
Abstract
Introduction:
In patients with HIV in antiretroviral treatment (ART) and virological failure to the first-line regimen, establishing a therapeutic regimen after having identified the M184V mutation, which confers ART resistance, represents a dilemma.
Objective:
To compare the virological response of the therapeutic regimens prescribed to patients with HIV who presented the M184V mutation in two national hospitals in Lima, Peru, during the years 2008 to 2019, and to determine the risk factors associated with poor virological response.
Methods:
A retrospective cohort study was developed based on the information of the HIV program participants with the M184V mutation.
Results:
A total of 175 participants were eligible for the study. The male sex predominated (75.4%), the current median age was 41 years [interquartile range (IQR) 35.84–47.47], and the time on ART was 89 months (IQR 57.7–124.53). The median initial viral load (VL) was 4.5 log10 copies/mL (IQR 3.97–5.09) and the time between genotyping and the change of therapy was 2 months (IQR 0–3.56). The most used antiretroviral regimen was protease inhibitor plus two nucleoside reverse transcriptase inhibitors (55.4%). With the protease inhibitor plus integrase inhibitor (PI + INI) ART, 69% less risk of poor virological response was obtained [p = .019 (confidence interval 95% 0.117–0.825)].
Conclusions:
In patients with HIV and the M184V mutation, the PI + INI ART has shown a greater decrease in control VL and, thus, a good virological response. The risk factors associated with a poor virological response were the delay between genotyping and change of therapy, high levels of initial VL, and poor adherence among the participants.
Introduction
Antiretroviral treatment (ART) has changed the natural history of HIV infection, as it reduces its replication in peripheral blood, allows the reconstitution of the immune system, delays clinical progression to advanced stages, and reduces morbi-mortality. 1,2 Since its widespread implementation in 1996 in the United States, and 2008 as a national strategy in Peru, deaths due to AIDS have decreased by 48% (Refs. 3,4 ). Likewise, ART is the main strategy to prevent the spread of the disease since if the viral load (VL) is undetectable, people living with HIV do not transmit it through sexual exchange. 3,5
In general, everyone with HIV should start ART regardless of their clinical stage, CD4 T cell count, and VL. The World Health Organization (WHO) and the Peruvian “Norma Técnica de Salud de atención integral del adulto con infección por el VIH” recommend the use of two nucleoside reverse transcriptase inhibitors (NRTIs) and a non-nucleoside reverse transcriptase inhibitor (NNRTI) as a first-line regimen. 5,6 Then, periodic monitoring of the VL is necessary to detect a possible virological failure (VF). VF is defined as the persistence of VL >1,000 copies/mL in two consecutive measurements within a 3-month interval, 7 which reflects ongoing replication of HIV in patients treated with these antiretrovirals (ARVs). Thus, despite the success of ART, 24% of patients in Peru have VF, which constitutes a clinical problem due to the progression to advanced stages, and a public health problem due to the possibility of transmission of resistant strains to the population with the consequent appearance of primary resistance in contacts. 6,8 Once the VF has been identified, a genotyping study should be carried out to recognize an existing mutation and establish a second-line regimen. 7,9 In Peru, the choice of such a regimen is based on observational studies done in other populations, in which some frequent mutations have been established, its genotypic characteristics have been studied, and it has been correlated with the response in the patient.
Currently, it is known that the presence of some mutations not only confers resistance to certain ARVs but also confers hypersusceptibility, and therefore enhances other ARV. 10 This is the case of the M184V mutation, the most frequent, observed in 78% of the world population and 64.2% of the Peruvian population receiving ART. 11,12 Among ARV drugs belonging to NRTIs, this mutation causes resistance to lamivudine (3TC) and emtricitabine (FTC), but confers hypersusceptibility to zidovudine (AZT) and tenofovir (TDF); in addition, the ability of the virus to replicate decreases. For this reason, it might be useful to keep NRTIs in the second-line regimen to preserve the mutation and take advantage of its characteristics. Precisely, one could opt for a regimen consisting of two NRTIs associated with a protease inhibitor (PI) or not using NRTIs because they have already produced VF and, instead, use an integrase inhibitor (INI) associated with PI.
In Peru, the identification of the M184V mutation represents a dilemma regarding the therapeutic behavior to follow. Evidence has shown that a second-line regimen must have two fully active drugs. The physician may consider NRTIs as such or may choose to exchange them for an INI associated with PI. However, in this patient population, the evidence for which therapeutic regimen is associated with a better virological response is still scarce. Likewise, there are no studies in the Peruvian population that compare second-line regimens in patients with the M184V mutation. By analyzing the characteristics of patients with HIV, the results of control VL, and identifying the therapy associated with a better virological response, this study shows evidence of clinical and public health relevance.
We compared the virological response at 6 months of the therapeutic regimens prescribed to patients with HIV who presented the M184V mutation in two national hospitals in Lima, Peru, during the years 2008 to 2019 and determined the risk factors associated with a poor virological response.
Materials and Methods
Study design and context
The present retrospective cohort study was based on the information of the participants of the HIV program with the M184V mutation in two national hospitals in Lima, Peru, during the years 2008 to 2019.
Population
This census study was conducted in patients with HIV and M184V mutation of the Department of Infectious Disease of the “Arzobispo Loayza National Hospital” and “Daniel Alcides Carrión National Hospital” of Lima, Peru, during the years 2008 to 2019. The inclusion criteria of this study were to be older than 18 years of age diagnosed with HIV and in ART and having been prescribed any of the therapeutic study regimens such as PI + INI, PI + 2 NRTIs, or NNRTI + 2 NRTIs after identifying the M184V mutation. The exclusion criteria were not having control VL results after identification of the M184V mutation and having changed the prescribed therapeutic regimen during the study follow-up period (Fig. 1).
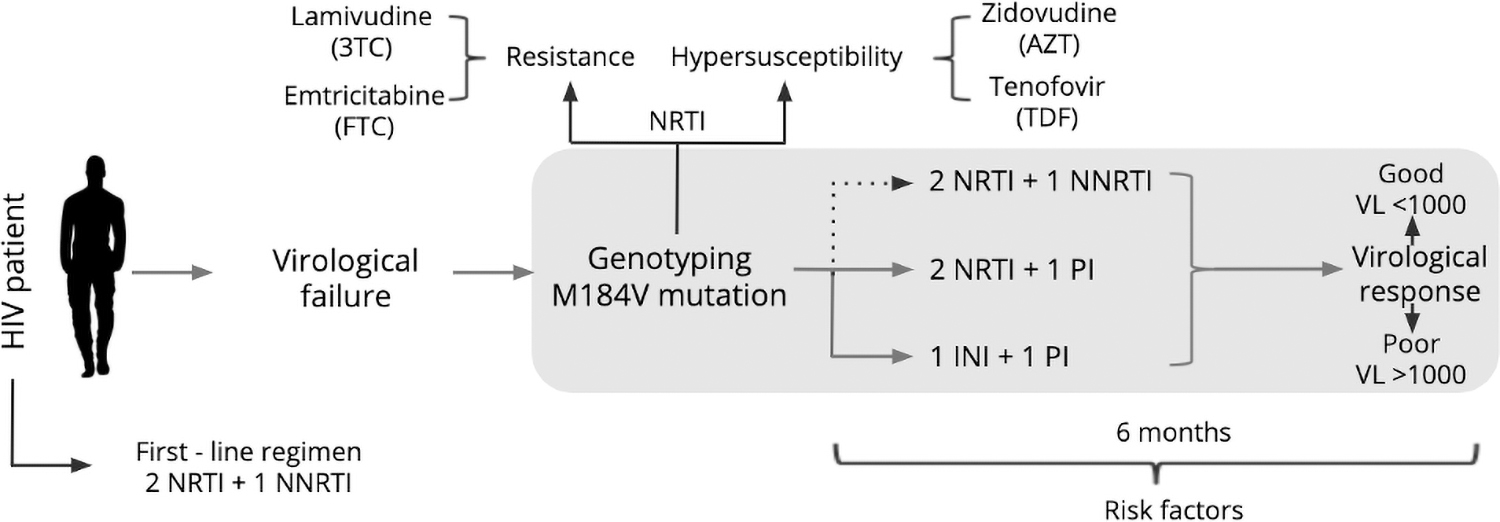
Population selection and study process. Every patient on first-line regimen needs a periodic monitoring of the VL to detect a virological failure. This should be followed by a genotyping study to recognize an existing mutation such as the M184V mutation, which not only confers resistance to certain ARVs but also confers hypersusceptibility to others. Once identified, physicians may consider a second line regimen composed of 2 NRTIs + PI or INI + PI with the aim of achieving a good virological response. ARVs, antiretrovirals; INI, integrase inhibitor; NRTI, nucleoside reverse transcriptase inhibitor; NNRTI, nonnucleoside reverse transcriptase inhibitor; PI, protease inhibitor; VL, viral load.
Variables definition
The main variables of this study were the prescription of a determined therapeutic regimen as an exposure variable and that included protease inhibitor plus integrase inhibitor (PI + INI), protease inhibitor plus two nucleoside reverse transcriptase inhibitors (PI + 2 NRTI) or a non-nucleoside reverse transcriptase inhibitor plus two nucleoside reverse transcriptase inhibitors (NNRTI + 2 NRTIs), and the virological response as an outcome categorized as good when the VL was <1,000 copies/mL and poor when the VL was >1,000 copies/mL after 6 months of the prescribed therapeutic regimen for patients with HIV who presented the M184V mutation. Likewise, other independent variables were established based on general data such as sex, current age, age at the identification of the M184V mutation, sexual orientation, educational level, and substance abuse; disease information such as time with HIV, time in ART, time between genotyping and change of therapy, time between change of therapy and control, adherence to treatment defined as the ratio in percentage of the total days the patient took the medication (total days it should have taken minus days of abandonment), and the total days to take the medication that must be >95% to be considered adherence, and chronic comorbidity; immunological information such as initial CD4 T cell count; and virological information such as initial and control VL.
Procedure
The genotyping results were obtained from the Instituto Nacional de Salud website (Net Lab). The information of the participants of the HIV program of the two national hospitals in Lima, Peru, was obtained through the Terapia Antiretroviral de Gran Actividad file belonging to an annex of the “Norma Técnica de Salud de atención integral del adulto con infección por el VIH.” Finally, a database was generated in an MS Excel 16 sheet based on the coding of the variables determined in the study.
Statistics analysis
The statistical software STATA 14.0 was used to analyze the data. In the descriptive analysis, the absolute and relative frequencies of the categorical variables were obtained (sex, sexual orientation, educational level, substance abuse, chronic comorbidity, adherence, virological response, PI + INI regimen, PI + 2 NRTIs regimen, and NNRTI + 2 NRTIs regimen), as well as the median and interquartile range of the nonparametric numerical variables (current age, age at mutation, time with HIV, time in ART, initial CD4 T cell count, initial VL, control VL, time between genotyping and change of therapy, and time between change of therapy and control). The bivariate analysis using the chi-square test explored the association between the virological response and the categorical variables. The Wilcoxon rank sum test explored the association between the virological response and the numerical variables. We use p < .05 as a significant cutoff point. In the multivariate analysis, Poisson regression was used to measure the strength of association (relative risk) between the virological response and the independent variables with 95% confidence intervals (CIs). In this analysis, the outcome was the virological response (dichotomous), the main exposure variable was the therapeutic regimens and the variables included in the adjusted multivariate analysis were those that had a value of p < .05 in the crude analysis such as time in ART, adherence to treatment, initial VL, time between genotyping and change of therapy, and the PI + INI therapeutic regimen.
Ethical aspects
The conduct of this study was reviewed and approved by the Ethics Committee of the Universidad Peruana de Ciencias Aplicadas. The corresponding permits were requested from the two national hospital authorities and those responsible for the Infectious Services parts of the study. In addition, the use of informed consent was exempted, since the information to be analyzed was obtained by secondary sources. The information of the participants of the HIV program of the two national hospitals in Lima, Peru, was handled anonymously through codes by the researchers. In this way, the confidentiality and nonexposure of personal data of the people part of the study to outsiders was guaranteed.
Results
Participant selection
This study was conducted in two hospitals from Lima-Peru, the Arzobispo Loayza National Hospital and the Daniel Alcides Carrión National Hospital. The possible population was 232 patients with HIV and the M184V mutation between 2008 and 2019. Of this number, 57 patients were excluded because they did not meet the eligibility criteria: 45 had no VL after genotyping and 12 patients were minors. In the end, a total of 175 participants were eligible for the study (Fig. 2).

Participants eligible for the study.
Descriptive analysis
The characteristics of the study participants are shown in Tables 1 and 2.
Characteristics of HIV Patients Who Presented the M184V Mutation in Two National Hospitals During the Years 2008 to 2019
n is the number of subjects of the categorical variables.
INI, integrase inhibitor; NRTI, nucleoside reverse transcriptase inhibitor; NNRTI, nonnucleoside reverse transcriptase inhibitor; PI, protease inhibitor; VL, viral load.
Characteristics of HIV Patients Who Presented the M184V Mutation in Two National Hospitals During the Years 2008 to 2019
m is the median and IQR is the interquartile range (p25–p75) of the numerical variables.
ART, antiretroviral treatment.
As for the demographic data, 75.4% were men, the median of the current age of the participants was 41 years, and the age at the time the M184V mutation appeared was 38 years. Overall, 27.4% were part of the homosexual population; the educational level was mostly secondary or higher (89.71%); 12.6% had issues with two or more kinds of substance abuse such as alcohol, drugs, or tobacco; and only 18.86% had one or more chronic comorbidities. Regarding the disease information, the patients lived with HIV for a median of 99 months, of which they received ART for 89 months, with 64.57% adherent to their therapeutic regimen since the identification of the mutation. With respect to virological information, the median VL at the time the mutation was identified was 4.5 log10 compared to the VL at control that was 1.8 log10. The median time between genotyping and change of therapy was 2 months, and the time between change of therapy and the control VL was 7.5 months. Finally, 68% of patients had a good virological response and the most commonly used regimen was the one made up of PI + 2 NRTIs (55.43%) followed by NNRTI + 2 NRTIs (26.86%).
Bivariate analysis
In the bivariate analysis, the following characteristics were associated (p < .05) with the virological response: adherence, initial VL, time between genotyping and change of therapy (months), and PI + INI regimen. For therapeutic regimen, the percentages of people with poor virological response were as follows: 13% for those who used the PI + INI regimen, 33% the PI + 2 NRTIs regimen, and 43% for the NNRTI + 2 NRTIs regimen. The median initial VL for those with poor virological response was 4.7 log10, compared with 4.4 log10 for those with good virological response. The median time between genotyping and change of therapy for those with poor virological response was 2.35 months compared to 1.8 months for those with good virological response. Forty-two percent of people without adherence experienced a poor virological response compared with 27% of people with adherence. The complete results of the bivariate analysis are shown in Tables 3 and 4.
Virological Response in Relationship to the Prescribed Therapeutic Regimen in HIV Patients Who Presented the M184V Mutation in Two National Hospitals During the Years 2008 to 2019
n is the number of subjects of the categorical variables. Chi-square test p-value to compare the virological response with the categorical variables.
Virological Response in Relationship to the Prescribed Therapeutic Regimen in HIV Patients Who Presented the M184V Mutation in Two National Hospitals During the Years 2008 to 2019
m is the median and IQR is the interquartile range (p25–p75) of the numerical variables. Wilcoxon ranks sum test p-value to compare the virological response with the numerical variables.
Regression model
In the multivariate model, the factors associated with poor virological response were explored and the RRc values were obtained for all variables.
Patients who used the regimen consisting of PI + INI had 70% less risk of poor virological response compared to those who used another regimen [p = .017 (95% CI 0.114–0.805)]. Patients who adhered to treatment had a 37% lower risk of poor virological response compared to nonadherents [p = .035 (95% CI 0.414–0.969)]. For every month of delay between genotyping and the change of therapy, there was an 8% higher risk of a poor virological response [p ≤ .001 (95% CI 1.058–1.105)]. For every base 10 logarithm of initial VL, there was a 49% higher risk of a poor virological response [p ≤ .001 (95% CI 1.195–1.848)]. In the regression analysis adjusted for time in ART, adherence to treatment, initial VL, time between genotyping and change of therapy, and therapeutic regimen, it was found that patients who used the regimen consisting of PI + INI had 69% less risk of a poor virological response [p = .019 (95% CI 0.117–0.825)]. Patients who adhered to the treatment had a 27% lower risk of a poor virological response [p = .101 (95% CI 0.504–1.063)]. For every month of delay between genotyping and change of therapy, there was a 7% higher risk of a poor virological response [p ≤ .001 (95% CI 1.050–1.094)]. For every logarithm of initial VL, there was a 59% higher risk of a poor virological response [p ≤ .001 (95% CI 1.247–2.029)]. The full results of the multivariate analysis are shown in Tables 5 and 6.
Association Between Virological Response and Therapeutic Regimen Prescribed in HIV Patients Who Presented the M184V Mutation in Two National Hospitals During the Years 2008 to 2019
RRc is crude relative risk and RRa is adjusted relative risk with a 95% confidence interval of the categorical variables.
Time in ART, adherence to treatment, initial VL, time between genotyping and change of therapy, and therapeutic regimen.
Association Between Virological Response and Therapeutic Regimen Prescribed in HIV Patients Who Presented the M184V Mutation in Two National Hospitals During the Years 2008 to 2019
RRc is crude relative risk and RRa is adjusted relative risk with a 95% confidence interval of the numerical variables.
Time in ART, adherence to treatment, initial VL, time between genotyping and change of therapy, and therapeutic regimen.
Discussion
Our main finding is that 87% of patients who used PI + INI achieved a good virological response and also had 70% less risk of a poor response, so this regimen would be optimal for this studied population. This result is consistent with that described in a cohort of 550 patients carrying the M184V mutation, in which virological suppression was achieved in 80% of those who used a regimen composed of INI. 13 Also, in the DTG VS LPV/R (DAWNING) study presented at CROI 2019, of 624 subjects randomized, M184V/I mutation was present in 513, 84% of the patients who used INI achieved undetectability compared to 70% of those who used PI + 2 NRTIs as second-line. 14 Wilson et al. recognized that, although their sample was small, 100% of patients on regimens containing two active agents other than NRTIs, such as PI + INI, achieved virological suppression. 15 However, in the Europe-Africa Research Network for Evaluation of Second-line Therapy (EARNEST) randomized controlled trial, despite the fact that 84% of patients in PI + INI achieved a good virological response, it was not statistically significant when compared to PI + 2 NRTIs; perhaps the result was related to the M184V mutation not being present in the entire study population. 16 In different populations, the frequency of prescription of the regimens after a bad virological response is varied. According to the WHO, the preferred regimen is the one composed of PI + 2 NRTIs and only as an alternative with “low quality of evidence” PI + INI can be used, regardless of whether or not the patient presents the M184V mutation. 5 Indeed, the study found that half of the subjects were prescribed the regimen proposed by the WHO and that in only 17% of cases the alternate regimen based on INI was prescribed. These results are similar to those reported in Brazil, where 12% of patients used an INI in the regimen. 17
In our study, patients were predominantly men between 30 and 40 years old, heterosexual and with secondary and higher education. This profile is very similar to that found in a recent study of epidemiological characterization of patients with HIV/AIDS infection and VF in a Peruvian hospital of level III. 12 A risk factor associated with poor virological response was the delay in changing therapy. It was established that for each month of delay, the risk increased by 7%, this is comparable to that reported by Levison et al. who found that for each month of delay, the risk of VF to the second-line increased by 7% (Ref. 18 ). It took 2 months for doctors to choose the new regimen, a result similar to that identified by Matsuda et al. whose average time was 2.2 months. 17 As proposed by Murphy et al., this gap is due to doctors' concern about adherence to a less familiar drug regimen, the toxicity of ARVs, and the protocols that must be followed to change treatment. 19 In Peru, for example, if the INI is intended to be included in the new regimen, the approval of the Committee of Experts on Comprehensive Care of Adults with HIV/AIDS is required. 7 Another risk factor for VF found in this study was the high initial VL. In Brazil, patients with VF to a second-line regimen presented initial VL of 4.98 log10 and a CD4 of 180 cells/mm3, values comparable to those of our study. In this regard, it is known that an initial CD4 count <200 cells/mm3 represents a higher probability of second-line VF and that an initial VL >4 log10 is associated with a poor clinical outcome and disease progression. 20,21
Finally, in countries with limited resources such as Peru, high rates of VF to a second-line therapy are often associated with poor adherence. 22 It is vitally important to characterize patients who are not adherent to ART in whatever regimen they are found. Characteristics such as little or no continuing education on adherence to ART, fatigue from treatment or alcohol consumption, 23 some of them identified in our study, are described as factors associated with poor adherence in Uganda, a developing country.
The retrospective nature of the study and the different exposure times to the second-line regimen are obvious limitations to this study. However, our findings are in line with other studies that show that using an INI in the second-line regimen results in a considerable decrease to the control VL. This premise has an important implication in clinical practice, since it will guide the therapeutic behavior of doctors when they are faced with a patient with the M184V mutation and VF to the first-line regimen.
We recommend immediate change of therapy after identification of the M184V mutation. In addition, accompanied by continuous monitoring that not only evaluates the virological response 6 months after starting the second-line therapy but also at 6 weeks and 3 months to ensure the sustained success of said therapy. In the case of INIs, we consider that it should be established as a free prescription therapy by the attending physician, thus facilitating the initiation of the second-line therapeutic regimen. Finally, it is still vitally important to intervene on each risk factor identified in the patient to avoid the progression of the disease.
Conclusions
In Peru, the group of HIV patients presenting with the M184V mutation are mostly prescribed regimens composed of NRTIs. However, our study identified that the use of a regimen composed of PI + INI has shown a greater decrease in control VL and, therefore, good virological response. In addition, the risk factors associated with a poor virological response, in this population, were the delay between genotyping and the change of therapy, high levels of initial VL, and poor adherence.
Footnotes
Authors' Contributions
R.P. and F.V. from the Escuela de Medicina, Facultad de Ciencias de la Salud, Universidad Peruana de Ciencias Aplicadas, Lima, Peru; A.L. from the Servicio de Infectología, Hospital Nacional Arzobispo Loayza, Lima, Peru. All persons who meet authorship criteria are listed as authors, and all authors certify that they have participated sufficiently in the work to take public responsibility for the content, including participation in the concept, design, analysis, writing, or revision of the article. Furthermore, each author certifies that this material or similar material has not been and will not be submitted to or published in any other publication before its appearance in the AIDS Research and Human Retroviruses.
Acknowledgments
The authors are grateful to study participants from the Arzobispo Loayza National Hospital and the Daniel Alcides Carrión National Hospital involved in the study.
Author Disclosure Statement
The authors declare that there is no conflict of interest regarding the publication of this article.
Funding Information
No funding was received for this research.