
Abstract
Frailty is associated with an increased probability of serious adverse health outcomes in the geriatric general population. People living with HIV have a higher prevalence of frailty. However, the magnitude of this problem in younger patients in South America is unknown. We aimed to determine the prevalence and factors associated with frailty. This is a cross-sectional study from the Brazilian cohort HIV-AIDS (CoBRA) developed between March and November of 2018, on patients ≥18 years of age. Frailty phenotype was assessed by original Fried criteria. The results were analyzed using descriptive statistics, while identification of factors related to frailty was assessed by using multivariate logistic regression. We enrolled 231 patients; all, but 2 were on antiretroviral therapy (ART). Median age was 45.6 interquartile range (36.7–52.1) years, 136 (58.9%) were male, and 86.7% self-identified as non-white. Mean CD4 count was 660 (±345) cells/mm3 and 83.5% had undetectable HIV plasma viral load (<50 copies/mL). Prevalence of frailty and prefrailty was 10.4% and 52.4%, respectively. A CD4 count <200 cells/mm3, depression, low income, and use of third-line ART were variables significantly associated with a greater risk to present frail or prefrail status. Frailty prevalence increases with age and is an important health problem to health care in HIV aging patients. It requires proper strategies to its early detection, prevention, and management.
Introduction
Frailty is recognized as a geriatric syndrome characterized by decreased physiological reserve, increased vulnerability to stressors, and reduced ability to compensate for homeostasis disruptions involving multiple physiologic systems. This leads, in consequence, to an increased probability of serious adverse health events, including falls, disability, institutionalization, hospitalization, and death. 1 –4 The increase of frailty with low CD4 T cell count and high HIV viral load, two biomarkers of HIV disease progression, suggests a common underlying mechanism for frailty and HIV disease. 6
Many approaches for measuring frailty have been proposed, including Fried's frailty phenotype (FFP), an instrument that includes both subjective and objective components. FFP is associated with increased morbidity and mortality in elderly persons. The presence of FFP in cohorts of younger HIV-infected individuals predicts a higher risk for loss of functional independence or decline in functional status. 5 –7
Successful antiretroviral therapy (ART) increased the life expectancy for people living with HIV (PLWHIV). Nevertheless, the available evidence suggests that PLWHIV can present an accelerated aging process. 8,9 Persistent and chronic activation of the immune system lead to immune exhaustion and accelerated immunosenescence, even in patients presenting stable viral suppression and normal levels of CD4+ cells. 9 This seems to increase the prevalence of aging-related noncommunicable diseases (including frailty), which can occur 10 to 15 years earlier in PLWHIV than in the general population. 9,10
Prevalence of frailty in HIV population ranges from 5% to 28.6%, and is associated with female sex, lower educational attainment, unemployment, low annual income, presence of major comorbidities, low CD4 cell count, and detectable viral load. 11 Recently, the first study on frailty developed on Brazil detected a 19.4 frailty prevalence among HIV adults older than 50 years. 12
Despite the evidences suggesting an accelerated aging process for PLWHIV, 9,13,14 there is scarce information on frailty in younger patients, in developing countries. The extent of this problem is unknown for younger adults in South America, and a cutoff point for a frailty screening in this population has not yet been determined. We aimed to evaluate the frequency and associated factors of FFP, in a study involving PLWHIV 18 years of age or older.
Materials and Methods
This is a cross-sectional study conducted in PLWHIV, conducted between March and November of 2018. Participants were individuals attending the AIDS outpatient clinics at Complexo Hospitalar Universitário Professor Edgard Santos (C-HUPES) from Universidade Federal da Bahia (UFBA), a public HIV referral service in Salvador, Brazil. Participants were eligible if 18 years of age or older. We excluded patients with a recent history of hospitalization (<30 preceding days), pregnant woman, and wheelchair users. Use of a cane or other instruments to aid walking was permitted. Informed consent was obtained from all participants. The study is part of the Coorte Brasileira de HIV-AIDS (CoBRA) and was conducted according to Helsinqui's Declaration. The study was approved by the institutional ethics in research committee (approval number: 1.035.826, data: April 26, 2015).
Participants completed a structured questionnaire and an assessment of frailty, functional dependency, and depression, in a single day. Additional clinical information was retrieved from physical and electronic medical records and from a national database (Laboratory Control System of the National Network for Lymphocyte Count, CD4+/CD8+, and HIV Viral Load-SISCEL).
Demographics
We recorded information like age, sex, self-reported skin color, marital status, education, occupational status, and individual income. We stratified education into two categories, <9 years versus >9 years of study. Individual income was dichotomized into less or equal to one minimum wage (954 Brazilian Reais, around USD 228.00 for 2018) versus monthly higher income. We defined current occupation as current involvement in any productive activity, including two categories: employed or studying versus unemployed or retired. In addition, age was stratified in three groups: <40, 40–50, and >50 years.
Substance use
Tobacco use was defined as current, former, or never smoker. Alcohol use was considered yes or no current use, and assessed with Alcohol Use Disorders Identification Test AUDIT 15 adapted and validated to Brazilian population. 16
Illicit drug use was defined as current use of marijuana, crack, lysergic acid diethylamide (LSD), cocaine, or injectable drugs.
Frailty assessment
Original components of the Frailty Phenotype defined by Fried et al. 2 were used to identify frail participants. Weight loss was defined as unintentional weight loss of at least 5%; we compared previous year's body weight with current weight. Exhaustion was identified using two questions from the Center for Epidemiologic Studies Depression Scale (CES-D Scale), 17,18 and subjects answering “2” or “3” to either of these questions were categorized as frail. We used the Portuguese version of Minnesota Leisure Time Activity questionnaire to assess physical activity level. 19 Weekly expended kcals were calculated using standardized algorithm, and stratified by gender. Men and women were considered frail if they reported an expenditure of <383 and <270 kcal/week, respectively. Weakness was assessed by grip strength measure using an electronic hand dynamometer (E•Clear - model EH 101) and obtaining the average of three dominant hand measurements. Results were stratified by gender and body mass index (BMI) quartiles. Slowness was assessed with the mean of three measures of the expended time to walk 4.6 m at usual pace, stratified by gender and height. We used cutoff points established by Fried et al. 2 to define frail individuals. Participants presenting three or more positive criteria were classified as frail, one or two positive criteria as prefrail, and no positive criteria as robust or nonfrail. We measured height in meters, weight in kilograms, and BMI in (kg/m2).
Frailty-related events
We asked the participants about any fall in the last 12 months. If they answered yes, number of falls and consequent hospitalization were recorded. Hospitalization, if any (more than 24 h at hospital), due to other causes than fall, in the last 12 months was also recorded. To assess self-perception of health, we used one question from the Questionnaire Short Form 36 Health Survey, 20 “In general, would you say your health is: Excellent, Very good, Good, Fair, Poor” and dichotomized as Good (Excellent, Very good, and good) or Fair (Fair and Poor). Polypharmacy was defined as the current use of more than three different medications, excluding ART.
Clinical assessments
Medical history was asked to the patients during the interview through a structured questionnaire. In addition, we reviewed clinical data in the physical and virtual medical records, including chronic condition and disease diagnosis such as systemic arterial hypertension, diabetes, dyslipidemia, osteoporosis, cancer, and chronic kidney disease. Confections by human T-limphotropic virus (HTLV), Hepatitis B, Hepatitis C, and Tuberculosis, and history of AIDS-defining conditions were also recorded.
We stratified BMI into three categories, underweight (<18.5), normal weight (18.5–25), and overweight (>25) kg/m2.
HIV-related characteristics
We also recorded the time elapsed between the year of HIV diagnosis and the year of enrolment in this study, and first and last recorded HIV-RNA plasma viral load (PVL)/CD4 cell count. PVL suppression was defined as HIV RNA <50 copies/mL at the moment of inclusion in the study. For analysis purposes, last and first CD4 cell count were stratified as ≤200 cells/mm3 or higher. Last and first PVL were also categorized as detectable PVL or not detectable. All alasta laboratory results were performed in a window of 6 months of inclusion in study.
Current antiretroviral treatment regimens (ART) were retrieved from medical records, and analyzed as a class, and drug by drug.
Depression assessment
Depression was evaluated by using The CES-D Scale, 18 validated to Portuguese language. 17 It is composed of 20 items and uses 16 cutoff points to define or exclude depression. We excluded two questions from the CES-D because they are used as a FFP criterion, and maintained the same cutoff as previously done at AGEhIV Cohort Study. 21
Functional dependency
Functional dependence was evaluated using the Scale of Instrumental Activities of Daily Living (IADL) developed by Lawton and Brody, 22 and adapted to Brazilian context. 23 It classifies participants as independent; partially dependent; and totally dependent if 21; 6–20; and ≤5 points on the scale score, respectively.
Statistical analyses
We used descriptive statistics to present participant's characteristics. For categorical variables, we used frequency and proportion, while for continuous variables, mean and standard deviation or median with interquartile range, when appropriate, was used. In the univariate analysis, comparison between categorical groups was performed using chi-square or Fisher's exact test. For continuous variables, we used independent t-test, analysis of variance, or nonparametric tests, as required.
Bivariate analysis was performed and variables presenting with a p value <.10 were selected for the multivariate model, excluding those that had a high collinearity value (education, marital status, living alone, viral load, and in use of dolutegravir [DTG] or darunavir [DRV]). To perform multivariable analysis, we excluded individuals who had missing data (n = 19) on the variables selected for the regression model (depression, wages, and third line of ART). For the selection of the predictor variables, bivariate logistic analysis was performed using the conditional backward to identification of factors related to FFP.
Statistical analyses were performed using SPSS software, version 18.0 for Windows.
Results
A total of 231 subjects were enrolled. Median age was 45.6 years (range 36.7 to 52.1 years), 136 (58.9%) were male, and 86.7% self-identified as non-white. Mean CD4 count was 660 ± 345 cells/mm3, 83.5% had undetectable HIV PVL (<50 copies/mL). All, but two participants, who were elite controllers, were on ART (Tables 1 and 3 depicts the main characteristics of patients).
Sociodemographic-Related Characteristics of the Study Population According to Frailty Status
Data are n (%) of participants.
Only age is represented into median (IQR).
Brazilian fundamental education are the first 9 years of schooling.
Brazilian minimum wage was 954 Brazilian Reais or around USD 228.00 for 2018.
IQR, interquartile range.
Frailty-Related Events According to Frailty Phenotype Groups
Data are n (%) of participants.
Falls, defined as any fall on the last 12 months.
Hospitalization, if more than 24 h at hospital.
Polypharmacy, defined as current use of more than three different medications, excluding ART.
Functional dependency was assessed using the Scale of IADL developed by Lawton and Brody adapted to Brazilian context.
Depression was evaluated by using The CES-D Scale, we excluded two questions from the CES-D because they are used as a, FRP criterion, and maintained the same cutoff of ≥16 point to define depressed.
ART, antiretroviral therapy; CES-D Scale, Center for Epidemiologic Studies Depression Scale; FRP; IADL, Instrumental Activities of Daily Living.
Frailty prevalence was 10.4% (n = 24), 52.4% (n = 121) were prefrail, and 32.7% (n = 86) were robust. The prevalence of frail, prefrail, and robust status was 6.6%; 50.0%; and 43.4%, respectively, for patients <40 years of age, and 8.6%; 50.6%; and 40.7% for those 40–50 years of age. For patients older than 50 years, the prevalence was 16.2%, 56.8%, and 27.0% for those categories. The proportion of patients classified as frail and prefrail increased with age, while proportion of patients classified as robust decreased, as shown in Figure 1. The most frequent positive criterion for frailty was grip strength (27.3%), followed by exhaustion (27.3%), low physical activity (27.3%), weight loss (14.3%), and slowness (3.9%).
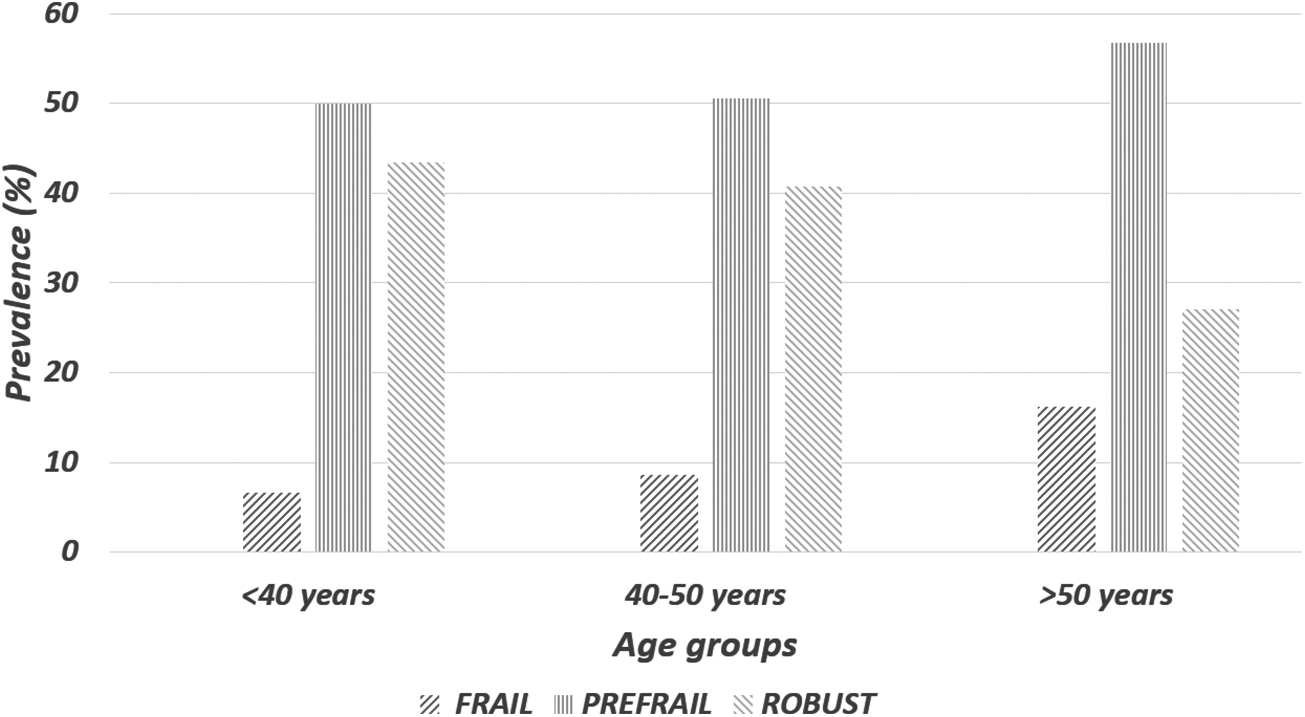
FFP by age groups. The prevalence of frail, prefrail, and robust status was 6.6%, 50.0%, and 43.4%, respectively, for patients <40 years of age, and 8.6%, 50.6%, and 40.7%, for those 40–50 years of age. For patients older than 50 years, the prevalence was 16.2%, 56.8%, and 27.0%, for those categories. The proportion of patients classified as frail and prefrail increased with age, while proportion of patients classified as robust decreased. FFP, Fried's frailty phenotype.
In bivariate analysis, significant associations were found between frailty and age, female sex, unemployed or retired persons, lower income, fair self-perception of health, falls, hospitalization, polypharmacy, partial functional dependency, depression, underweight, last CD4 count ≤200 cells/mm3, current detectable HIV-RNA PVL, first CD4 count ≤200 cells/mm3, current use of INSTIs, and third-line ART current use (Tables 1–4 summarize the main findings in the study population).
Distribution of Clinical Chronic Conditions, Confections, and Substance Use According to Frailty Phenotype Groups
Data are n (%) of participants.
Medical history about current and past clinical conditions was asked to the patients during the interview through a structured questionnaire. In addition, we reviewed and added clinical data in the physical and virtual medical records.
BMI was stratified into three categories, underweight (<18.5), normal weight (18.5–25), and overweight (>25) kg/m2.
We considered decreased kidney function (estimated glomerular filtration rate <60 mL/min/1.73 m2) by the CKD-EPI equation.
AUDIT (Alcohol Use Disorders Identification Test) and classifies alcohol consume into Zone I (Low risk), Zone II (Risky), Zone III (Harmful), Zone IV (Severe).
AIDS, Acquired Immune Deficiency Syndrome-Defining Conditions; AUDIT, Alcohol Use Disorders Identification Test; BMI, body mass index; HTLV, human T-limphotropic virus.
For comparison purposes, we used robust group as reference to assess the risk of frail or prefrail status. In a multivariate logistic regression analysis, we detected a higher risk of frail or prefrail status among subjects with a CD4 count <200 cells/mm3. Depression, low income, and use of third-line ART were also associated with a higher risk of frail or prefrail status, as shown in Table 5.
Binary Logistic Regression Comparing the Groups According to Fried's Frailty Phenotype Status
CI, confidence interval; aOR, adjusted odds ratio.
Discussion
We found a 10.4% prevalence of frailty, 52.4% of prefrailty, and 37.2% of robust, on a sample of people older than 18 years living with HIV. Among the factors associated with FFP, depression was a constant and strong association. Lower income, use of a third-line ART, along with the low CD4 level (<200 cells/mm3 count) characterized a vulnerable population. We did not find other associations between frailty and frailty predictors previously described by Levett et al., 11 such as Hepatitis C co-infection, chronic kidney disease, or diabetes mellitus. The only comorbidities significantly associated with frailty in our study were low BMI and osteoporosis.
Among our Brazilian PLWHIV cohort of predominantly middle-aged participants, with regular outpatient care and on successful ART, we found a frailty prevalence of 10.4%. This is in accordance with previous studies in this age population that reported similar frailty prevalence. 24,25 The detected frailty prevalence among individuals older than 50 years in our study was 16.2%, which seems to be slightly lower than that found in a previous Brazilian study 12 However, that study population was characterized by a high burden of chronic comorbidities, with 56.7% of the participants having at least one comorbidity, and a higher median age (55 years, range 50 to 83). In this study, most patients (52.4%) presented with no comorbidity, and the median age was 45.6 years (range 18 to 78).
Frailty prevalence ranged from 5.0% to 28.6% in literature, depending on the cohort studied. However, the characteristics of studied populations were heterogeneous and not all of them used the original frailty criteria proposed by Fried et al. 11 One previous Brazilian study (FIBRA) 26 conducted on non-HIV elder Brazilian people (mean age of 73.08 ± 6.17 years) found a frailty prevalence of 11.2%, but the age was much higher than that observed in our study population (median 45.6 years). Our findings suggest an earlier occurrence of frailty on HIV population, and a higher prevalence when compared with non-HIV population. 6,9,27,28 One characteristic of the frailty syndrome, (which distinguishes it from the effects of ordinary aging), is the potential reversibility of many of its features, 29,30 making HIV population an important group for intervention.
Socioeconomic factors were also associated with frailty status: in the bivariate analysis, we found significant associations between frailty and patients living alone, unemployed or retired, and receiving a low per capita income. Socioeconomic disadvantages had been linked to cumulative biological risk profiles 31 ; inflammation, 32 decreased physical tone, 33 decreased serotonin, 34 and decreased access to micronutrients 35 are factors that contribute to frailty status. It is clear that both, frailty and low socioeconomic status, are risk factors for illness and mortality. 36,38
Female sex could confer intrinsic risk of frailty due to the fact that women start with lower lean mass and strength than age-matched men, and also experience earlier muscle mass loss. 37,39 In addition, older women have a greater likelihood of inadequate nutritional intake, compared to men, because they are more likely to live alone. 2 Greater accumulation of muscle mass in males and higher levels of testosterone may protect them from developing frailty in old ages. 40 We could not include sex into our prediction model due to collinearity with age in our sample: in a secondary analysis, 100% of frail male participants were younger than 50 years and 68.8% of women older than 50 years were frail. Depression and frailty both predict disability and morbidity in later life. 41 Prevalence of depressive symptoms in frail non-HIV participants 55 years of age or more ranged from 20.7% to 53.8% in a previous study. 42 Our results show a higher prevalence of depression (65.2%) in the frail group and show depression as a constant variable across all of the FFP status. Some authors consider frailty a “predisability” state, in which a stressor can trigger the progression to disability. 43 Depression and frailty share symptoms such as low daily activity profiles, which could result from either decreased energy reserve (in both frailty and depression) and loss of interest (anhedonia in depression) or loss of ability to engage in daily life activities (functional impairment) (42). While it is clear that symptoms of depression and frailty tend to co-aggregate, the factors that drive this overlap are unclear, although a longitudinal study showed that frailty was an independent predictor of incident depressive symptomatology in similarly adjusted models (odds ratio = 1.86; 95% confidence interval = 1.05–3.28). 46 Our findings indicate there is a strong association between frailty and depression that is also related to disease severity and serious adverse events like falls, hospitalizations, and functional impairment.
Third-line antiretroviral drugs are recommended to patients with confirmed virological failure, genotyping test performed, or resistance to at least one antiretroviral from each of the three classes (nucleoside reverse transcriptase inhibitor, non-nucleoside reverse transcriptase inhibitor, and protease inhibitor). Dolutegravir had the same use recommendations of third line when introduced in 2015, 44 and was incorporated only in May 2017 for first-line preferential treatment, although it continues to be used as a salvage drug in cases of therapeutic failure. 45 Our findings on the association of these two drugs with frailty can be interpreted as an indirect evidence of several previous treatment failures, in heavily experienced patients.
Our findings have some limitations: the cross-sectional design of our study precludes any conclusion on causality. In addition, we used only the FRP as the criteria to define frailty, which could influence the overall estimate of frailty in our population. However, in this sample of patients, we could demonstrate that frailty is highly prevalent in our HIV population, and affects even patients at an younger age. In addition, our study population was a well-defined group, with extended follow-up at a referral center, making them a well-characterized group that could represent the population living with HIV-AIDS in Bahia, Brazil. These characteristics made possible to establish associations between several risk factors and progression across the FFP spectrum.
Conclusions
Our study is the first one developed on South America that includes younger PLWHIV. We were able to detect a high frailty and prefrailty prevalence that increase with age. Our results demonstrate that frailty is an important health problem in aging HIV patients and requires strategies to its early detection, prevention, and management.
Footnotes
Acknowledgments
We thank all study volunteers, the Federal University of Bahia, Post-graduate Program in Medicine and Health (PPgMS)/UFBA, and the LAPI—Research Laboratory of Infectious Diseases.
Author Disclosure Statement
The authors declare no conflicts of interest.
Funding Information
“This study was financed, in part, by the Coordenação de Aperfeiçoamento de Pessoal de Nível Superior—Brasil (CAPES)—Finance Code 001.” The funder had no role in study design, data collection, data analysis, data interpretation, or writing of the report.