
Abstract
We aim to determine the prevalence of HIV nonsuppression and factors associated with it. This is a cross-sectional multicenter study carried out in January 2016 with data of the VACH Cohort, a registry participated by 23 hospitals from most regions of Spain. The prevalence of HIV nonsuppression, defined as HIV RNA ≥200 copies/mL, is documented. The possible association of HIV nonsuppression with sociodemographic and clinical variables is assessed with a logistic regression analysis. A total of 30,843 adult patients are included; 7,358 of them (23.86%) have nonsuppressed HIV. An association is found between nonsuppression of HIV and the following variables: lower body mass index, lower age of patients in their last registered visit, lower number of visits carried out during follow-up, lower last available CD4 cell count, higher age of patients at the time of their HIV infection diagnosis, higher lowest available CD4 cell count, higher highest available HIV RNA, enrolment in the Cohort in first years of the HIV epidemic, region of Spain where the patient is attended other than Andalusia, HIV risk factor other than sexual, occurrence of death during follow-up, hepatitis C coinfection, being a smoker, pertaining to groups A1 or A2 of the CDC groups classification, and not taking antiretroviral treatment, p < .001 in all cases. HIV nonsuppression is still common with the effective antiretroviral treatment nowadays available. HIV nonsuppression is associated with HIV risk factor other than sexual, hepatitis C coinfection, and being a smoker, among other factors.
Introduction
Virologic nonsuppression of HIV has obvious negative consequences for patients, including progression of infection and increased risk of associated morbidity and mortality. 1 Studies in the past decades showed that the problem affected not only patients in underdeveloped regions, with poor sanitation, but also to patients in industrialized countries, where the most advanced health systems are available. Nowadays, treatments of HIV are much more effective, safe, and convenient for patients than those available in the first decades of the epidemic. But, despite that, the problem of nonsuppression persists. 2 –8
Nonsuppression may be due to many reasons. HIV resistance, intolerance to medications, and especially poor adherence to drugs are considered the major determinants. But other factors such as high pretreatment viral load, low nadir CD4 cell count, comorbidities, pharmacokinetic issues, prior exposure to suboptimal regimens, food requirements, drug interactions, or prescription mistakes may also be important in many cases. 2 –8 Anyway, the problem is complex and involved with several factors commonly implicated at a time. Improved knowledge in the field is still needed, to design appropriate support programs for those groups of patients with high nonsuppression rates.
In this study, we aim to determine nowadays prevalence of HIV viral load nonsuppression in real clinical practice, and improve knowledge on factors associated with that problem. For that purpose, we use data from Spain, one of the developed countries with higher prevalence of HIV infection. In this country, in the beginning of the epidemic, HIV was related to intravenous drug use, but nowadays, in the 90-90-90 objectives era, it has become a predominantly sexually transmitted condition. 9
Materials and Methods
Design
This is a multicenter cross-sectional study to determine the prevalence of HIV nonsuppression and to try to find factors associated with HIV nonsuppression.
Setting and patients
All the study data belong to patients included in the VACH Cohort Registry, a Spanish multicenter project, participated by Infectious Disease departments of 23 hospitals, pertaining to most regions of the country. 9 The Registry was created in 2000 and is continuously updated by members of the VACH Group. Recruitment and follow-up of patients are designated as a supplementary task to conventional clinical practice that does not modify the guidelines recommended care of patients. 10 All consecutive HIV-infected patients attended at participating centers are included in the Registry, if they give informed consent. Patients who do not give informed consent to participate are excluded from the Registry but are still attended as recommended by guidelines. More specific features of the Registry have been described elsewhere. 9,11
For the purpose of this study, we initially include all patients available in the Registry on January 31, 2016. We exclude those patients with unavailable results in the variables used in this study (see Tables 1 –3).
Characteristics of the Study Patients: Discrete Variables and Their Results
Data belong to the first visit, unless otherwise specified.
Variables excluded of multivariable analysis because of redundant information or collinearity with other variables.
Dependent variable.
NA, nucleoside analogue.
Characteristics of the Study Patients: Normally Distributed Continuous Variables and Their Results
Variables excluded of multivariable analysis because of redundant information or collinearity with other variables.
Characteristics of the Study Patients: Non-Normally Distributed Continuous Variables and Their Results
Variables excluded of multivariable analysis because of redundant information or collinearity with other variables.
All study centers use Cobas AmpliPrep/Cobas TaqMan HIV-1 Test v2.0, Roche Molecular Diagnostics, Pleasanton, CA, USA.
Study variables
A total of 28 variables are initially used in this study. Tables 1 –3 summarize them. In a separate article, we report a detailed description of the cohort, which includes results of a total of 53 sociodemographic and clinical variables.
Both sociodemographic and clinical variables are a priori hypothesized as possibly associated with HIV viral load nonsuppression.
Ethics
The study is carried out in compliance with the ethical principles for medical research involving human subjects, as set forth in the Declaration of Helsinki of 1964, and subsequent updates, 12 and in compliance with Spanish laws and regulations regarding confidentiality, patient autonomy, data protection, and medical research. The study is entirely performed with anonymized codes of participants, instead of recognizable personal details. The Ethics Committee of one of the participating centers, the Hospital Infanta Elena of Huelva, Spain, had approved the Registry protocol.
Statistics
Q-Q probability plots and Kolmogorov–Smirnov test are used to assess normality of continuous variables. Positively skewed variables are logarithmically transformed if needed. To simplify analyses, all discrete variables results are grouped into two possible values, except for the variable “antiretroviral treatment at the time of the last HIV RNA analysis,” whose results are grouped into five possible values.
Discrete variables are summarized as absolute number and percentage, and continuous variables are summarized as mean and standard deviation if normally distributed or as median and interquartile range if not normally distributed.
A multivariable binary logistic regression analysis, available in software IBM SPSS Statistics version 22, is carried out to try to find associations between a dependent variable and independent variables. The default specifications of the test are employed. The dependent variable is viral load nonsuppression (≥200 copies of ARN/mL) or suppression (<200 copies of ARN/mL) in the last available results. The independent variables are all the other study variables.
A level of significance of p < .05, of one or two tails, as needed, is used for all calculations in the study.
Results
Descriptive data
We initially assess all the 33,729 patients available in the VACH Registry on January 31, 2016. We exclude a total of 2,886 patients (8.56%), due to unavailability of data of the study variables and, therefore, we finally include 30,843 patients (91.44% of those initially assessed). Figure 1 summarizes this process.
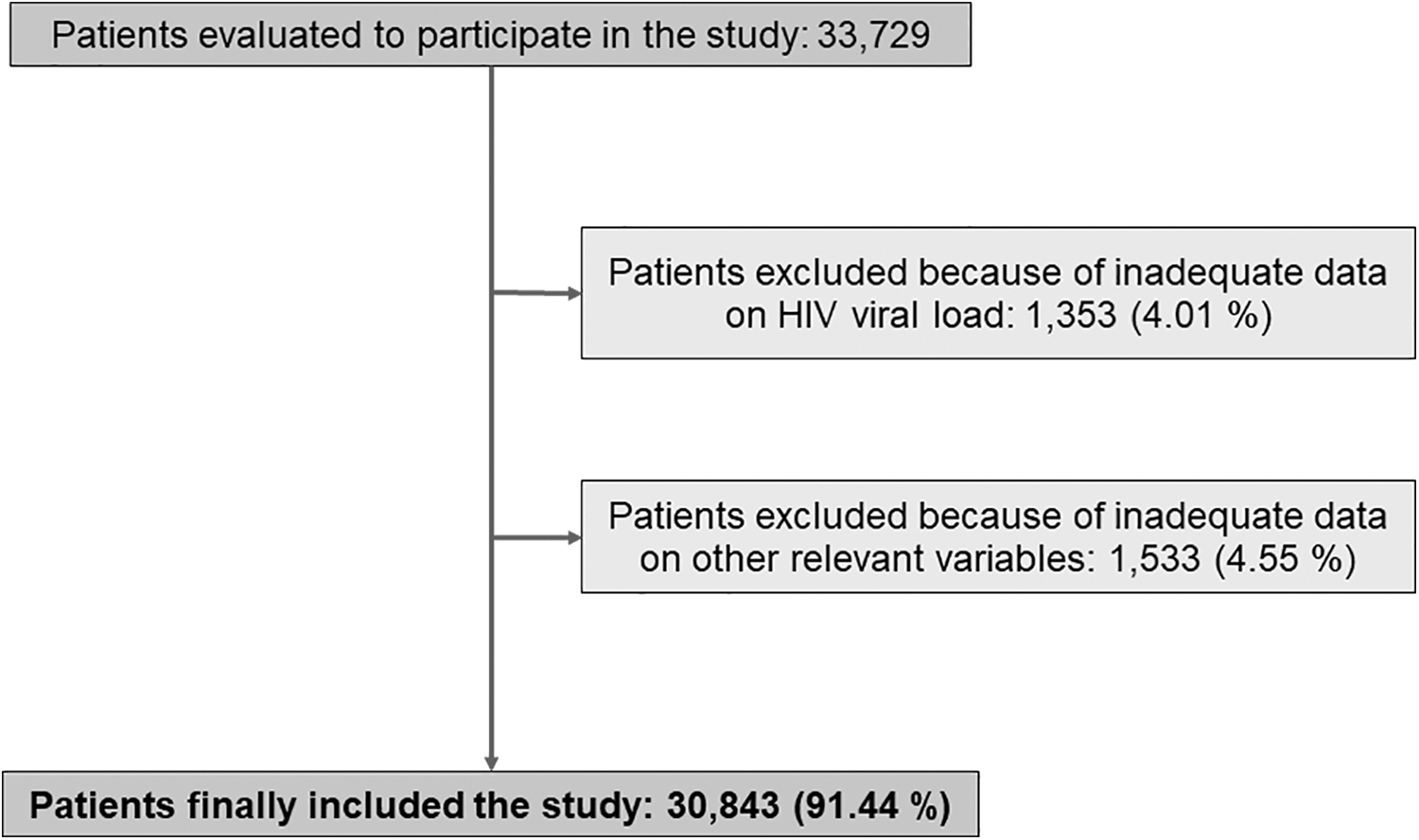
Flowchart of the study patients.
Tables 1 –3 display the results of the study variables. All data from all finally included patients are available for analysis.
Multivariable analysis
For the multivariable analysis we exclude four variables because of redundant data with other variables considered more relevant, and four variables because of problems of collinearity with other variables considered more relevant. Figure 2 summarizes this process. A total of three variables are positively skewed and are logarithmically transformed.
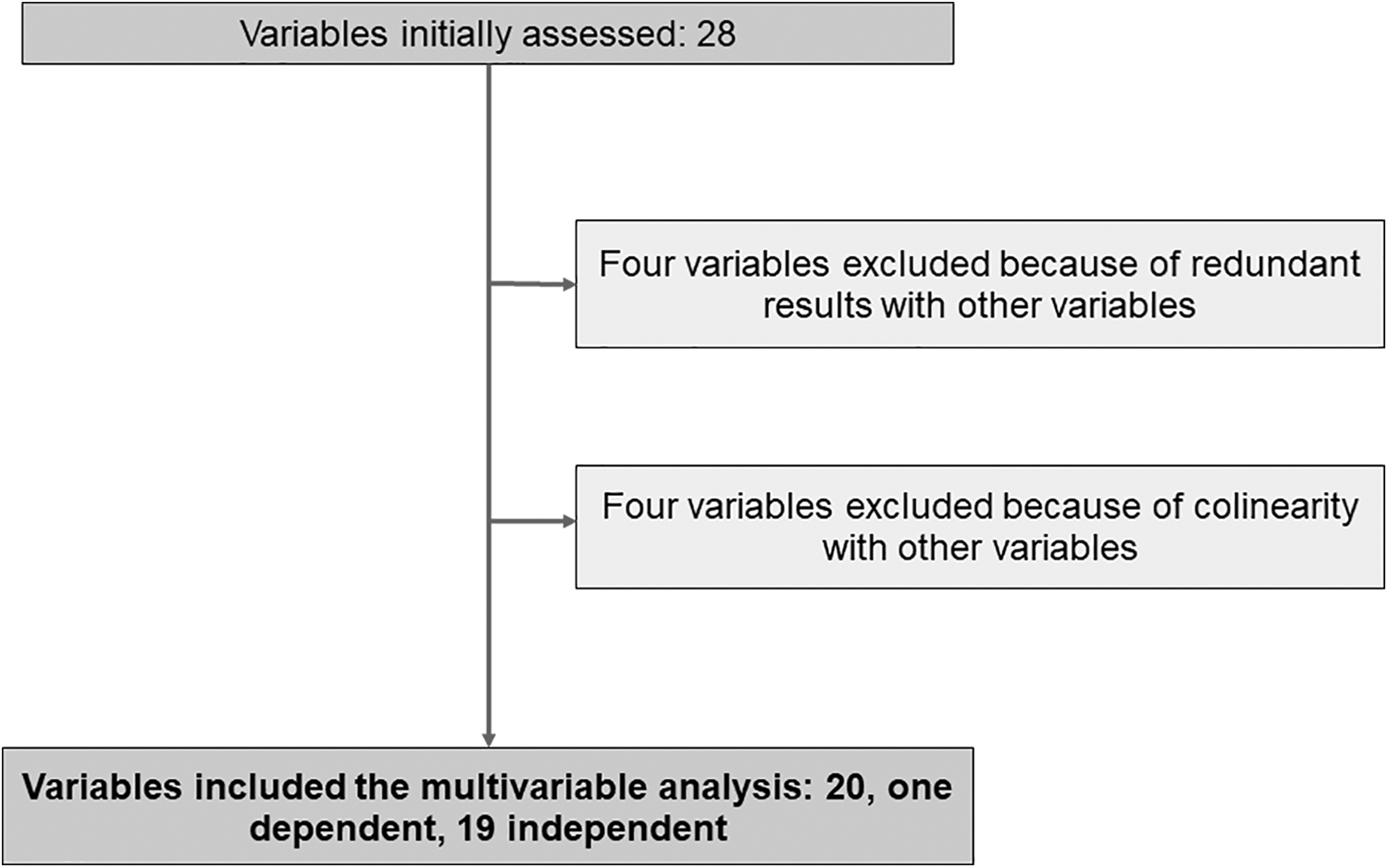
Flowchart of the study variables.
A direct logistic regression analysis is carried out, with the method “enter.” For that purpose, we use last HIV viral load not suppressed (≥200 HIV-RNA copies/mL) or suppressed (<200 HIV-RNA copies/mL) as dependent variable, and all the other variables that are finally included in the study (see Table 4) as independent variables.
Multivariable Logistic Regression Analysis
Data in rows belong to independent variables in the regression, in relation to the alternative “nonsuppression” of dependent variable.
Comparisons: (a) two nucleoside or NA plus an integrase inhibitor compared with all other groups; (b) two NA plus one protease inhibitor compared with all other groups; (c) two NA plus one non-nucleoside analogue compared with all other groups; y (d) no treatment compared with all other groups.
B, coefficient of regression; df, degrees of freedom; SE, standard error; Sig., statistical significance or P; Exp(B), odds ratio.
The analysis of the whole model compared with the constant model is statistically reliable: χ 2 10,050.001; p < .001. That means that independent variables are useful to reliably predict the dependent variable. The variation in the dependent variable explained by the independent variables is mild to moderate, with a coefficient of Cox & Snell R 2 = 0.278 and a coefficient of Nagelkerke R 2 = 0.417. Prediction of nonsuppression of viral load is correct in 49% of cases, whereas prediction of suppression is correct in 93% of cases. Overall prediction is correct in 83% of cases.
Table 4 shows regression coefficients, statistical significance level, and other results belonging to the regression variables. A total of 15 of the 19 independent variables show an association with the dependent variable.
Discussion
Our study is one of the largest projects on factors associated with HIV nonsuppression published in the literature of all time, and one of the few of them published recently. 2 –8 Studies of this kind are relevant because HIV-infected patients still have a disproportionally higher prevalence of morbidity and mortality, compared with the general populations, 13 and nonsuppression of the virus is presumably the main determinant. 14,15
Our study shows an association of nonsuppression of HIV RNA with a total of 15 variables, that is, with the majority of the 19 variables that we assess in a multivariable analysis. This is explained, at least in part, by the large number of patients that we include, which is known to favor the finding of statistically significant differences among variables, in general. 16
Among continuous variables, we find an association of nonsuppression of HIV RNA with lower body mass index, lower age of patients in their last registered visit, lower number of visits carried out during follow-up, and lower last available CD4 cell count. And we also find an association of nonsuppression of HIV RNA with a higher age of patients at the time of their HIV infection diagnosis, higher lowest available CD4 cell count, and higher highest available HIV RNA.
Published studies show mixed results regarding the association of HIV nonsuppression with body mass index 17,18 or age, 7,19,20 whereas HIV nonsuppression association with baseline or highest HIV RNA is much more uniformly reported in the literature 1,21 and coincident with our findings. Our result of association of nonsuppression of HIV with higher lowest (nadir) available CD4 cell is clearly discrepant with most published results, 1,16 although the corresponding regression coefficient in our study is close to negligible and, therefore, the relevance of this finding is questionable. We have found no studies assessing the relationship between nonsuppression of HIV and the number of visits made during follow-up.
Among discrete variables, we find an association of nonsuppression of HIV RNA with enrolment in the Cohort in first years of the HIV epidemic, region of Spain where the patient is attended other than Andalusia, HIV risk factor other than sexual, occurrence of death during follow-up, hepatitis C coinfection, being a smoker, pertaining to groups A1 or A2 of the CDC groups classification, and not taking antiretroviral treatment.
All those results are in accordance with general knowledge of HIV and published literature. 1,10 For example, the association of nonsuppression of HIV with the diagnosis of the infection the first years of the HIV epidemic, increased risk of death, or not receiving antiretroviral treatment are obvious. Our results suggest a superiority of integrase inhibitor or non-nucleoside analogue-based antiretroviral treatments, compared with other treatments, but our study was not designed to compare treatments and, therefore, this finding must be interpreted with care. In contrast, our results endorse the previously reported association of nonsuppression of HIV with parenteral HIV risk factor, which is probably related to poor adherence to antiretroviral drugs in that group of patients. 22 –24
Our results also show an independent association of nonsuppression of HIV with hepatitis C virus infection. Previous studies have given mixed results in this regard, 25 but in agreement with our results, recent studies have found increased morbidity among coinfected patients, 26,27 which presumably will be overcome in the near future with the highly effective hepatitis C treatments now available. 28
Another remarkable finding in our study is the increased rate of nonsuppression of HIV in regions other than Andalusia when HIV-infected patients in all regions of the country are covered by the National Health Service with similar resources. We have found no other studies assessing this point in Spain, but differences among regions with similar health systems have also been reported. 29 The association of nonsuppression of HIV with the habit of smoking, especially prevalent among our patients, has also been previously reported. 30
The association of nonsuppression of HIV with pertaining to groups A1 and A2 of the CDC classification is with all probability explained by the fact that antiretroviral treatment was not recommended for those groups of patients in guidelines of only a few years ago.
We believe that the main limitation of our study is the cross-sectional design, although that is the usual design used to find factors associated with clinical variables, when randomized comparative studies are not feasible. 31,32 In that regard, a longitudinal design of our study would have given more specific and informative results about the association of nonsuppression with the independent variables.
Another potential limitation is the lack of uniformity in data collection among centers of the VACH Cohort. Although the use of the same electronic application in all centers probably serves to minimize that problem.
And finally missing data is another drawback of our study, which made us exclude from multivariable analyses a small but significant percentage of patients.
Despite those limitations, the large number of patients and the massive quantity of data availability are important advantages of our study that allow reaching reliable conclusions. Our findings can be used to design strategies to modify factors related to nonsuppression in affected groups of patients and, therefore, may assist to improve control of the disease. 33
In brief, our study shows that nonsuppression of HIV is still a problem, despite availability of effective treatment. We outline several factors related to the problem, which should be specifically addressed to improve control of the disease. We believe that health systems must still assume HIV infection as a priority that requires continued efforts in clinical practice and in research.
Footnotes
Author Disclosure Statement
No competing financial interests exist.
Acknowledgments
Roca B, Teira R, Domingo P, Geijo P, Galindo MJ, Lozano F, Terron A, Garrido M, Suarez-Lozano I, Vidal F, Muñoz-Sanchez P, Viciana P, Ribera E, Castaño M, Martinez E, Puig T, Estrada V, Deig E, de la Fuente B, Montero M, Muñoz-Sanz A, Sanchez T, Romero-Palacios A, Lacalle JR.
Funding Information
No funding was received for this study.