster of differentiation; GALT, gut-associated lymphoid tissues; HIV, human immunodeficiency virus.
ART and gut microbiota
Antiretroviral drug discovery and development for treatment of HIV infection has led to fewer AIDS-related complications and better prognosis for HIV-infected people. 49 However, ART is shown to affect gut microbiota diversity and nowadays findings emerge with different views. Very recently, a study has demonstrated that active fraction of microbiota richness decreased in ART-treated patients compared with untreated patients and health controls. 50 However, current literature on HIV infection and response to ART has been shown to influence the composition of the microbiota. In a cohort of 26 HIV patients including 10 suboptimal immune responders ( = CD4+ T-cell <350 cells/μL) and 16 optimal immune responders ( = CD4+T-cell >500 cells/μL), after a minimum of 2 years on suppressive ART, suboptimal responders showed a significant increase in the relative abundance of Fusobacteria as compared with optimal responders and uninfected controls. Concomitantly, the study identified several differentially abundant microbial taxa and there was a notable increase in the abundance of the family Veilonellaceae and a depletion of the genus Eubacterium in other HIV patients. 28 In a study by Ling et al., alteration in the treatment effect showed a difference in stool microbiota diversity in treated and untreated HIV patients; Firmicutes and Proteobacteria were significantly less abundant in ART-treated patients (p < .05). 26
However, in HIV patients after a short-term highly active antiretroviral therapy (HAART), the diversity and composition of fecal microbiota were not shown to be completely restored. 13,24,26 A cross-sectional study revealed that there was partial restoration of gut microbiota in patients receiving HAART compared with those who did not receive it; levels of Bacteroides, Blautia, and Faecalibacterium displayed a remarkable increase, whereas Roseburia and Rminccoccaceae showed no change. 24
Probiotics and Prebiotics
Probiotics commonly refer to viable microorganisms that originated from the gut and they have beneficial health effects on consumers. At a different time, various explanations of probiotics have been given, and several hypotheses were elucidated regarding series of their evolvements with regard to the definition of probiotics. Recently, it has been defined as “live organisms that, when ingested in adequate amounts, exert a health benefit to the host.” 51 –54 Probiotics are able to enrich the human digestive system with good microbes that are able to neutralize the harmful ones and restore the balance between bacteria such as Lactobacilli, Streptococci, Clostridia, Coliform, and Bacteroides. 55 It has been shown that after 6 months of probiotics supplementation, there was a significant increase in specific bacteria genera compared with the baseline (p < .05). 56 Similarly, a study by d'Ettorre et al. revealed that there was a significant increase in Bifidobactria spp. (p < .019) after probiotic intervention. 57 It also exerts beneficial effects in old age patients. 46,58 –60 Thus, probiotic administration might also promote the reversing of gut damage in HIV-1 infection. 54
Moreover, as revealed by four earlier studies, there were changes in T cell activation, that is, the frequencies of CD4+ cells simultaneously expressing HLA-DR and CD38 significantly decreased after supplementation with probiotics. 55,57,61,62 Thus, probiotics may confer a health benefit on the host by the modulation of the immune system and controlling inflammatory gut disorders. 54
Likewise, the definition of prebiotics has been discussed and refined several times to accommodate emerging knowledge. 53 Currently, the prebiotic concept has been expanded, in part, because of a far more in-depth understanding of gut microbiome and sequencing studies, which has improved scientific community knowledge on the composition of the microbiota and enabled identification of additional substances influencing colonization. 53,63 Recently, in 2017, academic experts in the field of prebiotic research reached a consensus on the definition of prebiotics to mean a substrate that is selectively utilized by host microorganisms conferring a health benefit. 63
In humans, providing probiotics and prebiotics shows promising outcomes to maintaining and restoring the homeostasis of the gut microbial ecosystem. Given this, a recent study has revealed that in frail elderly groups, the Ruminococcaceae (Clostridium cluster IV), Parabacteroides, and Phascolarctobacterium were increased after prebiotic supplementation. 51,64 Likewise, prebiotics and glutamine have also been shown to exert benefits on gut microbiota and the enterocyte barrier function. Further, they ameliorated HIV-associated dysbiosis and improved innate and adaptive immunity. Indeed, in untreated HIV patients, the nutritional supplement increased the abundance of the depleted Faecalibacterium and Firmicutes (Catenibacterium, Blautia, Eubacterium) and Actinobacteria (Collinsella and Corinebacterium) phyla and it was not observed among ART-treated patients 65 The studies discussed in this review deal with the effect of prebiotics and probiotics and this is shown in Tables 3 and 4.
General Characteristics of the Included Studies on Probiotics/Prebiotics Effects
Values are shown as aSD, bmedian (range), cmedian (IQR) for age.
F, female; M, male; NA, not available.
Effect of Probiotics/Prebiotics Supplementation on Gut Microbiota Recovery Among HIV Patients
FMO, fluorescence minus one method; hsCRP, high sensitivity C-reactive protein; PCR, polymerase chain reaction.
Conclusion
It summary, the studies show that HIV infection certainly leads to alterations in gut microbiota and a worsening of patients' quality of life. Late diagnosis of HIV in old age has unpleasant outcomes and severe consequences because of immunological alterations due to the double effect of aging and HIV infection on gut microbiota. Hence, the early diagnosis of HIV plays an important role in the management of HIV-related complications. Notably, studies on the late initiation of ART and old age are seen to contribute toward such changes. The reversal of gut microbiota alterations with probiotics and prebiotics can be a promising therapeutic approach. However, further prospective studies are strongly recommended to determine the real association between old age and the late diagnosis of HIV and ART on the alteration of gut microbiota.
Footnotes
Authors' Contributions
All authors have contributed to this article equally. Conceptualization: A.A.A., Y.-G.F., R.-X.L., D.-Q.Y., B.-Z.L., H.-F.P., and T.A.L. Data curation: A.A.A., Y.-G.F., and R.-X.L. Fund acquisition: Y.-G.F., D.-Q.Y. Investigation: A.A.A., Y.-G.F., R.-X.L., and T.A.L. Method: A.A.A., Y.-G.F., D.-Q.Y., B.-Z.L., and T.A.L. Project administration: D.-Q.Y., Y.-G.F. Software: A.A.A., Y.-G.F., and R.-X.L. Writing original draft: A.A.A., Y.-G.F., and D.-Q.Y; Writing review and editing: A.A.A., Y.-G.F., D.-Q.Y., B.-Z.L., and T.A.L.
Acknowledgments
The authors thank all the authors who placed their findings online as well as those who provided data after personal communication.
Author Disclosure Statement
The authors declare that they have no competing interests.
Funding Information
This project was supported by the Natural Science Fund of Anhui Province (1608085MH174) and the program of technical support for Liuzhou (2019WT020089), which was authorized by the Chinese National Center for AIDS/STD Control and Prevention.