
Abstract
Despite the implementation of health education and free condom distribution for decades, the HIV/AIDS epidemic among older adults in China shows no sign of declining. This study aims to identify HIV transmission patterns and pathways in a rural county area and provide insight for developing effective HIV prevention strategies among older adults. Epidemiological field surveys combined with phylogenetic analysis were used to identify potential HIV transmission linkage in one rural county with a rapidly increasing HIV epidemic among older adults. A total of 160 HIV-positive individuals and their HIV-positive sexual partners diagnosed between 2015 and 2018 were recruited. Among them, 69.4% (n = 111) were diagnosed at age 50 or older, 68.1% (n = 109) were men, and 55.0% (n = 88) were married. Ninety-six participants self-reported as having been infected with HIV through commercial heterosexual behavior and 24 were infected from their HIV-positive spouse. CRF08_BC (67.0%, n = 73) and CRF07_AE (19.3%, n = 21) were the prevalent HIV stains and formed 15 clusters at distance cutoff of 0.0025. Participants diagnosed with HIV at age ≥50, those who were divorced or bereft their spouse, or infected with HIV locally were more prevalent within the 15 molecular clusters. We identified specific venues as the primary hotspot and found that commercial heterosexual contact between older men and commercial sex workers contributed to the local HIV epidemic. In rural areas with an increasing HIV epidemic, detecting HIV transmission clusters through epidemiological and phylogenetic analysis as well as designing localized HIV prevention strategies should be prioritized.
Introduction
China, the country with the largest population worldwide, is facing the challenge of population aging. The number of Chinese 50 years and older reached 430.8 million by 2017, and people in this age group accounted for 31.0% of the total population. 1 In the past, because of sexual inactivity, older adults were not considered to be at high risk of HIV infection. However, studies have challenged the stereotype of asexuality among this population. 2,3
There is growing evidence that older adults have been increasingly and disproportionally affected by HIV during the past decade in China. 4 The growth rate (136.1%) of newly diagnosed HIV-positive older adults between 2012 and 2017 is much higher than other age groups (54.9%). 5,6 Furthermore, older heterosexual men in rural areas were found to be at disproportionate risk of HIV infection, 7 especially the older male clients of low-cost commercial sex venues. 8
Songyang (SY) County is located in the southeast of Zhejiang province in eastern China. Almost 80% of the area is mountainous. By the end of 2018, the county had a population of ∼190,000 (0.3% of that of the entire Zhejiang Province), among which one-fifth of the population was 60 years and older. The real GDP per capital was 55,645 yuan (8,409 US dollars) in 2018, which ranked SY county as the 79th among 90 counties in Zhejiang province in terms of GDP. The first HIV case was diagnosed in SY County in 2006 and the number of newly diagnosed HIV cases remained <10 annually until 2011. In 2013, the first HIV-positive commercial sex worker (CSW) was diagnosed in SY County and the first HIV case who was older than 50 years. Furthermore, paralleling the increasing HIV epidemic in China, 21 HIV cases 50 years and older were diagnosed in 2016, representing a 250.0% increase over six cases diagnosed in 2014. More than 90% of newly diagnosed HIV cases were infected through heterosexual contact. However, the effects of HIV intervention strategies are hampered by lack of comprehensive information about the key population in this area and patterns of local HIV transmission pathways.
Recently, molecular data combined with targeted epidemiological investigation and public health action have been successfully implemented for identifying growing HIV transmission clusters in large-scale geographic areas 9,10 or key populations. 11,12 These studies and public health interventions shed light on the development of innovative HIV intervention strategies. Using a genetic distance (GD) threshold of low level (i.e., 0.5% or lower) can identify recent and rapid transmission clusters. Exploring the leading edge of transmission at local level will be most important to slow or prevent HIV transmission in a given area. 13
A good understanding of recent and ongoing transmission patterns is conducive to developing efficient local HIV intervention strategies. In this study, we sought to comprehensively investigate the recent HIV transmission pathway in one rural county in China with a rapidly expanding HIV epidemic among older adults, through the implementation of epidemiological field study and polygenetic analysis.
Materials and Methods
Ethical statement
Ethical approval for this study was granted by the Institutional Review Board of the Zhejiang Provincial Center for Disease Control and Prevention. Written informed consent was obtained from each participant before the epidemiological survey and the molecular analysis of the study. The design and implementation of the study followed the Declaration of Helsinki.
Study population and data collection
In this study, we recruited all newly diagnosed HIV cases in SY County (2015–2018), and HIV-positive individuals with epidemiological links to these newly diagnosed HIV patients. A total of 160 HIV-positive individuals were enrolled in our study. The identity and HIV infection status of the study participants was never revealed to their extramarital sexual partners, nor was the information resulting from the study conveyed back to the participants.
After HIV notification and consent procedures, we collected demographic information (age, gender, address, and registered place of residency [Hukou]) in combination with behavioral history associated with potential HIV exposure within the epidemiological field survey. Details of HIV-exposure history, including time and location of sexual behavior before HIV confirmation, were collected retrospectively among participants diagnosed before 2017, which then became routine survey content. To protect the privacy of the participants, all personal identifiers were removed from the study database before data analysis.
Ethylenediaminetetraacetic acid blood samples of HIV confirmation tests were collected and used for molecular analysis. All participants were treatment naive at the time of blood sampling. The plasma fraction was stored at −80°C at the Zhejiang Provincial Center for Disease Control and Prevention.
HIV screening initiative among older adults
After the outbreak of the localized HIV epidemic among older adults in 2016, the health administration of SY County initiated a HIV screening campaign for older adults, which began in May 2017. The purpose of the campaign was to identify undiagnosed HIV cases as much as possible. An opt-out HIV testing service was provided for adults 60 years and older during their physical examination, which was covered as basic public health services in rural area. The testing initiative continued in 2018 in four villages with the highest number of people living with HIV and AIDS (PLWHA), which were Xiping, Shuinan, Wangsong, and Yecheng. A total of 31,868 and 8,141 residences were administered HIV test during this initiative in 2017 and 2018, respectively. Of the people undergoing screening, 45 HIV-positive individuals were identified in 2017 (33 were newly diagnosed and 12 had been diagnosed in previous years), and 3 HIV-positive individuals were identified in 2018.
RNA extraction and amplification
HIV RNA was extracted from 140 μL of plasma using a QIAamp Viral RNA Mini Kit (Qiagen, Germany) according to the manufacturer's instructions and was subsequently subjected to reverse transcription PCR and nested PCR to generate pol fragments (HXB2: 2147–3462). The pol fragment was ∼1,316 bp in length and covered the coding region of full-length protease (PR) and the first 300 codons of the reverse transcriptase (RT). The PCR products were purified by Sanger's dideoxy chain position method and then sequenced by using five overlapping primers in an ABI 3730XL sequencer (Applied Biosystems, Carlsbad, CA).
Phylogenetic analysis
The consensus sequences were trimmed, assembled, and adjusted to Sequencher® v5.0 (Gene Codes Corporation, Ann Arbor, MI). Ambiguous bases were considered when the secondary peak was >30% of the main peak. The overall proportion of ambiguous bases was as low as 0.32% in the study. ClustalW multiple alignment and manual editing were performed using BioEdit v7.2.0 (Ibis Biosciences, Carlsbad, CA). Reference sequences covering the major HIV-1 subtypes and CRFs (including the 08_BC sequence from southeast China) were retrieved from the Los Alamos HIV sequence database (
Network construction
Pairwise GDs were computed using MEGA v6.0 based on the Tamura-Nei 93 model. The ambiguous bases were treated as gaps through pairwise deletion in the calculation of the GDs among viral sequences by MEGA. The cluster was defined according to connected network components at a distance threshold of 0.25% (0.0025 expected substitutions per site). The network was constructed by identifying pairs of sequences (nodes) and their potential transmission relationships (edges) using the visualization software Cytoscape v3.6.2.
Molecular clock analysis
We applied a Bayesian Markov chain Monte Carlo (MCMC) method as implemented in BEAST (version 1.7.5) for phylogenetic analysis of time to the most recent common ancestor (tMRCA) for CRF08_BC clusters. To allow for variation in molecular evolutionary rates among lineages and through time, we used the exponential relaxed molecular clock with a discretized gamma-distributed general time reversible substitution model. The nonparametric Bayesian skyline coalescent model was used. Analyses of 50 million MCMC generations were performed in duplicate. Evolutionary parameters were sampled every 2,000 generations and 25,000 posterior trees were retrieved. After removing 10% of burn-in and combining evolutionary parameters and trees using TreeAnnotator v1.6.2, convergence of the MCMC output was assessed in Tracer v1.6, and all parameters achieved effective sample sizes (ESSs) >200. Within these clusters, we identified strongly supported clades (i.e., posterior probability ≥0.90) of sequences, which provide evidence for onward transmission within a local area.
Data analysis
All statistical analyses were computed using Statistical Product and Service Solutions (SPSS, version 19; IBM, Armonk, NY). Frequencies and associated percentages were calculated for categorical and categorized continuous variables. The chi-square tests and or Fisher's exact tests were used to compare the difference of proportions between categories. Differences were deemed statistically significant given p < .05, and all tests were two sided.
Results
Social demographic characteristics of study participants
The social demographic and HIV clinical characteristics of the 160 study participants are summarized in Table 1. Overall, 69.4% (n = 111) of participants were diagnosed at age 50 years or older, 68.1% (n = 109) were men, 55.0% (n = 88) were married, and 62.5% (n = 120) were illiterate or graduated from primary school. A great majority (91.9%, n = 147) of participants were SY County residents, four participants were from other cities in Zhejiang province and nine from other provinces in China.
Comparison of Demographic and HIV Infection Characteristic Among HIV-Positive Individuals Diagnosed During 2015–2018 in Songyang County, China, According to Age
Using Fisher's exact test.
Only for participants infected from commercial sex behavior and noncommercial sex behavior diagnosed in 2017 and 2018.
CDC, Center for Disease Control and Prevention; SY, Songyang County; XP, Xiping Village.
A total of 101 participants were diagnosed with HIV at hospitals (63.1%, n = 101), included 59 diagnosed during physical examinations (PE) conducted by basic public health services in rural areas. Forty-nine participants were diagnosed at the local Center for Disease Control and Prevention (CDC) (30.6%, n = 49). Over one-third (36.9%, n = 59) of participants were diagnosed at the stage of AIDS.
To focus on the older HIV-positive individuals, study participants were divided into two groups by age at HIV diagnosis: <50 years (n = 49) and ≥50 years (n = 111). These age groups showed statistical differences (p < .05) in marital status, education, census registration, living township at HIV diagnosis, years of HIV diagnosis, agency of HIV detection, CD4 count at HIV diagnosis, transmission route, self-reported heterosexual contact history (for women), and the location of HIV infection. In contrast to participants <50 years old, those diagnosed at age ≥50 years were more likely to be married (61.3%, n = 68), less educated (illiteracy or primary school, 70.3%, n = 78), diagnosed after the year 2017 (80.2%, n = 89), diagnosed in hospital (69.4%, n = 77), and infected with HIV in SY County (75.7%, n = 53) (Table 1).
HIV infection-related exposure history
Heterosexual sexual contact was reported as the predominant exposure behavior of HIV infection, accounting for 92.5% (n = 148) of study participants, followed by homosexual sexual contact (7.5%, n = 12).
Among 148 participants with heterosexual contact history, 64.9% (n = 96) disclosed commercial sexual contact history (89 men and 7 women), 18.9% (n = 28) had extramarital noncommercial sexual contact, and 16.2% (n = 24) reported their husbands or wives as their only sex partners. There were 25 seroconcordant couples in total in this study. Among one seroconcordant couple, both the husband and wife were infected with HIV from extramarital sexual contact.
Characteristics of HIV subtypes and potential transmission clusters
Four HIV subtypes were identified among 109 participants with HIV sequence data, of which CRF 08_BC (67.0%, n = 73) was the predominant subtype, followed by CRF 07_BC (19.3%, n = 21), CRF 01_AE (11.9%, n = 13), and B (1.8%, n = 2).
At a distance threshold of 0.25%, 48.6% (n = 53) of 109 sequences linked to at least one other sequence, forming 15 clusters comprising 2–11 participants. Each cluster contained at least one male participant ≥50 years old, who had commercial sexual contact (i.e., an older male client). Eight clusters included seroconcordant couples (Fig. 1).

Molecular HIV transmission clusters of HIV patients diagnosed in SY County, China, during 2015–2018. This figure depicts HIV molecular transmission clusters of study participants in SY County. Each circle or triangle in the network corresponds to a study participant. Circle indicate men and triangles indicate women. Clusters 1–11 were of the CRF08_BC strain, clusters 12 and 13 were of the CRF07_BC strain, and clusters 14 and 15 were of the CRF01_AE strain. Connections are represented by a solid gray line if two participants have molecular linkage, and by a red line if the two participants are seroconcordant couples with molecular linkage. The circles and triangles are color coded to represent sexual contact characteristics, older male clients diagnosed with HIV at age ≥50 years, blue; male clients diagnosed with HIV at age <50 years, light blue; CSW, red; infected from spouses, yellow; other contact history, green. Edge lengths are not proportional to the genetic distance between nodes. SY, Songyang. Color images are available online.
Participants diagnosed with HIV at age ≥50 years (p = .019), divorced or bereft of one's spouse (p = .035), and those infected with HIV in SY County (p = .049) were more prevalent among the 15 clusters (Table 2).
Comparison of Demographic and HIV Infection Characteristic Among HIV-Positive Individuals Diagnosed During 2015–2018 in SY County, China, by Clustering Status
Using Fisher's exact test.
Only for participants infected from commercial sex behavior and noncommercial sex behavior diagnosed in 2017 and 2018.
SY, Songyang.
Clusters 1 and 2 were the two largest clusters of the CRF08_BC HIV strain in SY County, with 11 and 10 participants each. In cluster 1, seven of eight men had commercial sexual contact and five were diagnosed at age ≥50 years. In cluster 2, all eight men had commercial sexual contact and seven of them were diagnosed at age ≥50 years. Many participants in these clusters (9 and 8 in clusters 1 and 2, respectively), lived in a particular village or in the surrounding 15 km. The median GD between participants in clusters 1 and 2 was 0.002 and 0.002, respectively.
There were CSWs within cluster 1, 2, 8, and 12. Each of them had 4, 8, 1, and 4 molecular linkages with other participants. Older male clients in clusters 1 and 2 had 1–8 and 3–9 molecular linkage with other participants.
Figure 2 presents the Bayesian MCMC tree of all 73 CRF 08_BC sequences obtained using a Bayesian analysis. CRF 08_BC was estimated to be introduced into SY County in the year 2010, with an average evolution rate of 1.5910−3 nucleotide substitutions/site/year. There were three CSWs in two clades, a clade with CSW1 was formed in the year 2012–2013, and a clade with CSW2 and CSW3 was formed after 2017. The estimated time of HIV infection of 80.8% (59/73) of the participants with CRF08_BC was ∼2015–2017, including six seroconcordant couples.
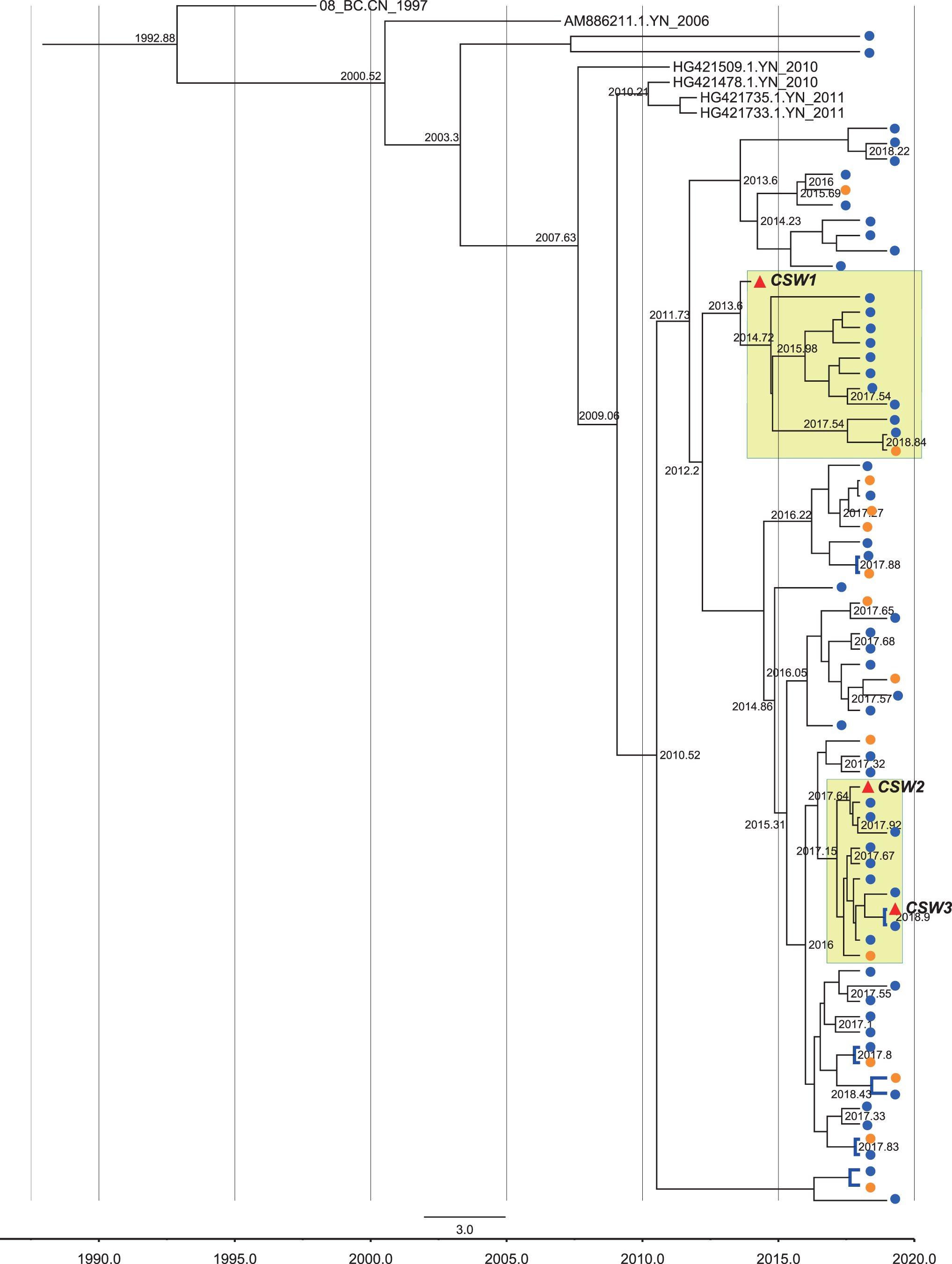
MCMC tree based on HIV pol sequences among CRF08_BC-infected patients diagnosed in SY County, China during 2015–2018. Bayesian molecular clock analyses were performed using BEAST v1.75 (see Methods for details); maximum clade credibility trees for clusters with a light yellow background suggests a cluster with a CSW, and evolved from the same ancestral strain. Nodes labeled evolutionary time are supported high posterior probability (≥0.90). Blue solid circle represents men, orange solid circles represent women, and red solid triangles represent CSWs. Blue lines represent seroconcordant couples. CSW, commercial sex worker; MCMC, Markov chain Monte Carlo. Color images are available online.
Epidemiological characteristics of transmission clusters that included CSWs
Four CSWs were found within the transmission clusters. Three of them were infected with CRF08_BC (cluster 1, 2, and 8), and one of them was infected with CRF07_BC (cluster 12). They were diagnosed with HIV between 2013 and 2018, and were 40–47 years old at diagnosis. They worked at specific venues in SY County. The four CSWs had been sex workers for varying durations (around a half year to over a decade). The CSW in cluster 1 was diagnosed with HIV in 2013, and she refused to be treated until 2018. The CSWs in clusters 2 and 3 moved to SY County from other cities in Zhejiang province and diagnosed in 2017 and 2018. The epidemiological survey indicated that they were infected with HIV in SY County. The four CSWs in the clusters had molecular links with 14 male clients in total, and 11 of these clients were diagnosed with HIV at age ≥50 years.
Discussion
By aggregating evidence from epidemiological field surveys and phylogenetic analysis, our study underscored the complexities of the burgeoning HIV epidemic in a rural area of eastern China. We found that continuous commercial sexual behavior among CSWs and older male clients has facilitated the expansion of a local HIV transmission network.
In our study, 89 of 109 male participants reported commercial sexual contact. Previous studies among male clients and CSWs in China have focused on the frequency of sexual contact and condom use. 8,14 We found evidence of back and forth transmission pathway among CSWs and senior male clients. Furthermore, ample evidence was found from epidemiology research and molecular analysis that CSWs act as “hubs” within local HIV transmission networks. In addition, both HIV-positive CSWs and older adults played crucial roles in transmission networks. 15 Therefore, in addition to health education and condom distribution among older adults and CSWs, more emphasis should be placed in identifying high-risk or HIV-positive individuals in rural areas.
Population mobility can accelerate the transmission of sexual transmitted disease, 16 including HIV. 17 Unlike randomly distributed transmission networks at the national 10,18 or provincial/state 19 level, the study site for this study is a rural county with low level of population mobility. However, HIV can be still be transmitted inadvertently through commercial sex among older adults. CRF08_BC and CRF07_BC, which originated in injection drug users in Yunnan Province, 20 were not the prevalent HIV strains observed in Zhejiang Province. 21,22 Moreover, we observed homogeneity within transmission clusters in SY County, including age, marital status, and the location of HIV infection and type of risk behavior. Epidemiological investigation found that among clustered participants, 81.1% (43/53) were diagnosed at age ≥50 years and 76.9% (30/39) were infected with HIV in SY County. HIV prevention intervention targeting the ‘hotspot would not only impact HIV incidence within the county, but also disrupt the much wider transmission network surrounding it. 23 In this study, epidemiological information collected from participants indicated that specific commercial sex venues including barbershops and rental rooms in specific village could be the hotspots for local HIV transmission. This is vital evidence for designing localized HIV prevention approaches.
Transmission cluster can represent recent and ongoing HIV transmission, providing important knowledge in a population where public health interventions could improve health care outcomes and prevent new infection. 24 The GD cutoff was selected at 0.25% for identifying recent or ongoing HIV transmission. 13 Integrating disease investigation and molecular HIV analysis provide the benefit of more rapid and efficient identification and response to localized outbreaks of HIV infection. 11 Rapidly detecting and responding to emerging clusters of HIV infection to further reduce new transmissions was proposed as a strategic initiative by the U.S. Department of Health and Human Services (HHS), with the goal of ending the HIV epidemic in the United States within 10 years. 25 Our study result suggests that the application of epidemiological investigation and molecular analysis on a county level is effective in detecting and identifying persons with multiple potential transmission links, especially in rural areas with fast growing HIV epidemics.
As with most epidemiological studies, our study suffered from several limitations. First, the number of identified PLWHA might have been affected by the intensity and coverage of HIV testing, the efficiency of policies and intervention strategies, and the study design. Second, because of the heterogeneity of HIV-1 quasi-species, the consensus population sequencing method we used could lead to mixtures at specific nucleotides, and result in miscategorization for some of the relationships identified in the cluster analysis. Clonal analysis would be more accurate in identifying transmission clusters, especially in highly suspicious transmission events. Additional limitations include the fact that 109 of 160 participants had a valid HIV sequence for molecular analysis, and PLWHA in SY County who were undiagnosed or without gene sequence data could not be included in the transmission network. However, 95 of the 109 participants with valid HIV sequence were diagnosed in 2017 and 2018, and thus our results can be representative of emerging clusters of the ongoing HIV epidemic in SY County.
Conclusion
In conclusion, our results delineate the complex traits of HIV epidemic dynamics and sexual networks among older adults in a rural county. Through epidemiological field surveys and phylogenetic analysis, we found evidence of key populations and geographic hotspots of local HIV transmission. Our results show that both male clients and CSWs played a crucial role in SY County HIV epidemic, indicating that detecting HIV transmission clusters through epidemiological field surveys and phylogenetic analysis should be prioritized, and that more evidence-based localized HIV testing and intervention strategies should be designed to reduce onward HIV transmission in rural areas.
Footnotes
Authors' Contribution
J.J. and L.Y.Q. collected and prepared the epidemiological information. Q.F., J.F. Z., and X.B.D. processed and managed HIV-1 sequence data. X.H. P, J.M.J., and L.Y.Q. conceived the study. J.J. and Q.F. did all analyses. M.Y.L. provided support and advice. X.H. P. and J.M.J. reviewed the statistical analyses. J.J. and Q.F. wrote the article and all authors revised the final draft.
Acknowledgment
The authors thank all study participants for devoting their time to recall sexual behavior history. Without their help this research would not have been possible. We gratefully acknowledge the staff, Shufeng Liu, Tao Tao, and Weiqun Shi in the Center for Disease Control and Prevention and SY County and Lishui City for their assistance in collecting valuable epidemiology information and blood sample among study participants. The authors also thank Professor Andreas Handel, Dr. Justin Bahl, and Dr. Ye Shen of University of Georgia for reviewing and providing advice regarding the article.
Author Disclosure Statement
No competing financial interests exist.
Funding Information
This work was supported by Health Commission of Zhejiang Province, Zhejiang Medical and Health Research Program (grant: 2019KY356). Results and conclusions reported in this article are those of the authors and do not necessarily represent the views of the Health Commission of Zhejiang Province.