
Abstract

A 33-year-old woman with a history of HIV infection presented to the infectious disease clinic to establish care. She had a history of Pneumocystis jirovecii pneumonia but had been lost to follow-up and never initiated antiretroviral therapy. She eventually presented to her primary care provider with complaints of malaise and abdominal pain. Laboratory testing at this time revealed a CD4 count of 4/μL and an HIV viral load of 3.1 million copies/mL. An abdominal and pelvic computed tomography (CT) scan was performed and showed retroperitoneal and mesenteric lymphadenopathy.
She was referred to oncology for evaluation for lymphoma. At this visit, she reported new onset night sweats with a nearly 25-kg weight loss. Positron emission tomography/CT demonstrated metabolically active and pathologically enlarged lymph nodes in numerous regions, including in the left lower neck, bilateral hilum, para-aortic, retrocrural, retroperitoneal, periportal, and mesenteric zones, which was highly concerning for lymphoma. A laparoscopic mesenteric lymph node biopsy was performed. Touch preparation and histological analysis performed on a lymph node sample revealed findings consistent with the final diagnosis (Fig. 1A). After the biopsy results, blood and lymph node cultures both grew Mycobacterium avium complex.
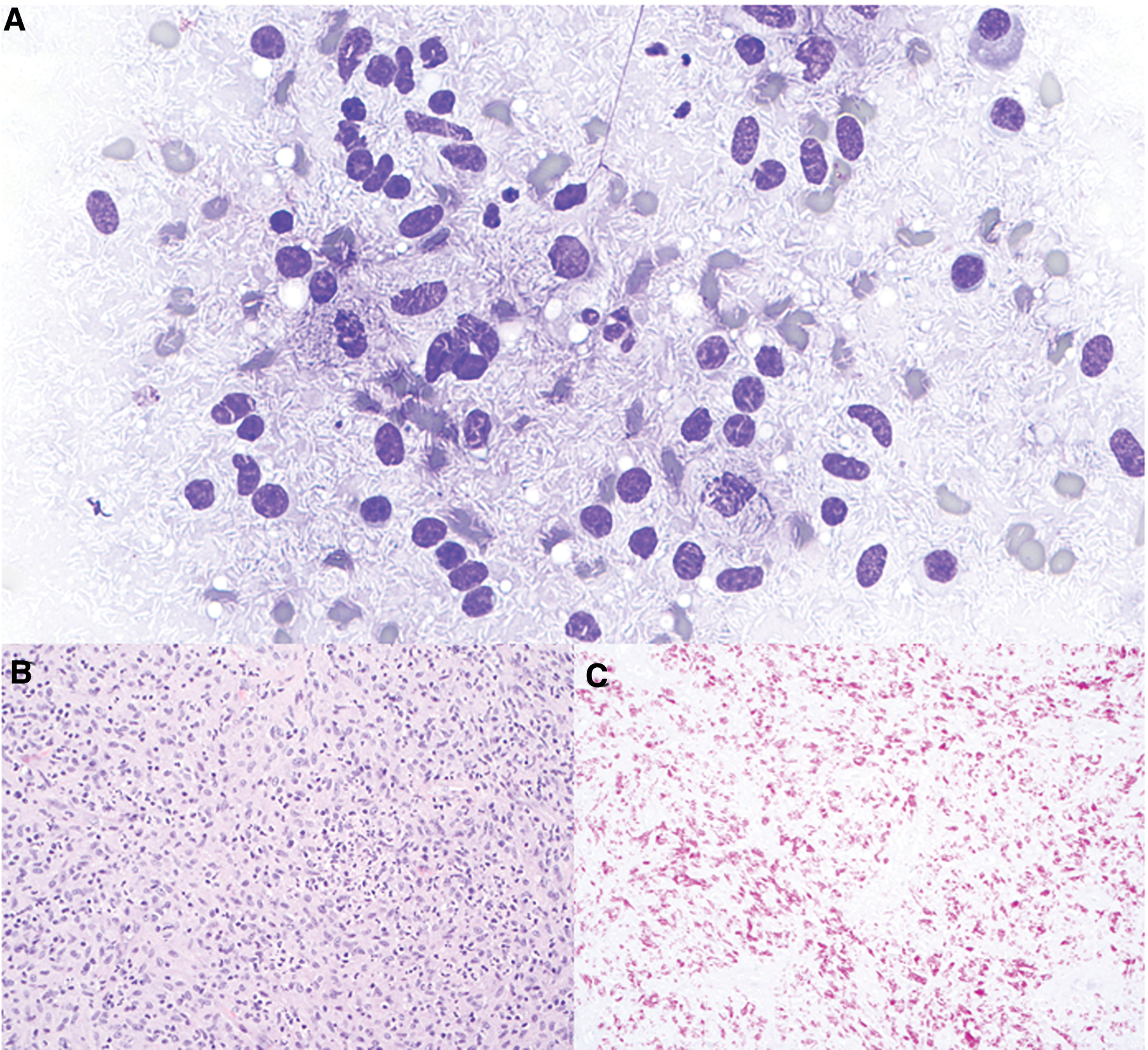
In this case, the patient's initial touch preparation work-up performed on a mesocolonic lymph node revealed the negative outline of innumerable small elongated organisms as seen in Figure 1A. Further histological analysis showed non-necrotizing granulomas (Fig. 1B) and acid-fast bacilli special stains highlighted extensive involvement of the nodal tissue by acid-fast bacilli (Fig. 1C). This work-up supported a diagnosis of an acid-fast bacillus-associated infection, most likely M. avium complex (MAC). Blood and peritoneal cultures grew an organism identified as MAC through DNA probe.
The touch preparation procedure was the key to making the diagnosis. Touch preparation is an important technique in cytopathology for intraoperative evaluation and for guiding specimen triage in the pathology laboratory. 1 In this case, the remarkable display of countless organisms within the lymph node tissue immediately propelled the diagnosis toward mycobacterial infection and away from a diagnosis of lymphoma, allowing for further diagnostic work-up for the infection.
The Mycobacterium genus consists of bacteria that are grouped together on the basis of three characteristics: acid-fastness, mycolic acids in the cell wall, and high guanine+cytosine content in their DNA. These bacteria are nonmotile nonspore-forming bacilli that can be either slow or rapid growers. As of 2015, 170 different species of Mycobacterium have been isolated in humans. 2 Although many of these organisms can cause human disease, the most common are M. tuberculosis, M. leprae, M. avium complex, M. kansasii, M. fortuitum, M. chelonae, and M. abscessus. Mycobacteria are transmitted either through inhalation of aerosols or ingestion. This group of bacteria pose a particularly significant threat in counties with limited access to medical resources. 3
In immunocompetent patients, the most common disease presentation is a progressive indolent pulmonary infection. These usually occur in patients with underlying lung disease or chronic cough suppression. Immunocompromised hosts (e.g., HIV/AIDS, transplant, and hematologic malignancies) typically develop disseminated disease with hundreds to thousands of bacteria per milliliter of blood. 2 Common symptoms include persistent high-grade fevers, night sweats, weight loss, anorexia, fatigue, and cramping abdominal pain; diffuse lymphadenopathy in the chest and abdomen are commonly found on imaging. 4
The patient began an 18-month course of antimycobacterial multidrug therapy shortly after confirmation of diagnosis. At the time of this writing, the patient's symptoms have resolved, and she is doing well on therapy.
Footnotes
Authors' Contributions
N.H. and M.K. prepared and analyzed the photomicrographs; P.B. and D.J.R. provided clinical care and acquired the clinical data; N.H. and P.B. drafted the article; M.K. and D.J.R. provided critical input and revised the article; all authors gave final approval for submission.
Author Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was received for this article.