
Abstract
Immune activation and inflammation are hallmarks of chronic HIV infection and are etiologically linked to major causes of morbidity and mortality among HIV-infected persons, including coronary artery disease and cancer. Systemic immune activation is dampened, but not resolved, with use of combination antiretroviral therapy (cART). Statins are cardioprotective drugs that also appear to have immunomodulatory and anti-inflammatory properties. We sought to understand the association between statin use, cART, and levels of circulating immune markers in a longitudinal cohort study. From 2004 to 2009, statin use was ascertained in male participants of the Multicenter AIDS Cohort Study (MACS) using interviewer-administered questionnaires. Twenty-four circulating markers of immune activation and inflammation were measured in archived serial samples from a subset of cohort members using multiplex assays. Propensity-adjusted generalized gamma models were used to compare biomarkers' distributions by statin use, and multivariable linear regression models were used to assess the effect of initiating statin on these biomarkers. Overall, 1,031 cART-exposed individuals with HIV infection were included in this study. Statin use was reported by 31.5% of cART-exposed participants. Compared to nonstatin users on cART, statin users on cART had lower levels of IP-10, IL-10, and IL-12p70, and the effect of statin use was decreased in participants using lipophilic statins (atorvastatin, simvastatin, fluvastatin, or lovastatin); these results were statistically significant (p < .05). Among cART users not on aspirin, starting statins decreased levels of high sensitivity c-reactive protein (hsCRP), IL-12p70, and IL-6. Statin therapy is associated with reduced levels of certain biomarkers of immune activation and inflammation in cART users, which may contribute to a lower burden of disease.
Introduction
Statins are cardioprotective drugs used for primary and secondary cardiovascular disease (CVD) risk reduction and are among the most commonly prescribed drugs in the United States They reduce cholesterol production in the liver by inhibiting the conversion of 3-hydroxy-3-methylglutaryl CoA to mevalonate, a rate-limiting step in the cholesterol biosynthesis pathway. 1 In addition to cholesterol synthesis, mevalonate is required for production of several intermediates that are integral to the post-translational modification and activation of several intracellular signaling proteins. Thus, statins have pleiotropic effects, and the mechanism whereby statins reduce mortality and morbidity from CVD may not just be due to their cholesterol-lowering properties, but also because of their immunomodulatory and anti-inflammatory properties. 1,2
Statins appear to also have chemopreventive properties. 3 A growing body of epidemiological literature has shown that statin use is associated with a reduced risk of cancer at diverse sites, 4 –6 including non-Hodgkin lymphoma (NHL) in the general population, 7 –10 and AIDS-related NHL (ARL), 11 which is currently the most common malignancy in HIV-infected persons.
Interestingly, a strong body of literature demonstrates that ARL is preceded several years by elevated levels of serum biomarkers of inflammation and immune activation, 12 –17 suggesting that the immunomodulatory effects of statins in the setting of HIV may have beneficial effects on reducing the burden of ARL, as well as CVD.
Although combination antiretroviral therapy (cART) greatly inhibits HIV replication, and its use has dramatically decreased AIDS-related mortality, 18 many HIV-infected individuals on cART still show some degree of persistent chronic inflammation. 19 –21 Given its immunomodulatory properties, statin therapy may reduce inflammation-related outcomes in HIV-infected individuals on cART. Several prior studies have examined the effects of statins on markers of inflammation and immune activation in people living with HIV on cART; however, results have been variable. Some common limitations of these prior studies include a small sample size, inclusion of a limited number of biomarkers, and examination of a single type of statin usually in the context of a randomized controlled trial. 22 –29
The influence of different statin classes on immune biomarkers in people living with HIV on cART is not very well understood, although some prior studies suggest that lipophilic statins (atorvastatin, simvastatin, fluvastatin, and lovastatin) may have more potent immune effects compared to hydrophilic statins (pravastatin or rosuvastatin), which are less efficient at permeating cell membranes. 30,31 Furthermore, nonsteroidal anti-inflammatory drugs (NSAIDs) are commonly used among those with high CVD risk and may mask statin effects; thus, NSAID use needs to be accounted for in the examination of statin effects on immune markers.
To fill in some of these knowledge gaps, we utilized a well-characterized longitudinal cohort followed semiannually with standardized protocols to investigate the association between statin use and serum levels of cytokines and other molecules associated with inflammation or immune activation in HIV-infected individuals on cART.
Methods
Study population
This study was nested in the Multicenter AIDS Cohort Study (MACS), an ongoing prospective cohort study of the natural and treated history of HIV/AIDS in men who report sex with men, who had a mean age of 32–36 years depending on recruitment cohort. Participants were recruited from four U.S. metropolitan areas (Baltimore/Washington, Chicago, Los Angeles, and Pittsburgh), and study visits have been held at 6-month intervals beginning in 1984 (
The current analysis capitalized on an existing MACS substudy conducted to understand the effects of HIV and HCV infection and cART exposure on biomarkers of inflammation and immune activation. 21,33 –35 Included in the substudy were all MACS participants with known HIV seroconversion dates and cART initiators at the time of analysis. Biomarkers were measured on archived sera obtained over 1-year intervals in men with known HIV seroconversion dates and from visits immediately before and after cART initiation (and at 2-year intervals thereafter) for all cART users. For comparison, biomarkers were measured in a representative sample of 250 HIV-uninfected MACS participants, using archived sera from four visits that spanned the MACS follow-up from 1984 to 2009, including all HIV-uninfected men with HCV infection (N = 35).
Exposure assessment
Current statin use was identified from the 6-month study interviews starting in 2004, when questions about statin use were first included in the study protocol, through 2009, when samples were selected for testing. Using the names of the reported medications, we categorized statin drugs as lipophilic (atorvastatin, lovastatin, simvastatin, and fluvastatin) or hydrophilic (rosuvastatin and pravastatin).
Biomarker assessment
Twenty-four circulating markers of immune activation and inflammation were measured in archived sera. Concentrations of cytokines [interleukin (IL)-1β, IL-2, IL-6, IL-10, IL-12p70, interferon (IFN)-γ, granular-macrophage colony-stimulating factor (GM-CSF), and tumor necrosis factor (TNF)-α] and chemokines (IL-8 or chemokine C-X-C motif ligand (CXCL)8, IP-10/CXCL10, MCP-1/chemokine C-C motif ligand (CCL)2, MIP-1β/CCL4, EOTX/CCL11, MCP-4/CCL13, TARC/CCL17) were assessed using the Human Pro-inflammatory 9-Plex Ultra-Sensitive panel and Human Chemokine 7-Plex Ultra-Sensitive panel on the Meso-Scale Discovery (MSD, Gaithersburg, MD) system. In addition, six soluble receptors (sCD14, sCD27, sgp130, sIL-2Rα, sIL6R, and sTNF-R2, one cytokine (BAFF/BLyS), and one chemokine CXCL13/BLC/BCA1 were measured using Human Biomarker Custom Premix Kit A, a multiplexed Luminex xMAP system (Fluorokine® MAP) assays (R & D Systems, Minneapolis, MN) on a Bio-Plex 200 Luminex instrument (Luminex, Austin, TX) and Bio-Plex software (Bio-Rad, Hercules, CA). To reduce laboratory variability, all longitudinal specimens from an individual were assessed on the same plate. Finally, CRP was measured by Quest Diagnostics using a high-sensitivity immunonephelometric assay.
Potential confounders
Prior observational studies of the effects of statin use have been criticized for potential confounding by indication. To address this potential confounding, we calculated exposure propensity scores as the predicted probability of statin use conditional on the baseline covariates using multivariate logistic regression models. The following covariates were included in the model: age (at biomarker testing visit), race (white, black, other), smoking status (never, former, current), body mass index (BMI), family history of heart attack or myocardial infarction before 55, family history of hyperlipidemia, aspirin use, hypertension (reported hypertension and use of antihypertensive medication), high systolic blood pressure (SBP, SBP ≥140 mmHg), high diastolic blood pressure (DBP, DBP ≥90 mmHg), type 2 diabetes (T2DM = a fasting plasma glucose >126 mL/dL or reported T2DM and use of antidiabetic medication), and history of angina. Lipid profile [total cholesterol, high density lipoprotein (HDL), low density lipoprotein (LDL), and triglyceride] levels were also assessed as confounders. To maintain the temporality between lipid profile as a confounder and statin use, we used the average lipid levels from 1999 to 2001 for individuals enrolled before 2001 and the average from 2001 to 2002 for those enrolled in 2001. These time periods precede the widespread use of statins beginning in 2004. In addition, we adjusted for hepatitis C virus (HCV) infection (having a positive HCV RNA test before the biomarker testing visit). For HIV-1-infected cART users, CD4 cell count and HIV-1 viral load at the visit before the biomarker assessment were used for adjustment.
Covariate balance before and after propensity score weighting was assessed using the standardized mean differences (SMD). SMD of 0.1 and above were defined as a meaningful imbalance. To account for residual confounding, all analyses were further adjusted for covariates with meaningful imbalance.
Statistical analysis
All the analyses were conducted separately for cART users and HIV-uninfected participants. Propensity scores for using statins were derived from logistic regression incorporating the potential confounders defined above. Given the small sample of HIV-uninfected participants, race, smoking, family history of hyperlipidemia, angina, high DBP, and HCV infection were not included in the propensity score model.
We inversed the biomarker levels (1/biomarker level) to treat observations below the limits of detection as right-censored and fitted generalized gamma (GG) models. 36 We selected the GG model because it is a highly flexible distribution that does not impose strong assumptions on the biomarker distributions, and we have described a similar application in prior publications. 21,34,35 This was key because only a few biomarkers exhibited lognormal distributions. GG distributions are defined by 3 parameters: location (β), scale (σ), and shape (κ). For parsimony, only the location (β) parameter was allowed to vary by exposure, while σ and λ were held constant. The model also accommodated repeated measurements per individual allowing us to use all available biomarker values for each analysis. We subsequently converted predicted values back into the original scale.
The estimated probability densities of each biomarker for cART users and HIV-uninfected participants were obtained by statin use. The effects of statins may not be similar across the entire distribution of each marker. Therefore, we calculated relative percentiles (RPs, ratios of each percentile of biomarkers among statin users to the same percentile among nonusers) for the median, 25th and 75th percentiles using the lognormal distribution, a special case of GG family. A RP close to 1 indicates no difference between statin users and nonusers; a RP >1 indicates that statin users have a higher biomarker level versus nonusers at that percentile, and a RP <1 means that the biomarker level for the statin users was lower. All models were adjusted by age and weighted by the estimated propensity scores. For cART users, models were additionally adjusted for CD4 counts at prior visits.
Several subgroup analyses were conducted. First, we examined the subset of cART users who had viral loads less than 50 HIV RNA copies/mL. We also examined the effects of lipophilic statins on biomarker levels, given the prior body of literature suggesting more potent immune effects by these statins compared to hydrophilic statins. 30,31 In addition, we conducted subgroup analyses by aspirin use to evaluate whether aspirin use modified the effect of statins.
Case-crossover analysis of statin initiation to address confounding by indication
Observational studies examining the effects of statins are susceptible to confounding by indication because statins are used by people with high CVD risk who may have abnormal immune activation and inflammation. To address this potential confounding, we conducted an analysis restricted to statin users and examined biomarker levels before and after statin initiation among cART users. The level before initiation was an average of the measurements from the last two statin-free visits; the level after initiation was the average of measurements from the first two visits following statin initiation. We used multivariable linear regression to examine the change in serum biomarker levels (loge) from before to after statin initiation, accounting for clustering within individuals. We adjusted for age and CD4 cell count at the visit before statin initiation and, as a sensitivity analysis, restricted the analyses to cART users with suppressed HIV-1 RNA levels. Finally, we assessed these associations in different strata of aspirin use. All hypothesis tests were conducted with a two-sided alpha of 0.05.
Results
Overall, 1,280 individuals (1,031 cART users and 249 HIV-uninfected participants) contributed 3,646 person-visits over 5.5 years. Statin use was reported by 325 (31.5%) and 46 (18.5%) of the cART users and HIV-uninfected participants, respectively. At their first visit in 2004–2009, 226 cART users and 36 HIV-uninfected participants were on statins.
Table 1 describes selected characteristics of cART users and HIV-uninfected participants at their index visit, which was defined as the first visit at which statin use was reported for statin users, or the last visit seen for statin nonusers. On average, statin users were older compared to nonusers in both groups (cART users and HIV-uninfected participants), and statin users in both groups were more likely to be white. As expected, CD4 count was higher among HIV-uninfected participants; in addition, CD4 count was higher, and HIV load was lower, among statin users compared to nonusers. HCV infection was less prevalent among statin users. In addition, HCV was more than twice as prevalent among HIV-uninfected participants compared to cART users, which was due to oversampling of HCV-infected/HIV-uninfected participants for the parent biomarker substudy on which the current study is based. Among the HIV-uninfected participants, statin users had a higher BMI compared to statin nonusers. Statin users were also less likely to be current smokers and more likely to be former smokers; this difference was more substantial among the HIV-uninfected participants. Family history of CVD (early heart attack and hyperlipidemia) was lower in the HIV-uninfected group compared to cART users. While family history of heart attack was similar from statin users and nonusers, there was a higher prevalence of family history of hyperlipidemia among statin users. Aspirin use was more prevalent among statin users and among HIV-uninfected participants.
Characteristics of Combination Antiretroviral Therapy Users and HIV-Uninfected Participants According to Statin Use
Values at index visit defined as the first report of statin use or last visit seen for statin nonusers.
Values reference cumulative over all study visits.
Lipid profiles at visit 31–36 for the pre 2001 cohort and at visit 37–39 for the 2001 cohort.
As expected, participants who went on to become statin users had higher baseline lipid levels compared to nonusers, in both groups. Less than 7% of all participants had a history of heart disease. Hypertension was higher among statin users and higher among HIV-uninfected participants. History of angina was rare, affecting less than 2% of participants. Diabetes was more than twice as prevalent in statin users and was similar for cART users and HIV-uninfected participants.
From 2004 to 2009, statin users contributed 815 person-visits with biomarker measurements, 764 among CART users and 51 among HIV-uninfected participants. Lipophilic statins were reported at 77.9% (n = 631) of the statin person-visits, 76.8% (n = 583) person-visits among cART users, and 94.1% (n = 48) person-visits among HIV-uninfected participants. The nonstatin users contributed 2,833 person-visits with biomarkers (2,412 for cART users and 421 for HIV-uninfected participants).
As shown in Supplementary Table S1, biomarker levels at the first visit with statin use in 2004–2009 did not differ significantly between prevalent and incident statin users (p-values for Mann–Whitney U test >.05). Supplementary Figure S1 shows the estimated densities of each biomarker according to statin use for cART users and HIV-uninfected participants. Among HIV-uninfected participants, clear differences between statin users and nonusers were observable for most biomarkers. Among HIV-uninfected statin users, nearly all of the biomarker values were more tightly distributed compared to nonusers. In addition, biomarker differences by statin use were pronounced at the upper tail of the distributions where statin users had lower biomarker levels compared to nonusers for BAFF, CXCL13, sCD14, sCD27, sGP130, sIL-2RA, sTNF-R2, IFN-γ, IP-10 and MIP-1β, and TARC. Among cART users, more subtle differences across statin use groups were observed for several biomarkers. For example, biomarker distributions for sCD14 and sGP130 were shifted to the left (toward lower values) for statin users.
Figure 1a and b shows the relative 25th, 50th, and 75th percentiles of the biomarkers for statin users compared to nonusers estimated from the propensity-adjusted GG models. Among cART users (Fig. 1a), the 25th percentile of sCD14 was significantly higher among statin users compared to nonusers (p < .05), although there was no difference by statin use for the 50th and 75th percentiles, suggesting that the statin effect on sCD14 is limited to those with the highest biomarker levels. The 75th percentile values for IP-10 were significantly lower among statin users compared to nonusers. When we restricted the cART users to those with suppressed HIV RNA, there were no appreciable differences in relative proportions for any of the biomarkers (Supplementary Fig. S2). Among HIV-uninfected participants (Fig. 1a), IFN-γ, IL-1β, and IP-10 were significantly lower among statin users compared to nonusers.
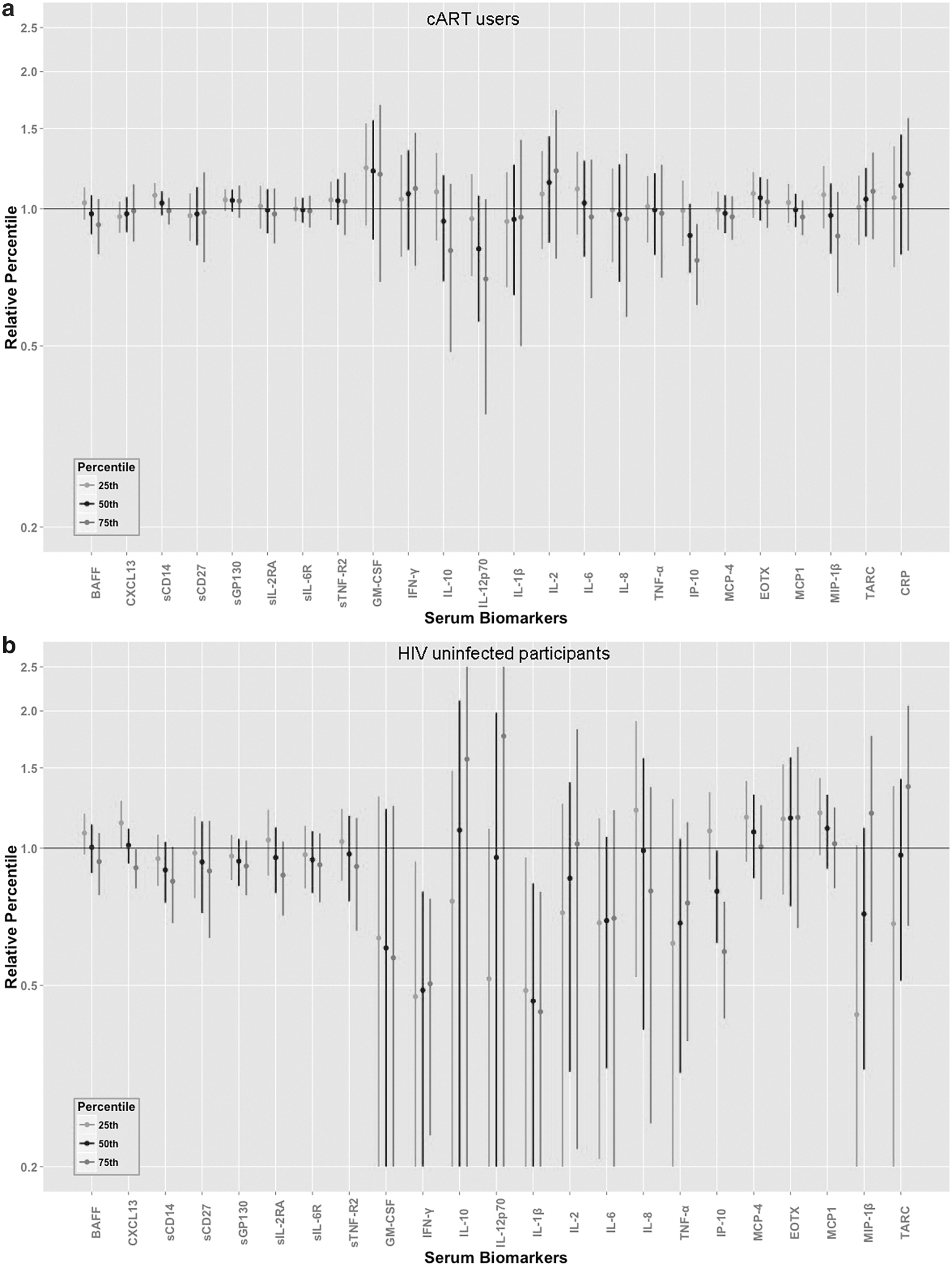
Supplementary Figure S3 shows the estimated RPs for all biomarker values by statin use across the entire distribution of the biomarkers for cART users and HIV-uninfected participants. Notably, for IP-10, the RP distributions were similar for cART users and HIV-uninfected participants, and biomarker levels just above the median percentile and greater were significantly lower for statin users compared to nonusers for both groups alike.
When we looked specifically at lipophilic statin use, the results were similar to overall statin use for HIV-uninfected participants (Supplementary Fig. S4). Among cART users, we observed that in addition to the decreased values of IP-10, IL-10 and IL-12p70 levels were also significantly decreased among statin users compared to nonusers of lipophilic statins (Supplementary Fig. S5).
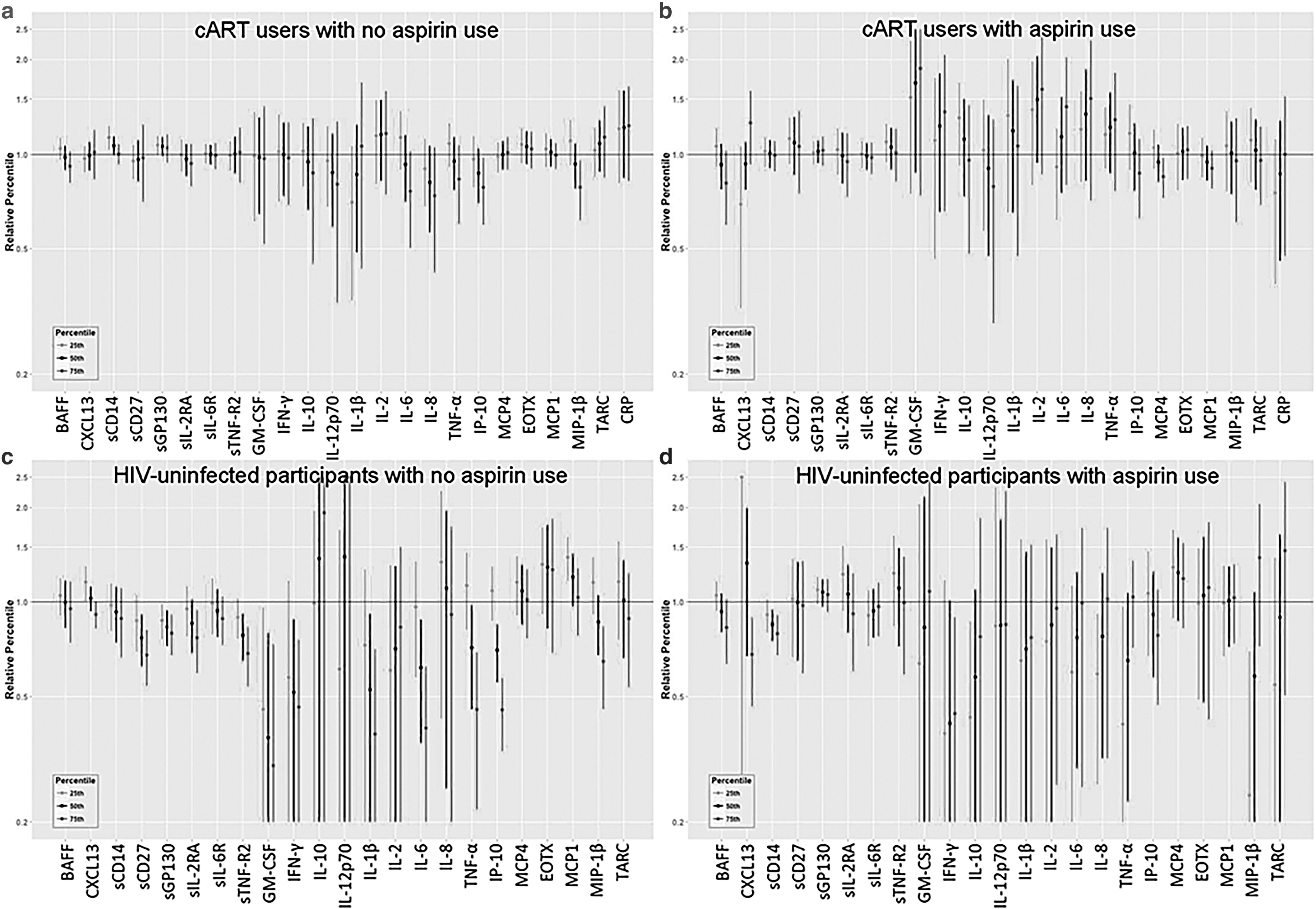
Among cART users not on aspirin, statin use was associated with higher levels of sCD14 at the 25th percentile and lower 75th percentile levels of IP-10 and MIP-1β compared to those not on statins (Fig. 2). Among cART users reporting aspirin use, statin use was associated only with decreased MCP-4 levels at the high end of the distribution. However, for comparison, among HIV-uninfected participants, there appeared to be greater decrease in biomarker levels related to statin use among those who were not users of aspirin. Among HIV-uninfected participants not using aspirin, statin use was associated with decreased levels of sgp-130, GM-CSF, sCD27, sTNF-R2, IFN-γ, IL-1β, IL-6, TNF-α, IP-10, CXCL13, and MIP-1β. Among aspirin-using HIV-uninfected participants, only IFN-γ, CXCL13, sCD14, IL-10, IL-8, TNF-α, and MIP-1β were significantly decreased with statin use.
Relative 25th, 50th, and 75th percentiles comparing statin users to nonusers among
For the case-crossover analysis, we included 83 cART users who initiated statin use between 2004 and 2009. Significant decreases in IL-12p70 and hsCRP levels were observed following the initiation of statins (Fig. 3). The significant effects of statin initiation on IL-12p70 and hsCRP levels were observed only among those without aspirin consumption (Fig. 4). In this group with no aspirin use, starting statins also significantly reduced serum IL-6 levels. Starting statins had no significant effects on serum biomarkers in aspirin users (Fig. 4).
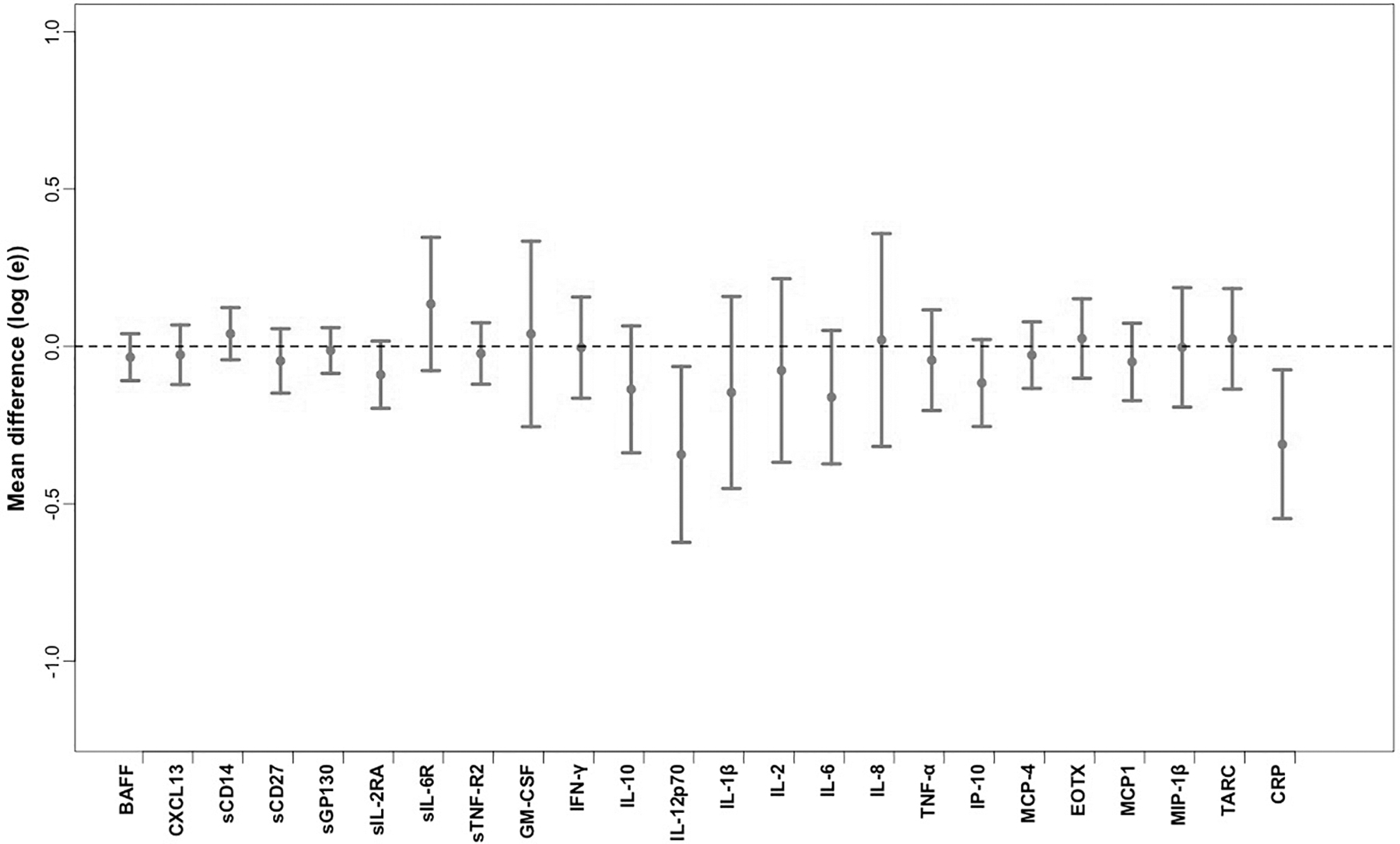
Average mean difference in biomarker levels associated with statin initiation among cART users. The lines represent the 95% confidence limits.

Mean difference in serum biomarker levels associated with statin initiation among cART users by categories of aspirin use. Left line = aspirin users, right line = aspirin nonusers. The lines represent the 95% confidence limits.
Discussion
In the current era of widespread cART usage, excess immune activation and inflammation remain a concern due to their associated risks of morbidity and mortality from CVD, cancer, and other immune-associated conditions. Within the context of a well-characterized longitudinal cohort study that included cART-exposed and HIV-uninfected participants for comparison, we addressed whether statin use is associated with 18 biomarker markers of inflammation and immune activation measured in 3,648 specimen visits. We found that among cART users, statins were associated with a significant decrease in key markers of immune activation, including interferon gamma-induced protein 10 (IP-10). In addition to IP-10, IL-12p70 and IL-10 were decreased among lipophilic statin users, suggesting that there may be a class effect for heightened immune modulation by lipophilic statins. In addition, we observed more prominent statin effects at the higher ends of the biomarker distributions, suggesting that statins may offer protection from the effects of severe inflammation and immune activation.
Our finding that IP-10 was reduced in association with statin use among cART users is supported by some, but not all, prior research. In the SATURN-HIV trial, cART-treated participants randomized to daily rosuvastatin (N = 72) had significantly reduced IP-10 levels compared to the placebo (N = 75) control group. 22 However, among the 303 participants of the AIDS Clinical Trials Group (ACTG) study A5321 who were on long-term cART and maintained suppression for 3 years, higher plasma levels of IP-10 were observed among participants receiving statins. 29 The exclusion of participants who did not achieve long-term suppression in this study may explain their paradoxical finding. Interestingly, we also observed reduced IP-10 in association with statin use in our comparison group of HIV-uninfected MACS participants. IP-10 is an important biomarker of HIV disease 13,37,38 ; thus, more research is needed to clarify the association with statin use in HIV.
HsCRP was reduced immediately following statin initiation in the case-crossover analysis, which controlled for potential confounding due to indication. This observation is supported by some, but not all, prior studies. For example, hsCRP was reduced among statin users initiating antiretroviral therapy 48 weeks after treatment initiation in one study. 23 However, in another study of HIV-suppressed cART users, atorvastatin was not associated with hsCRP levels. 24 In addition, the ACTG 5086 trial of 74 cART users with hyperlipidemia randomized to pravastatin, fenofibrate, or both did not find an association between pravastatin and hsCRP. 25 Some of the variability in these findings may be a result of differences in study design, control for confounding, as well as the type of statin under investigation. Our study population includes a large proportion of persons treated with simvastatin, which is a highly lipophilic statin. For comparison, among HIV-uninfected controls, statin use had a more pronounced inhibitory effect on markers of inflammation and immune activation. This is consistent with prior observational data from other populations that have provided ample evidence that statins can play an immune-modulatory role. 39
Aspirin, like statins, is used for prevention of cardiovascular related morbidity and mortality and is suspected of having immune-modulatory effects in HIV. However studies have shown that aspirin does not appear to have a significant benefit on immune activity for HIV-infected patients on cART. 40,41 When we honed-in on the effect of statins among those who were not aspirin users, several biomarkers were reduced among statin users. Although these stratified analyses were underpowered, it does suggest that statins have an independent effect on immune biomarkers from that of aspirin.
Importantly, most of the biomarkers of immune activation and inflammation that we have examined were not significantly influenced by statin use, supporting the results from several prior studies. 22 –29 However, it is important to note that the biomarkers that were associated with statin use in this study (e.g., IP-10, hsCRP, and IL-6) are important markers of HIV treatment and progression. 21
In this observational study, statin use was determined by self-report, which may have caused some exposure misclassification. However, potential limitations of recall may have been minimized due to the assessment of medication status prospectively every 6 months. Unfortunately, statin dosage was unavailable and therefore could not be evaluated for influence on biomarker levels. In addition, we did not assess favorability of the pharmacokinetic profile for each combination of statins and ART drugs, although it is possible that clinically significant interactions may exist that influence immune biomarker levels. 42 A unique feature of the MACS is the HIV-uninfected participants recruited from the same source population providing an important comparison group. However, for this particular substudy, oversampling of HCV-infected participants may obscure the findings of the HIV-uninfected comparison group. Furthermore, while the case-crossover analysis enabled an assessment of the immediate effect of statins on biomarker levels, with control for confounding by indication, it was limited in statistical power. A post hoc power analysis shows that we had 80% power to detect a mean change in biomarker levels of 0.44 (assuming within person standard deviation of 1), which is a higher mean change than was observed for the majority of biomarkers examined. Finally, we may have increased our susceptibility for false positives due to the number of biomarkers and subgroup analyses performed.
The strengths of this study include the longitudinal assessment of biomarker levels (1,280 individuals contributing 3,646 person-visits over 5.5 years) and the large panel of biomarkers assessed. In addition, we evaluated and directly compared the effect of statin use in cART users and HIV-uninfected individuals from the same underlying population followed with the same standardized study protocols. The strength of our analytic approach allowed examination of the effects of statin use across the entire spread of all of the biomarkers' distributions and not just on the median or mean levels, which allowed us to identify that the statin effects can be primarily observed among those with levels at the upper end of the distribution.
Conclusion
In conclusion, statin use was associated with a dampening of inflammation, suggesting that statin therapy may help reduce the risk of inflammation-related outcomes among cART users. The lower magnitude of the effect when comparing cART users to the HIV uninfected suggests that the pleiotropic effects of statins observed in the general population may not fully translate to the HIV-infected population on cART; this suggests that more investigation is needed to elucidate the underlying mechanisms associated with the anti-inflammatory and immune-modulating properties of statins in HIV infection.
Footnotes
Acknowledgments
The authors thank the MACS participants, without whom this and many other studies would not have been possible. Data in this article were collected by the Multicenter AIDS Cohort Study (MACS), now the MACS/WIHS Combined Cohort Study (MWCCS).
Authors' Contribution
Conception and design: S.K.H., A.G., O.M.-M., and L.P.J. Acquisition of data: O.M.-M. and L.P.J. Analysis and interpretation of data: S.K.H., A.G., O.M.-M., and L.P.J. Writing, review, and/or revision of the article: all authors. Study supervision: L.P.J.
Author Disclosure Statement
No competing financial interests exist.
Funding Information
The contents of this publication are solely the responsibility of the authors and do not represent the official views of the National Institutes of Health (NIH). MWCCS (Principal Investigators): Baltimore CRS (Todd Brown and Joseph Margolick), U01-HL146201; Data Analysis and Coordination Center (Gypsyamber D'Souza, Stephen Gange and Elizabeth Golub), U01-HL146193; Chicago-Northwestern CRS (Steven Wolinsky), U01-HL146240; Los Angeles CRS (Roger Detels), U01-HL146333; Pittsburgh CRS (Jeremy Martinson and Charles Rinaldo), U01-HL146208. The MWCCS is funded primarily by the National Heart, Lung, and Blood Institute (NHLBI), with additional cofunding from the Eunice Kennedy Shriver National Institute Of Child Health & Human Development (NICHD), National Institute On Aging (NIA), National Institute Of Dental & Craniofacial Research (NIDCR), National Institute Of Allergy And Infectious Diseases (NIAID), National Institute Of Neurological Disorders And Stroke (NINDS), National Institute Of Mental Health (NIMH), National Institute On Drug Abuse (NIDA), National Institute Of Nursing Research (NINR), National Cancer Institute (NCI), National Institute on Alcohol Abuse and Alcoholism (NIAAA), National Institute on Deafness and Other Communication Disorders (NIDCD), National Institute of Diabetes and Digestive and Kidney Diseases (NIDDK), National Institute on Minority Health and Health Disparities (NIMHD), and in coordination and alignment with the research priorities of the National Institutes of Health, Office of AIDS Research (OAR). MWCCS data collection is also supported by UL1-TR000004 (UCSF CTSA), P30-AI-050409 (Atlanta CFAR), P30-AI-050410 (UNC CFAR), and P30-AI-027767 (UAB CFAR). Additional support for this work was obtained from the UCLA AIDS Institute, the UCLA Center for AIDS Research (CFAR; AI28697), and the UCLA Jonsson Comprehensive Cancer Center (JCCC; CA016042) and from R01-CA168482 to R21-CA200420.
Supplementary Material
Supplementary Figure S1
Supplementary Figure S2
Supplementary Figure S3
Supplementary Figure S4
Supplementary Figure S5
Supplementary Table S1
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.