
Abstract
Poor access to HIV viral load (VL) testing prevents the timely monitoring of HIV treatment adherence and efficacy. Factors enabling clinical benefits of VL testing when added to local standards of care, can inform the development of more cost-effective routine VL scale-up plans. We compared antiretroviral therapy (ART) switch practices in 13 clinics across 6 countries, with full (N = 8), phasing-in (N = 3) or no onsite access (N = 2) to VL. The analysis used data from the Pan-African Studies to Evaluate Resistance (PASER), observing virological and drug resistance outcomes among adults receiving first- or second-line ART between 2008 and 2015. Study plasma viral load (sVL) determined at baseline, every 12 months thereafter and at the time of switch served for retrospectively validating switch decisions, categorized into “necessary,” “unnecessary,” and “missed.” Virological failure was defined as two consecutive sVL ≥1,000 HIV-RNA copies/mL. One thousand nine hundred ninety-five of the 2,420 (82.4%) study participants had continuous virological suppression during the median 30 months of follow-up. Among the 266 virological failures (11.0%), the proportion of necessary switches were similar in clinics with full (37%), phasing-in (25%), or no access (39%) to local VL testing. Documented utilization of local VL results for the switch decision was associated with higher percentage of necessary switch (87.6% vs. 67.9%). Shorter time to necessary switch was associated with higher rates of long-term virological suppression, regardless of access to local viral load. Availability of HIV VL testing capacity does not systematically result in adequate switch practices or better virological outcomes. Systems supporting sufficient test demand execution, and actual utilization of results for patient management need strengthening.
Introduction
HIV RNA viral load (VL) is recommended by the World Health Organization (WHO) 1 as the most reliable indicator to confirm the success of antiretroviral therapy (ART) and support the timely and adequate clinical management that preserves the efficacy of empirical first- and second-line treatments. 2 The WHO defines virological failure as two consecutive HIV RNA VL ≥1,000 copies/mL of plasma after at least 3 months of ART, with treatment adherence support following the first VL result ≥1,000 copies/mL. 1 Intensified adherence counseling after an initial high VL results is an important aspect of patient management. Confirmed virological failure, despite documented treatment adherence is suggestive of HIV drug resistance (HIVDR). It is an indication to promptly switch to second-line therapy, to subsequently ensure the resuppression of the VL, allow immunologic recovery, and prevent HIV-related and non-HIV-related morbidity and mortality. Delayed, missed, or unnecessary switch to second-line treatment can promote the emergence of HIVDR, favor mortality and morbidity, reduce future treatment options, and increase direct and indirect costs of HIV care. 3 –5
The lack of HIV VL molecular testing capacity has been identified as the main barrier to the virological monitoring of ART in many low- and middle-income countries in sub-Saharan Africa that adopted the WHO recommendation for the routine VL monitoring of ART. 6 For this reason, large VL scale-up programs are being implemented in multiple sub-Saharan African countries to improve the clinical outcomes of ART and accelerate the achievement of the third fast track treatment targets of UNAIDS stating that 90% of all people receiving ART should have virological suppression by 2020. 7,8
However, evidence suggests that in routine practice, improved access to VL testing capacity alone might not necessarily translate into enhanced public health outcomes. 9 The execution of VL testing for all who need it and the prompt review and sharing of test results by laboratory staff to the clinicians for swift appropriate actions are critical to realize the full clinical potential of VL testing. 10 –13 The cost and complexity associated with VL testing remain significant for the constrained health systems of low- and middle-income countries, while scarce resources are also needed to strengthen clinical practices promoting linkage to care, patient retention, and treatment adherence support to achieve lasting virological suppression.
There is a need to document whether and under what conditions access to VL testing capacity can translate into clinical benefits when added to local standards of care in “real-life” clinical settings of sub-Saharan Africa. These data could inform the development of more cost-effective VL scale-up plans and the rational allocation of resources ensuring sufficient support of those clinical practices that are most effectively supporting the realization of “the third 90.”
To assess the impact of available VL testing capacity on regimen switching, we compared ART switch practices in 13 clinical sites in Uganda, Zambia, South Africa, Nigeria, Zimbabwe, and Kenya with different access to VL testing: full, partial, or absent. We used observational cohort data from the Pan-African Studies to Evaluate Resistance (PASER), observing virological and HIVDR outcomes among HIV-positive adults receiving first or second-line ART 14 according to respective local standards of care. Clinic- and patient-associated determinants of appropriate switch practices and favorable treatment outcomes were investigated.
Materials and Methods
Study design, setting, and population
The Pan-African Studies to Evaluate Resistance Monitoring (PASER-M) has followed a prospective cohort of HIV-1-positive adults (≥18 years) at 13 clinical sites in 6 sub-Saharan African countries. Details on the cohort with first- and second-line treatment outcomes have been described elsewhere. 3,14 –17 Participants were enrolled at the time of first- or second-line ART initiation and participants were followed up in routine care according to local ART guidelines, 1,18,19 which included onsite routine VL monitoring, whenever VL testing was accessible and part of the local standards of care. The cohort was closed, with every patient enrolled and starting treatment between 2008 and 2011. The present study included all participants who initiated first-line regimen containing a non-nucleoside reverse transcriptase inhibitor (NNRTI) and two nucleoside reverse transcriptase inhibitors (NRTIs) or who initiated second-line booster-PI-based regimen.
A standard case-report form capturing data on demographics, clinical status, medication, adherence, and laboratory results was completed at enrolment, every 3 months thereafter, and at regimen switch. CD4 cell counts recorded closest to the ART start date were used as pretreatment counts. Treatment failure was assessed at each visit by the clinicians based on clinical, immunological, and/or virological criteria defined by local standards of care guidelines, as previously described. 14 Clinical failure was defined as WHO clinical stage 4 condition after 6 months of effective treatment. Immunological failure was defined as CD4 count falling to or below baseline levels or persistently below 100 cells/mm3. Virological failures was defined as two consecutive VL ≥1,000 HIV-RNA copies/mL after 3 months with adherence support. Reasons for treatment switch as determined by the clinicians were reported in the patient files. Maximum patient follow-up time to database closure differed between clinical sites: 24 months for six sites (two Kenya, two South Africa, two Zambia), 60 months for two sites (one Nigeria, one Zimbabwe), and 72 months for five sites (one South Africa, three Uganda, one Zambia). Patients were followed up until the end of the study or until discontinuation because of death, transfer out, switch to third-line, or loss to follow-up (i.e., unseen for >180 days).
Ethics
Participants provided written informed consent at study enrolment. The study was approved by the appropriate research ethics committees at all collaborating sites. The secondary analysis of anonymous data at CDC was determined as nonhuman subjects research by the Office of the Associate Director for Science at the Center for Global Health, CDC, Atlanta, GA.
Laboratory methods
Plasma samples for retrospective study VL (sVL) were collected at baseline and every 12 months thereafter, and at time of switch to second-line or third-line treatment. The sVL was determined using NucliSens EasyQ real-time assay (version 2.0; bioMérieux, Lyon, France) or COBAS Ampliprep/COBAS TaqMan assay (Roche, Branchburg, NJ). The costs of the sVL were covered by the program. For the retrospective analysis, virological failure was defined as two consecutive sVL ≥1,000 HIV-RNA copies/mL, during the follow-up and at least 6 months after ART initiation.
Subsequent genotypic resistance testing (sGRT) was performed if the sVL was ≥1,000 HIV-RNA copies/mL. Population-based genotyping of protease and partial reverse transcriptase was done using in-house sequencing methods. 20 Major drug resistance mutations were scored using the 2017 International Antiviral Society–USA drug mutation list. 21
Statistical analyses
sVL results were used to define virological failure and to retrospectively validate the documented reason(s) for switch in the patient files. Virological failure was defined as two consecutive sVL ≥1,000 HIV-RNA copies/mL. ART switches were retrospectively categorized as “missed,” when no switch occurred after two consecutive sVL ≥1,000 HIV-RNA copies/mL; “unnecessary” when occurring during virological suppression (latest sVL <1,000 HIV-RNA copies/mL); and “necessary” when occurring after two consecutive sVL ≥1,000 HIV-RNA copies/mL. The adequacy of ART switch decision was retrospectively assessed from the perspective of virological failure, to understand the level of contribution of onsite VL testing to correct decision to switch.
HIVDR was identified among those with sGRT data available and was defined as low-level, intermediate, or high-level resistance to one or more of the NNRTIs, NRTIs, and PIs; A Stanford classification of “potential” drug resistance was not classified as drug resistance. HIVDR information was not required for the ART switch decision as per WHO recommendations for the public health approach to ART during the study period. 3,18,19 Hence HIVDR data were not used to assess the adequacy of switch decision, and rather served to retrospectively understand the consequences of switch decision on the HIVDR outcomes.
Due to logistical constraints inherent to the study set up, the result of sVL and HIVDR genotyping became available months to years after any given patient visits, and had no influence on the clinicians' decision to switch.
Patient characteristics and clinic access to local HIV VL testing (full, partial, or none) were compared according to whether a patient switched to a second- or third-line ART regimen (categorized into necessary, unnecessary, or missed switch) or was maintained at the same regimen in the context of virological suppression using chi-squared tests. The cumulative probability of remaining virally suppressed was estimated with confidence intervals (95% CIs) over 12-month periods using the Kaplan–Meier method. For the subset of patients experiencing viral failure, the time to switch to a second- or third-line ART regimen was assessed against patient and clinic characteristics using Cox proportional hazards models, including a frailty term to account for heterogeneity by study site. HIVDR was measured cumulatively by a 1-year time period, and summarized by clinic access to VL testing and type of ART switch. All analyses were conducted using SAS 9.3 (SAS Institute, Cary, NC).
Results
Clinic profiles
Among the 13 participating clinics, 8 had access to either onsite (N = 5) or centralized (N = 3) VL testing for the full study period (Table 1). Additionally, two clinics in Zambia had no access to VL testing for the whole study period, three clinics started to access VL testing services in 2011 (two clinics in Kenya) and 2012 (one clinic in Zimbabwe). The 11 clinics accessing local VL testing at one point or the other, reported a 6- or a 12-month routine testing schedule. VL testing costs were supported by the ART program for nine clinics and by patients themselves or through a research project in two (private) clinics. Second-line antiretroviral drugs (ARVs) were available for the whole duration of the study in 11 clinics. Third-line ARV was available for the whole study period in two clinics and introduced during the course of the study in an additional five clinics.
Characteristics of the Facilities in the Pan-African Studies to Evaluate Resistance Cohort, 2008–2015
Kenya only completed 24 months of follow-up.
ART, antiretroviral therapy; ARV, antiretroviral drug; FBO, faith-based organization; NA, not applicable; NGO, nongovernmental organization; PFP, private for-profit; VL, viral load.
Cohort profile
The PASER-M cohort included 3,007 HIV-1-positive adults initiating first- or second-line ART in 1 of the 13 participating clinics. We included 2,420 participants who had at least two consecutive sVL results available in our analysis; 587 participants without consecutive sVL results were excluded (Fig. 1). Patients who had a high value for the WHO performance scale at baseline were more likely to have no consecutive sVL results. Among the 587 with no consecutive sVL results, 420 had <180 days of follow-up. The median follow-up time of the cohort was 30 months.
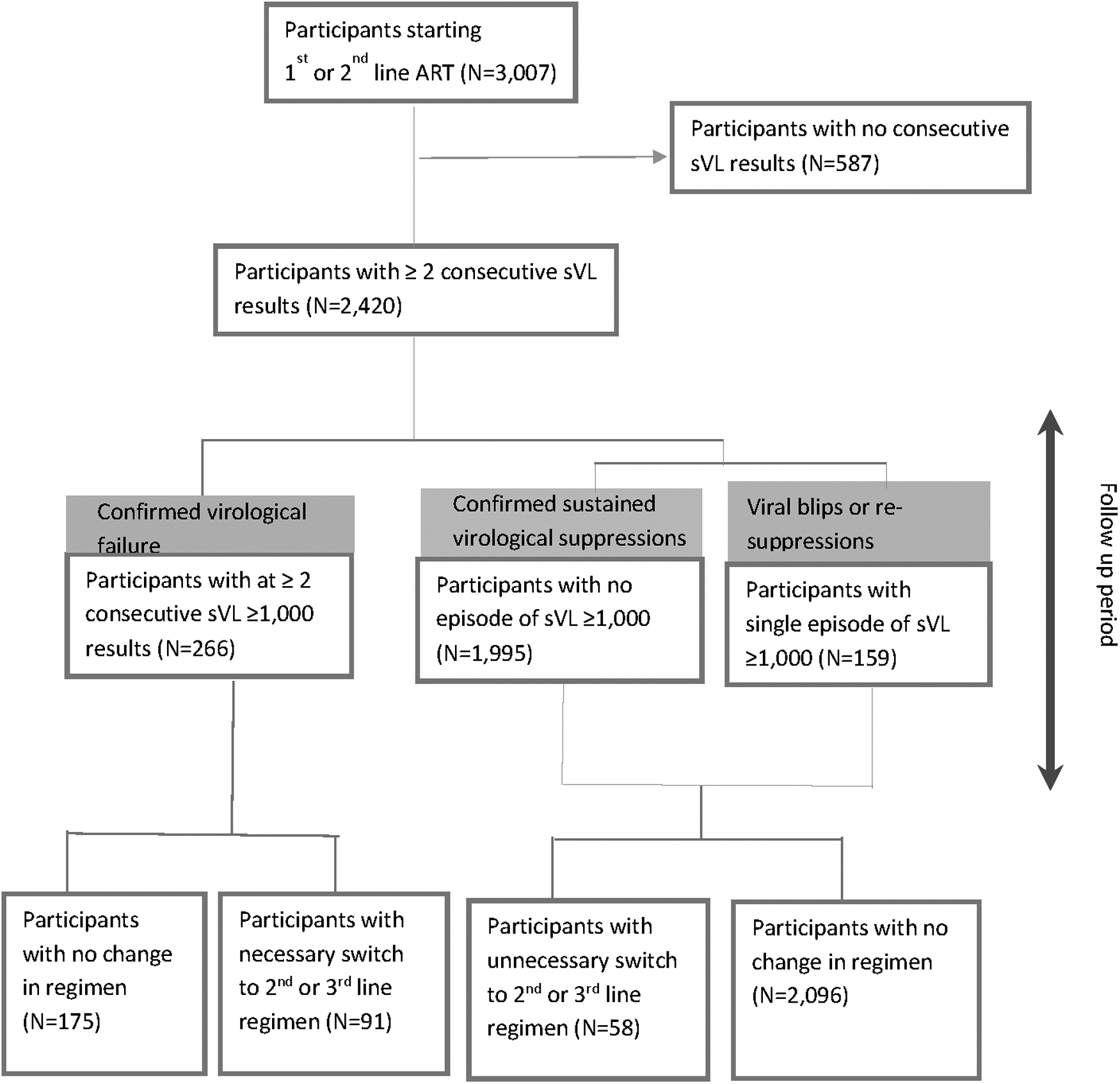
Of the 3,007 starting first- or second-line ART, 2,420 had at least two consecutive sVL results. Among those, there were 266 virological failures, 1,995 sustained virological suppressions, and 159 viral blips based on the sVL result across the whole study period. Among the 266 virological failures, 175 patients did not change ART regimen (delayed switch) and 91 had a necessary switch to second- or third-line treatment. Among the confirmed virological suppressions of viral blips, 58 unnecessarily switched to second- or third-line, whereas 2,096 stayed on the same regimen. ART, antiretroviral therapy; sVL, study viral load.
In total, 1,995 (82.4%) participants had continuous virological suppression (all sVL <1,000 copies/mL) throughout the follow-up period and 266 (11.0%) had at least two consecutive sVL ≥1,000 copies/mL (i.e., confirmed virological failure). There were no viral failures identified among patients on second line (data not shown). The remaining 159 (6.6%) had an isolated sVL ≥1,000 copies/mL (i.e., viral blips or resuppressions).
Virological outcomes, switch practices, and access to local VL testing
Among the 266 virological failures, 61 (37%), 16 (25%), and 14 (39%), respectively switched treatment in clinics with full, phased-in, or no access to local VL testing (Fig. 2 and Supplementary Table S1). Among the 159 participants with an isolated sVL ≥1,000 copies/mL (viral blips or resuppression), treatment switches were more common in the context of full access to VL testing (N = 23; 24%), compared with phasing in (N = 2; 4%) and no access (N = 1; 6%) to VL testing. Of the 1,995 participants with a continuously suppressed sVL, a minority were switched to second-line in clinics with full (1%), partial (2%), or no access to VL (2%), respectively. In total, 105 missed switches and 36 unnecessary switches were not avoided by onsite access to VL testing.
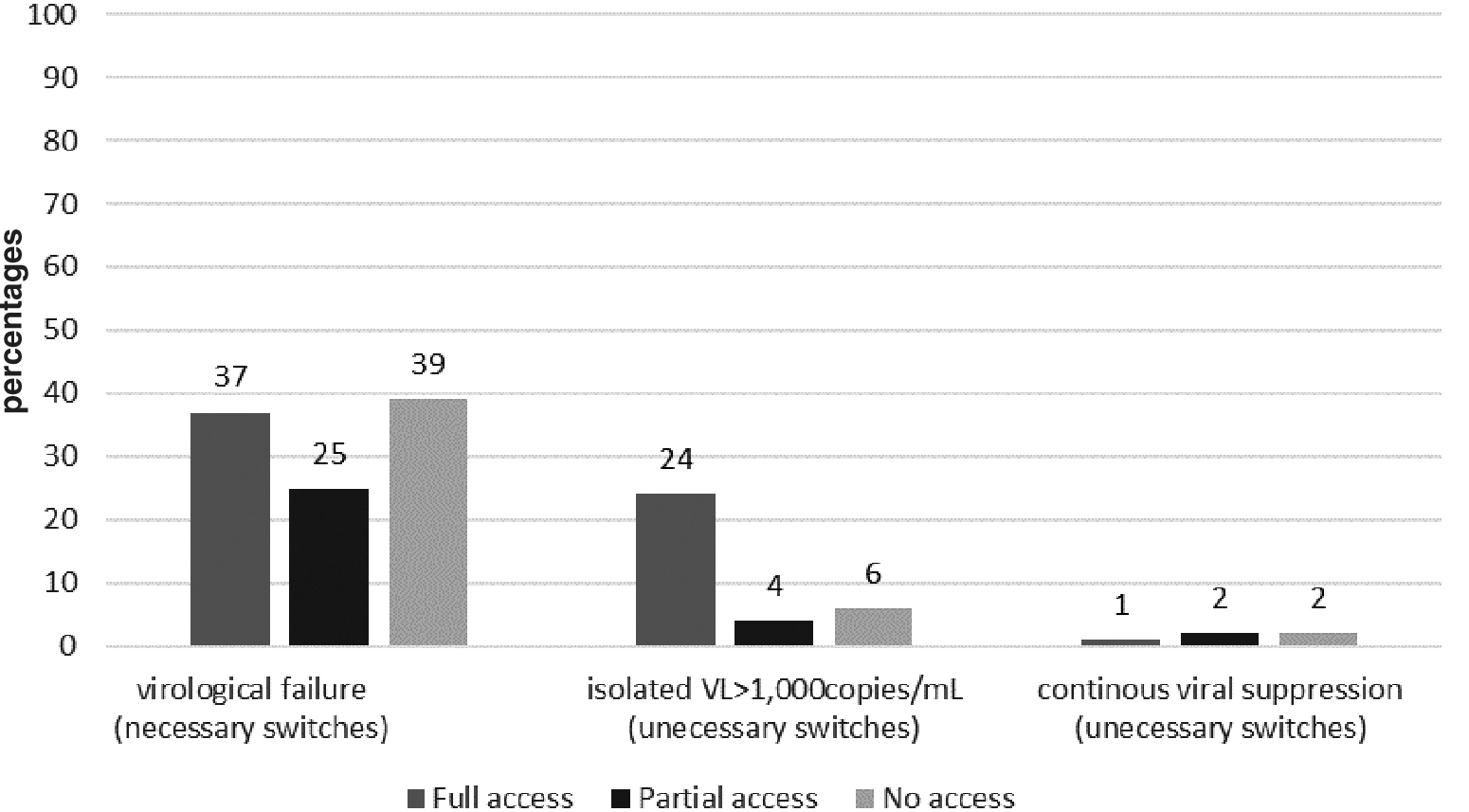
Percentages of patients from sites having full, partial, or no access to local viral load testing were compared among the groups of necessary, unnecessary and delayed switch.
Associations between patient characteristics, type of treatment switch, access to local VL testing, and time to necessary switch
Based on the sVL results, 149 switches could retrospectively be classified as necessary (N = 91) or unnecessary (N = 58, Table 3). There were 175 missed switches among patients with confirmed virological failure based on sVL. Although half of these patients (50.9%, Table 2) showed evidence of HIVDR mutation, 134 (77%) did not achieve resuppression at the end of the program. Moreover, 2,096 patients with no identified virological failure were maintained on the same regimen throughout the study period.
Patient Characteristics by Type of Switch to a Second- or Third-Line Regimen Among the 2,420 Patients Participating to the Pan-African Studies to Evaluate Resistance Cohort, 2007–2015, with ≥2 Study Viral Load Results Available
NNRTI, non-nucleoside reverse transcriptase inhibitor; NRTI, nucleoside reverse transcriptase inhibitor; PI, protease inhibitor; WHO, World health Organization.
HIVDR, HIV drug resistance.
Associations Between Participant Characteristics, Access to Local Viral Load Testing, and Time to Necessary Switch, in the Pan-African Studies to Evaluate Resistance Cohort, 2007–2015
Hazard ratios calculated using individual Cox proportional hazards models, including a frailty term for study site.
Time-varying covariate.
sVL, Study plasma viral load.
Patients cited above were more likely to be poorly adherent among the missed switches (30%) as compared with the necessary and unnecessary switches (21.8% and 7.7%, respectively). Occurrence of other medical conditions at baseline was comparable between patients with unnecessary and missed switches (10.3% and 9.7%, respectively) as compared with necessary switches (5.5%, Table 2). The clinician was more likely to report a virological failure as a reason for switch among necessary switches (87.6%) as compared to unnecessary switches (67.9%).
Access to local VL testing was not associated with faster switch decision (hazard ratio 1.12; 95% CI: 0.48–2.63, Table 3) among the 266 confirmed virological failure. Furthermore, age, sex, adherence, WHO performance scale, pulmonary tuberculosis, and other medical conditions were not associated with faster time to switch. However, longer period of virological suppression before virological failure and sites in South Africa (SA/ACC) and Uganda (UG/JCR) (both having full access to VL testing) were associated with faster time to switch.
Probability of acquiring HIVDR after initiating ART and access to local VL testing
The cumulative probability of remaining virally suppressed after initiating a first- or second-line ART increased over time and this was more marked after switching during follow-up compared with starting the initial regimen, after 1 year of follow-up [92% (95% CI: 84–96) vs. 97% (95% CI: 96–97)] at month 12; and [53% (95% CI: 33–70) vs. 78% (95% CI: 75–80) at month 60, Supplementary Tables S2 and S3].
Among the 2,420 patients initiating ART and having ≥2 consecutive sVL results, the cumulative probability of acquiring HIVDR to NRTI, NNRTI or PI, increased over time regardless of the type of access local VL testing (Table 4). Cumulative probabilities of acquiring HIVDR were not reduced in clinics with full access to local VL testing as compared with sites with no access to VL testing.
Cumulative Acquired HIV Drug Resistance After Initiating Antiretroviral Therapy by Follow-Up Time, and Access to Local Viral Load Testing Among 2,420 Patients Participating the Pan-African Studies to Evaluate Resistance Cohort, 2007–2015, with ≥2 Consecutive Study Viral Load Results (sVL) Available
Italic figures represent the number of participants for whom no sVL data were available and whom were not included in the analysis.
Number of patients with drug resistance mutation (s) based on the study genotyping HIVDR testing.
Number of patients still in follow-up with study viral load (sVL) results.
Discussion
This study shows that access to VL testing at the site of HIV care was not associated with improved treatment switch practices in 13 African clinics delivering ART according to national treatment guidelines. The proportion of missed and unnecessary switches to second- or third-line ART was similar in clinics that had direct access as compared with those that had no access at all to local VL testing. There were no longitudinal improvement in virological outcomes in those clinics acquiring VL testing capacity over time. The poor contribution of VL testing results to switch decision was accompanied by similar levels of virological failure and HIVDR in clinics with and without onsite access to VL testing, confirming the lack of impact of VL testing on the cascade of HIV care. Additionally, missed opportunities for VL-guided intensification of treatment adherence counseling were illustrated by the small resuppression rate, among failing patients with no HIVDR in sites with full access to VL. The results reported here corroborate findings in similar settings 22 and suggest that in clinics where VL testing capacity is available, low demand and/or utilization of test result for clinical management translate into no additional clinical benefit for patients receiving ART.
Despite this overall worrisome picture, the results show that when utilized, local VL testing did provide some value to patient management. Necessary switches were correlated to the reporting of “virological failure” in patient file, suggesting that clinicians used local VL test results showing unsuppressed VL to make the decision to switch. These observations confirm the clinical utility of VL testing, provided that the results are used for clinical management. Additionally, a larger proportion of patients with one isolated sVL ≥1,000 HIV-RNA copies/mL were switched to second line in clinics with full access to VL. This suggests that clinicians may have used local VL testing to take their decision to switch. Up to a third of those patients with a single isolated sVL ≥1,000 HIV-RNA copies/mL actually presented HIVDR mutations, and can retrospectively be classified as necessary switchers.
High rates of long-term virological suppression and clinic-associated characteristics rather than access to VL testing, correlated with faster time to necessary switch. These findings suggest that some sites do apply practices that critically enable the effective contribution of VL testing to patient outcomes. Some successful ideas supporting the optimal impact of VL test results include: appointing VL focal persons or champions ensuring that unsuppressed VL results in patient files; establishing ART committees at facility level or telephone hotlines to assist clinicians in taking clinical decisions; providing treatment adherence support through community outreach interventions. 23 Sharing locally developed and context-adapted solutions that facilitate the application of treatment guidelines in real-life clinical settings, could improve patient management regardless of access to VL testing technology.
Previous qualitative research conducted in one of the three participating facilities of Uganda, 24 confirmed that commonly described health system barriers affected the optimal utilization VL testing during the study period. These included: unaffordability of VL testing, inconsistent or poorly labeled VL test requests by clinicians, frequent equipment breakdown, specimen backlog, long turnaround time of test results, and shortage of skilled clinical and laboratory workforce. The poor interaction between clinic and laboratory staff as well as a poor overview of performances at each step of the VL testing cascade were identified as critical cross-cutting issues.
This study had some limitations. First, some sources of heterogeneity between participating sites could not be completely factored in the analysis. For instance, various levels of compliance to the WHO guidelines, difference in institutional organization of health care, retention policies, and human behavior could have influenced the findings. Moreover, it could not be ascertained that along the 10 years spanned by the study, facilities complied with new guidelines or had access to new drug regiment 100% of the time from January 1 to December 31 of any given year. Second, the lapse of 12-month in-between two sVL combined to the fact that some sVL were missed, might have overlooked some virological failures, thereby overestimating the proportion of unnecessary switches. Third, reluctance of the clinician to switch patients due to the lack of treatment adherence or unavailability of second- or third-line drugs could not be verified from the retrospective data analysis, with the possibility that missed switches might have been overestimated. Finally, although the IAS mutation list of 2017 and 2019 are comparable in terms of identifying (N)NRTI mutations, the HIVDR to PI may have been underestimated since additional protease mutations were added to the 2019 list after the study was completed.
Conclusions
More sophisticated, innovative, point-of-care or affordable technologies are often proposed as solutions to address diagnostic gaps in resource limited settings, and to improve individual patient and public health outcomes. Despite their initial promises, the implementation of diagnostic devices requires supportive systems such as rigorous quality assurance, robust systems for test demand, results' return and effective use, as well as efficient operation management 25 to ensure optimal clinical benefits and returns on investment. Our observations highlight the critical importance of appropriate treatment adherence monitoring and support, as an indispensable enabler of the clinical utility of HIV VL monitoring. The results reported in this study corroborate the recommendations from Chun et al., 6 to carefully review system requirements, structural needs, and procedural and technical factors for the entire continuum of VL testing. Special emphasis on optimal test demand and post-test result utilization at both site and national level is critical to optimize the expansion of VL testing, to minimize the emergence of HIVDR and to achieve the third 90 of the UNAIDS 90-90-90 targets. This requires system-strengthening approaches 26 based on multidisciplinary, multistakeholder interventions, specifically coordinated to improve the implementation of VL testing for appropriate patient management. 25,27 The implementation of actionable data dashboards linked to treatment outcomes, adequate and supervised staff, continuous quality improvement at the laboratory/clinic interface and sufficient allocation of resources to conduct corrective actions at the site level are important and should be pursued concomitantly with data-informed laboratory system strengthening at the national level.
Footnotes
Acknowledgments
The authors thank the study participants, the staff at the collaborating clinical sites, and reference laboratories. PASER is part of the Linking African and Asian Societies for an Enhanced Response to HIV/AIDS (LAASER) program, a partnership of Stichting Aids Fonds, the Foundation for AIDS Research (amfAR)-TREAT Asia, PharmAccess Foundation, and International Civil Society Support (ICSS).
The PASER Study Group: Mariette Botes (Muelmed Hospital, Pretoria, South Africa), E. Botes, Alani Sulaimon Akanmu, Suleiman Akanmu (Department of Haematology & Blood Transfusion, College of Medicine of the University of Lagos, Nigeria), Maureen Wellington (Newlands Clinic, Harare, Zimbabwe), Margareth Siwale (Lusaka Trust Hospital, Lusaka, Zambia), Kishor Mandaliya (Coast Province General Hospital, Mombasa, Kenya), Cissy Kityo (Joint Clinical Research Center, Kampala, Uganda), Eman E.F. Labib (Coptic Hospital, Lusaka, Zambia), and Titilope A. Adeyemo (Department of Haematology & Blood Transfusion, College of Medicine of the University of Lagos, Nigeria).
Disclaimer
The use of trade names is for identification only and does not constitute endorsement by the U.S. Department of Health and Human Services, the Public Health Service, or the Centers for Disease Control and Prevention. The findings and conclusions in this report are those of the authors and do not necessarily represent the official position of the funding agencies. The content of this publication is solely the responsibility of the authors and does not necessarily represent the official views of any of the governments or institutions mentioned above.
Author Disclosure Statement
No competing financial interest exist.
Funding Information
The Pan-African Studies to Evaluate Resistance (PASER) is an initiative of the Amsterdam Institute for Global Health and Development, with major support provided by the Ministry of Foreign Affairs of the Netherlands through a partnership with Stichting Aids Fonds (grant no. 12454), and the Netherlands Organization for Scientific Research (NWO-WOTRO grant no. W07.10.101 and W07.10.106), and additional support provided by De Grote Onderneming, The Embassy of the Kingdom of the Netherlands, Heineken Africa Foundation, and Jura Foundation. The data analysis has been supported by the President's Emergency Plan for AIDS Relief (PEPFAR) through U.S. Centers for Disease Control and Prevention. The funders had no role in study design, data collection and interpretation, or the decision to submit the work for publication.
Supplementary Material
Supplementary Table S1
Supplementary Table S2
Supplementary Table S3
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.