
Abstract
International guidelines recommend the use of integrase strand transfer inhibitor (INI)-based regimens as first-line antiretroviral (ARV) in both naive and experienced HIV-infected patients. We analyzed a multicenter cohort of HIV-infected patients, both naive and experienced, starting an ARV, including an INI. Chi-square test and nonparametric tests were used to assess differences in categorical and continuous variables, respectively. Kaplan–Meier survival analysis was performed to estimate the probability of maintaining the study drug and Cox-regression analysis to evaluate predictors of discontinuation. We enrolled 4,343 patients: 3,143 (72.4%) were males, with a median age of 49 years (interquartile range 41–55). Naive patients were 733 (16.9%), of whom 168 (22.9%) were AIDS presenters. Overall, 2,282 patients (52.5%) started dolutegravir (DTG), 1,426 (32.8%) raltegravir (RAL), and 635 (14.7%) elvitegravir (EVG). During 10,032 patient years of follow-up (PYFU), we observed 1,278 discontinuations (13 per 100 PYFU); 448 of them (35%) due to simplification and 355 (28%) to toxicities (98 for central nervous system toxicity). Reasons of discontinuation were different between INIs. Estimated probability of maintaining DTG at 3 and 4 years were 81.5% [95% confidence interval (CI): 80.5–82.5] and 76.3% (95% CI: 73.9–78.7), respectively; RAL 61.6% (95% CI: 60.2–63.0) and 54.1% (95% CI: 52.7–55.5); EVG 71.6% (95% CI: 69.2–74.0) and 68.3% (95% CI: 65.3–71.3) (p < .001). At a multivariable analysis, being on a RAL-based ARV [vs. DTG, adjusted hazard ratio (aHR) 2.9, 95% CI: 2.3–3.6, p < .001], a EVG-based ARV (vs. DTG, aHR 1.3 95% CI: 1.1–1.7, p = .049), and a peak HIV-RNA >500k cp/mL (aHR 1.3, 95% CI: 1.1–1.6, p = .006) predicted INI discontinuation. Our data confirm the good tolerability of INIs in clinical practice. Differences emerge between the three drugs in reasons for discontinuation.
Introduction
Integrase strand transfer Inhibitors (INIs) have become, in both national and international guidelines, 1,2 the first choice for both first-line antiretroviral (ARV) regimens and switch regimen in virologically suppressed HIV-infected patients, thanks to their efficacy and favorable tolerability profile compared to other classes. 3 –5
At the time of data collection, licensed INIs in Italy were raltegravir (RAL), elvitegravir (EVG)/cobicistat, and dolutegravir (DTG): RAL was the first INI approved [US Food and Drug Administration (FDA), October 2007; European Medicines Agency (EMA), January 2008] and as such was prevalently used in experienced, multifailed patients; EVG was then approved, initially (FDA, August 2012; EMA, May 2013) exclusively as a component of a single-tablet regimen, while DTG, although being the most recently approved INI (FDA, August 2013; EMA, November 2013), has now become one of the most used ARV drugs, thanks to its high genetic barrier and convenient dosing. 6
The efficacy of INI has been widely described in different works, 7,8 but studies from clinical practice have questioned the optimal tolerability profile of this class of ARV, 9 –11 showing unexpected high rates of toxicity-related discontinuations. However, data from large cohorts, in particular, regarding experienced patients are still lacking.
We aimed to compare, in a real-life scenario, the durability of all three INIs in both treatment-naive and experienced HIV-positive patients in our multicenter cohort (the ODOACRE Cohort). 12 ] The clinical centers involved in this study (listed in Table 1) take care of about 15,000 people living with HIV (PLWHIV), more than 10% of the estimated PLWHIV in Italy (130,000). 13 About half of them, at some point, started an INI-based strategy. In this study, we also intend to investigate reasons for INIs discontinuation and differences between them.
List of Clinical Centers Involved in the Study
Materials and Methods
We retrospectively analyzed a cohort of HIV-1 infected adult (age ≥18 years) patients, both treatment-naive and -experienced, from nine Italian clinical centers (the list of clinical centers is described in Table 1) belonging to the “ODOACRE cohort,” starting an INI-based ARV regimen between January 2008 and December 2018. Primary endpoint was the time to treatment discontinuation (defined as the discontinuation of DTG, RAL, or EVG, regardless of whether the remaining ARV drugs used in the combination had been stopped or not).
We collected baseline characteristics (age, sex, HIV-risk factor), as well as patients' clinical history and viroimmunological parameters at baseline; reasons for INI discontinuations were also collected. Censor was defined as death, suspension of the INI, or the date of the last virological determination.
Chi-square test and nonparametric tests were used to assess differences in categorical and continuous variables, as appropriate. Kaplan–Meier survival analysis was performed to estimate the probability of maintaining the study drug and Cox-regression analysis to evaluate predictors of discontinuation. Multivariable models were adjusted for naive status, calendar year, and for significantly different variables between INIs at baseline.
The study was approved by each local Ethics Committee (protocol number of the promoting center: 5,284/15) and all patients signed informed consent for data collection.
Results
We enrolled 4,343 patients: 3,143 (72.4%) were males, with a median age of 49 years [interquartile range (IQR) 41–55]. Median peak HIV-RNA was 5.04 log10 copies/mL (IQR 4.50–5.51), while median CD4+ cell nadir was 171 cell/mm3 (IQR 48–304). Treatment-naive patients were 733 (16.9%), of whom 168 (22.9%) were AIDS presenters. As to experienced patients, their median time from HIV diagnosis was 16 years (IQR 8–23), with a median time from ARV initiation of 13 years (IQR 4–21); among experienced patients, 2,696 (76.2%) had a HIV-RNA ≤50 cp/mL at baseline. Overall, 2,282 patients (52.5%) started a DTG-containing regimen, 1,426 (33.1%) a regimen containing RAL, and 635 (14.7%) EVG. Full patients' characteristics are available in Table 2.
Characteristics of the Study Population
p Values were evaluated between the three groups.
ARV, antiretroviral; CDC, Center for Disease Control and Prevention; CNS, central nervous system; GI, gastrointestinal; IDU, intravenous drug users; INI, integrase strand transfer inhibitor; IQR, interquartile range; MSM, men who have sex with men; NNRTI, non nucleoside reverse transcriptase inhibitor; NRTI, nucleoside reverse transcriptase inhibitor; PI, protease inhibitor; TE, treatment-experienced patients.
During 10,032 patient years of follow-up (PYFU), we observed 1,278 discontinuations, with a cumulative rate of 13 per 100 PYFU. Three hundred thirty-one (14.5%) discontinued DTG, 812 (56.9%) discontinued RAL, while 135 (21.3%) discontinued EVG. Median time to INI discontinuation was 13 months (IQR 4–33). Discontinuations in the first year of follow-up (“early” discontinuations) were 572—221 in the DTG group (66.7% of group's overall discontinuations), 260 in the RAL group (32.0%), and 91 in the EVG group (66.9%). Difference in discontinuation rate in the first year between the three analyzed groups was statistically significant (p < .001).
As to the reasons for INI discontinuations, 448 (35.0% of total discontinuations) were due to simplification, 355 (27.8%) to toxicities (98 of which were due to neuropsychiatric events), 145 (11.3%) to virological failure, 69 (5.4%) to death, 35 (2.7%) to drug–drug interactions, and 227 (17.7%) to other/unknown causes. Reasons of discontinuation were different between INIs, as shown in Table 3.
Reasons for Integrase Strand Transfer Inhibitor Discontinuation
Estimated probabilities of maintaining DTG at 2, 3, and 4 years were 84.7% [95% confidence interval (CI): 83.9–85.5], 81.5% (95% CI: 80.5–82.5), and 76.3% (95% CI: 73.9–78.7), respectively; for RAL, they were 69.2% (95% CI: 67.9–70.5), 61.6% (95% CI: 60.2–63.0), and 54.1% (95% CI: 52.7–55.5), while for EVG, they were 77.2% (95% CI: 75.8–78.6), 71.6% (95% CI: 69.2–74.0), and 68.3% (95% CI: 65.3–71.3) (Fig. 1). Differences between groups were statistically significant (log-rank p < .001).
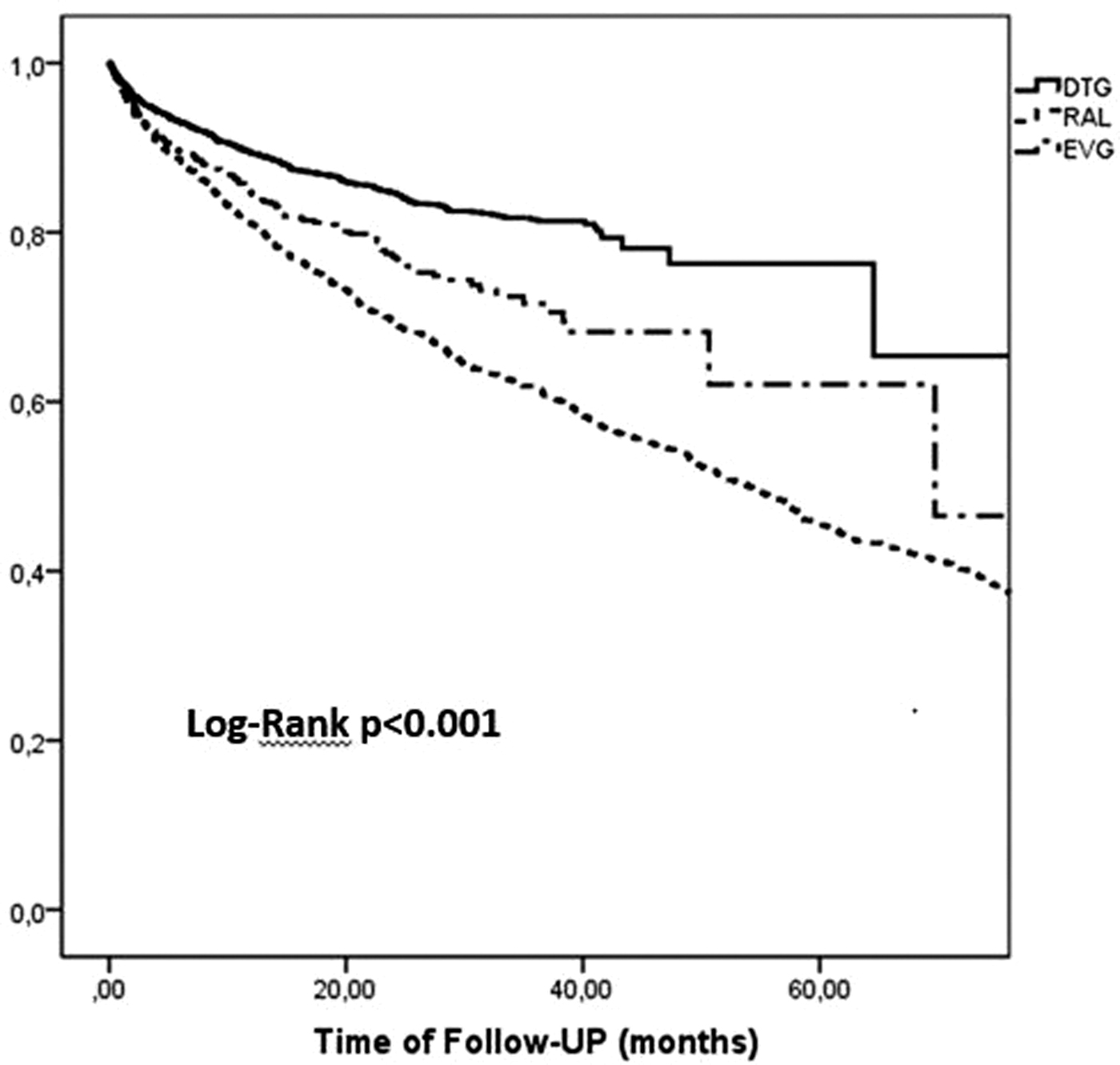
Estimated probability of maintaining study drug (overall population).
At a multivariable analysis, being on a RAL-based regimen [compared with DTG, adjusted hazard ratio (aHR) 2.9, 95% CI: 2.3–3.6, p < .001], a EVG-based one (vs. DTG, aHR 1.3 95% CI: 1.1–1.7, p = .049) and a peak HIV-RNA over 500,000 copies/mL (aHR 1.3, 95% CI: 1.1–1.6, p = .006) predicted INI discontinuation, after adjusting for calendar year, naive status, age, sex, HIV risk factor, time of virological suppression, years of HIV, and CD4+ cell nadir.
Considering only treatment-naive patients, probability of maintaining DTG was 78.7 (95% CI: 76.2–81.2) at 2 years, 77.1% (95% CI: 74.4–79.8) at 3 years, and 72.6% (95% CI: 67.5–78.1) at 4 years. Probabilities for RAL were 54.1% (95% CI: 50.4–57.8), 45.6% (95% CI: 41.8–49.4), and 40.4% (95% CI: 36.3–44.2), while for EVG they were 73.3% (95% CI: 69.1–77.5), 65.6% (95% CI: 60.6–70.6), and 58.5% (95% CI: 52.0–65.0), respectively. In this subanalysis, starting a first-line RAL-based regimen (compared with DTG, aHR 3.32, 95% CI: 2.1–5.2, p < .001) and a concomitant AIDS-defining event (aHR 1.65, 95% CI: 1.01–2.71, p = .045) resulted predictors of INI discontinuation.
Evaluating discontinuations due only to toxicities, we did not find a significant difference between INIs using Kaplan–Meier survival analysis and Cox regression analysis (log-rank p = .064, Fig. 2); in this specific analysis, male sex (vs. female, aHR 0.65, 95% CI: 0.44–0.96, p = .030) was reversely associated with drug discontinuation. Reasons for stopping study INI were significantly different between males and females (p < .001); in particular, among women, 8.7% of the total discontinuations were due to GI toxicity, 2.3% to renal toxicity, and 6.7% to neuropsychiatric events. Meanwhile, among males, the observed percentages were 5.4%, 3.5%, and 8.2%, respectively.
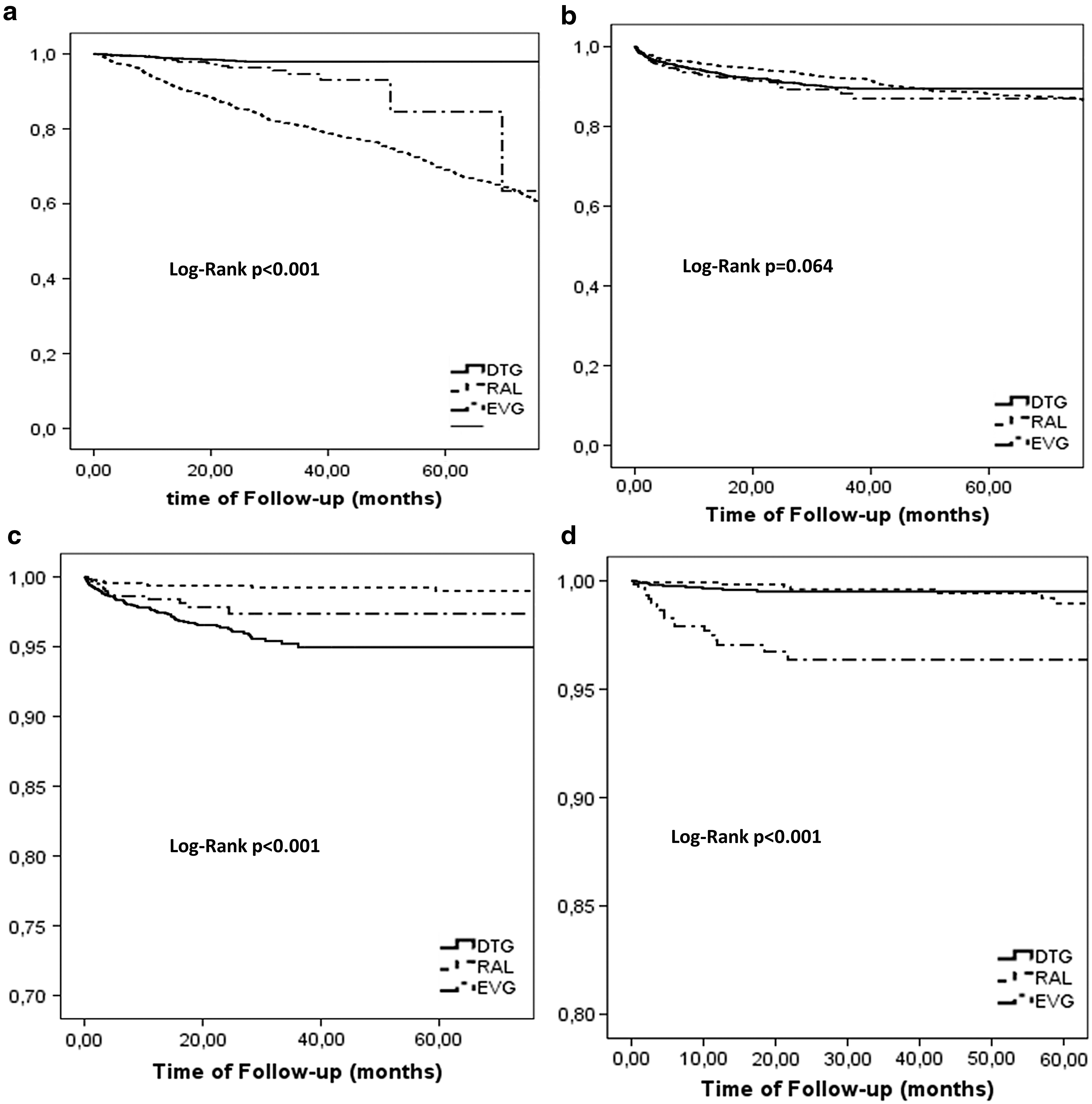
Estimated probabilities of maintaining study drugs (subanalysis):
A specific subanalysis on discontinuation due only to neuropsychiatric toxicity, found significant differences between groups (log-rank p < .001); a previous INI exposure (aHR 1.9, 95% CI: 1.1–3.3, p = .017) was associated with the event, while being on a RAL-based regimen (vs. DTG, aHR 0.1, 95% CI: 0.1–0.5, p = .004) or on a EVG-based one (vs. DTG, aHR 0.4, 95% CI: 0.2–0.9, p = .035) was inversely associated.
We also observed significant differences between groups in estimated probabilities of INI discontinuations due to drug–drug interactions (log-rank p < .001) and simplification (log-rank p < .001). In our cohort, being on a EVG-based regimen (vs. DTG, aHR 8.4, 95% CI: 3.0–23.0, p < .001) independently predicted discontinuation due to drug–drug interaction. Discontinuation of study INI due to simplification, meanwhile, was predicted by being on a RAL-based regimen (vs. DTG, aHR 20.0, 95% CI: 11.3–35.2, p < .001) or a EVG-based one (vs. DTG, aHR 2.4, 95% CI: 1.1–5.7, p = .042), while it was inversely associated with time of ARV exposure (aHR 0.96, 95% CI: 0.92–0.98, p = .024). As to patients discontinuing RAL due to simplification, 258 of them (65.0%) started a ARV regimen containing another INI (177 with DTG).
Discussion
In our multicenter cohort, we found differences in durability of the three integrase inhibitors available in Italy at the time of data analysis. Overall, the probability of maintaining DTG was higher compared with those of RAL and EVG both in treatment-experienced and naive patients, a finding in line with previous studies. 14,15 However, no difference was found regarding discontinuations due to toxicity between groups, confirming the good tolerability of the whole integrase inhibitors drug class observed in other cohort studies. 16
Central nervous system toxicity was a particular concern, not only for patients taking DTG 17 but also for those on other INIs. 11 In our cohort, we found that patients taking DTG-based regimens were more prone to discontinue following neuropsychiatric events compared with the other INIs, a finding that confirms results from other cohorts. 18,19 Central nervous system toxicity was the leading cause of DTG interruption in our cohort.
However, as recently pointed out by Llibre et al., 20 there is the possibility that Clinicians' awareness, following initial reports on the association between DTG and neuropsychiatric events, had a significant biasing effect. On the contrary, the favorable dosing and the high efficacy, shown as part of 2DR, 21,22 make DTG the drug less likely to be stopped due to simplification.
The higher probability of stopping EVG due to drug–drug interaction could be explained by the need of a pharmacokinetic booster.
Early (≤1year) discontinuations were lower in the RAL group compared with the other two. This finding could be explained by the different use that was made of RAL when it was first approved; being the first INI available, in fact, led clinicians in using RAL prevalently in heavily experienced patients, while DTG and EVG in our cohort were started mainly because of simplification or dyslipidemia.
Strengths of our study include the size of the population, one of the largest described, representing different clinical experiences, as well as the length of follow-up; these features make it possible to best reflect clinical practice. As to the main limitations, the most important is the high number of discontinuations due to unknown reasons. In addition, the three groups are very different, mainly due to the fact that the three molecules were introduced into the clinical practice in different time points and were used often in the context of different ARV strategies, although during analysis, we tried to correct this bias, by adjusting for differences between groups. Finally, other limitations are the retrospective design of the study and the fact that adverse events not leading to drug discontinuations were not collected.
In conclusion, our data confirm the good tolerability of INIs in clinical practice, with some differences between the three analyzed drugs regarding reasons for discontinuation.
Footnotes
Authors' Contributions
A.C., G.B., and S.D.G. contributed to the conception and design of the study. A.C. and G.B. contributed to the draft of the article. V.B., G.S., G.M.,
Acknowledgments
Collaborators in ODOACRE group: Alberto Borghetti, Roberto Cauda, Luigi Celani, Alex Dusina, Silvia Lamonica, Francesca Lombardi, Claudio Maria Mastroianni, Davide Moschese, Enrica Tamburrini (Roma), Arianna Emiliozzi, Barbara Rossetti (Siena), Cristina Mussini (Modena), Sergio Babudieri, Andrea De Vito (Sassari), Carlo Torti, Enrico Maria Trecarichi (Catanzaro), Maria Vittoria Cossu, Massimo Galli, Andrea Giacomelli, and Giuliano Rizzardini (Milano).
Author Disclosure Statement
G.B. received travel grant from Gilead Sciences. G.S. has received funds for speaking by Gilead, Merk, Janssen, Abbvie, and ViiV. G.M. reports personal fees from Gilead Sciences, Janssen-Cilag, Merck Sharp & Dohme, ViiV Healthcare, outside the submitted work. A.C. has received a personal grant from AB, Gilead, and ViiV. S.R. received research grants to his Institution from ViiV Heathcare, Gilead Sciences, and Janssen, outside the submitted work; he was also a paid consultant for ViiV Heathcare, Gilead Sciences, Merck Sharp and Dohme, Bristol-Myers Squibb, and Janssen. S.D.G. was a paid consultant or member of advisory boards for Gilead, ViiV Healthcare, Janssen-Cilag, Merck Sharp & Dohme and Bristol-Myers Squibb. All other authors (A.F.C., V.B.,
Funding Information
This study was conducted during our routine clinical activity.