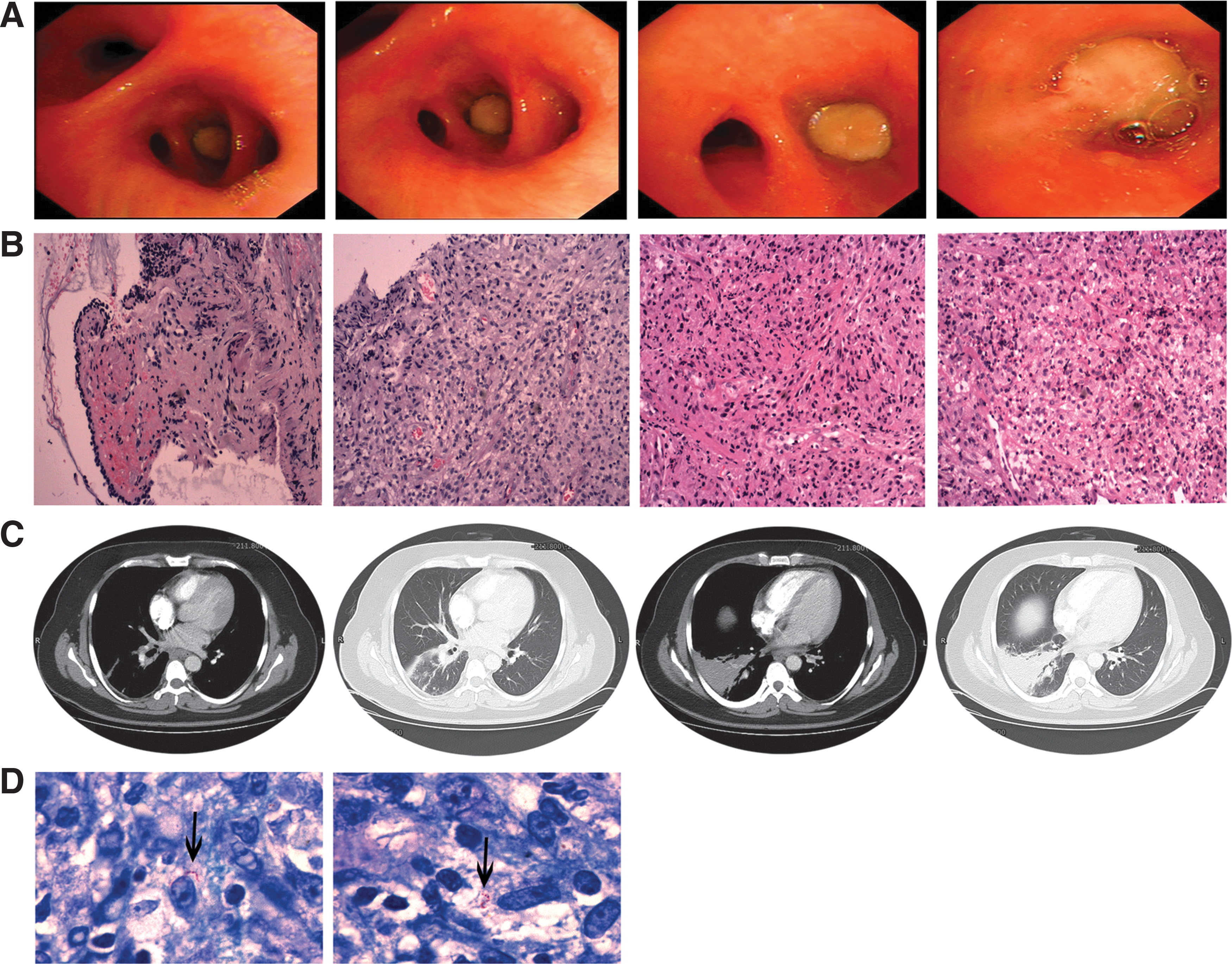
A 29-year-old male with a 5-year history of human immunodeficiency virus (HIV) infection and fatty liver presented with high fever, cough, hemoptysis, palpitations, and chest tightness for 3 weeks. CD4 count was 6.06 cells/μL and moxifloxacin was initially used for suspected community acquired pneumonia (CAP). Repeat bronchoscopies showed a mass in the right basal bronchus (Fig. 1A). Histopathologic examinations showed chronic inflammation with fibrous exudation and granulation tissue hyperplasia (Fig. 1B). Contrast-enhanced computed tomography (CT) imaging showed patchy consolidation in the lower lobe of right lung (Fig. 1C). However, no positive evidence was found in twice bronchoscopy lavage fluid. Inflammatory myofibroblastoma was highly suspected. Thus, we changed the therapy regimen to an antiretroviral therapy of tenofovir, dovegravir, and lamivudine on the 19th day. The patient's condition was stable and was discharged. After 3 months, Mycobacterium kansasii was finally detected in bronchoscopy lavage fluid culture, and positive acid-fast bacilli staining was observed (Fig. 1D). Isoniazid, rifabutin, ethambutol, and moxifloxacin were given in the therapy regimen. The patient was in good condition during the 5-month follow-up. AIDS patients with invasive endobronchial M. kansasii infection are extremely rare, and very limited studies were reported.1–3 In this study, we report an unusual HIV-infected case of M. kansasii infection presenting as an invasive endobronchial occupancy.
(A) Bronchoscopic view shows a mass in the right basal bronchus. (B) Biopsy of bronchial mucosa shows chronic inflammation with ulceration and granulation tissue formation (H&E stain, × 100). (C) Contrast-enhanced CT scan of the chest shows bronchial stenosis and occlusion in the lower lobe of the right lung and multiple lymph nodes in the mediastinum. (D) Acid-fast bacilli staining of bronchoscopy biopsy tissue shows positive results (black arrows). CT, computed tomography; H&E, hemotoxylin and eosin. Color images are available online.
Ethics Approval and Consent to Participate
The study was conducted in accordance with the principles of the Declaration of Helsinki and Good Clinical Practice guidelines. The study was approved by the ethics committee of Tianjin Haihe Hospital. A verbal consent has been obtained from the participant, who has approved the publication of the article with anonymity.
Availability of Data and Materials
All data generated or analyzed during this study are included in this article. The data sets used and/or analyzed during this study are available from the corresponding author on reasonable request.
Footnotes
Authors' Contributions
Y.G. provided input into the concept and design of the study. Y.G. and D.B. collected and assembled the data. Y.G. and C.W. wrote the article. Y.G. and Y.L. critically revised the article. All authors have read and approved the final version at the time of submission.
Author Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was received for this article.
References
1.
ConnollyMG, BaughmanRP, DohnMN: Mycobacterium kansasii Presenting as an endobronchial lesion[J]. Am Rev Respir Dis, 1993; 148:1405–1407.
2.
KimMS, HanJW, JinSS, et al.: A case of Mycobacterium kansasii pulmonary disease presenting as endobronchial lesions in HIV-infected patient. Tuberc Respir Dis (Seoul), 2013; 75:157–160.
3.
OhJY, MinKH, LeeSY, ShimJJ, LeeJ, KimWJ.: Invasive endobronchial Mycobacterium kansasii infection. Am J Respir Crit Care Med, 2019; 200:e143–e144.