
Abstract
A lack of studies analyze risk factors associated with surgical site infection (SSI) in human immunodeficiency virus (HIV)-positive patients with trauma undergoing orthopedic surgery. We questioned, (1) “What is the proportion of SSI in HIV-positive patients receiving open reduction and internal fixation (ORIF) of traumatic limb fractures?” and (2) ”What are the independent risk factors for SSI of HIV-positive patients with traumatic limb fractures who received ORIF?” A retrospective study was performed in our institution from May 2011 to December 2019. A total of 246 patients were enrolled. Data of HIV-positive adult patients with traumatic limb fractures treated by ORIF were extracted from the electronic medical records, including the demographic information, characteristics of fractures, treatment-related variables, and indexes of laboratory examination. Multivariable logistic regression was used to identify independent predictors of SSI. A total of 26 patients developed SSI in this study, the overall proportion was 10.6% [95% confidence interval (CI) = 7.2%–15.3%]. Among them, 18 cases (7.3%) suffered from superficial SSI and 8 cases (3.3%) had the deep SSI. Independent predictors of SSI identified by multivariable logistic regression analysis were CD4+ T-lymphocyte count (adjusted odds ratio per 100/μL increase = 0.55; 95% CI = 0.37–0.81; p = .002) and albumin (adjusted odds ratio per 5 g/liter increase = 0.50; 95% CI = 0.30–0.81; p = .003). We recommend that orthopedic surgeons assess immunosuppression and nutritional status of HIV-positive patients rigorously and optimize the perioperative strategy of supplementary to reduce the risk of SSI.
Introduction
There were 37.9 million people living with human immunodeficiency virus (HIV) in the world by the end of 2018. 1 With the development of antiretroviral therapy (ART), HIV infection has become a chronic and manageable disease. 2 HIV mainly impairs a patient's immune system by reducing the CD4+ T-lymphocyte count, thereby increasing the risk of opportunistic infection. Previous studies showed the high infection rate of HIV patients after surgery for fractures occurred in developing countries, since the patients suffered more open fractures and unfortunately had no chances to receive the ART. 3 However, with the wide application of ART, there have been a number of well-designed studies with appropriate course of follow-up to evaluate early infection in surgery for fractures, demonstrating no increased risk of infection in HIV-positive patients with closed fractures. Nevertheless, limited evidences for the open injuries require a deeper understanding. 4
Surgical site infection (SSI) is one of the most reported hospital-acquired infections, which is associated with increased morbidity and mortality. In addition, SSI constitutes a financial burden and negatively impact on patients' quality of life. 5 The use of implants in orthopedic surgery is associated with an increased risk of infection after surgery due to foreign body implanted. 6 The patients with infected implants have to receive antibiotics for a long period or even implants will be removed or replaced resulting in a high morbidity and cost. 7
Although available data have compared the rate of SSI after fracture surgeries between HIV- positive and -negative patients in the post-ART era, 8 the risk factors of SSI among peoples living with HIV (PLWH) after open reduction internal fixation (ORIF) for traumatic limb fracture are less well characterized, based on the existing studies yielding conflicting results. 9
Given that, in the current study, we quantify the proportion of SSI in HIV-positive patients receiving ORIF of traumatic limb fractures. Furtherly we identify the independent risk factors for SSI. This study provides comprehensive refers for the following operation strategies.
Methods
Study design
This study was approved by the Ethics Committee of Beijing Ditan Hospital, Capital Medical University. A retrospective single-center cohort study was performed between May 2011 and December 2019 in our institution. HIV-positive patients treated with ORIF for an extremity fracture were enrolled in our study and the postoperative follow-up data ranged from 3 to 12 months.
The exclusion criteria contained patients younger than 18 years old, patients without complete follow-up data, multiple fractures, per prosthetic, pathological, or old fractures (>21 days from initial injury), and treated without open reduction internal fixation and preexisting infection requiring treatment.
Definitions and data collection
All data were extracted from the electronic medical record. Demographic information of patients including age, gender, occupation, body mass index, illicit drugs use, smoking status, comorbidities, and previous operation for any other diseases were inquired and recorded. Surgery related characteristics such as location of surgical site (upper limb or lower limb), injury mechanism (high-energy fractures or not), injury type (close or open), operation season (summer or not), surgery type (emergent or elective), surgeon level (residents, attending, associate chief or chief), preoperative station, anesthetic type (general or not), American Society of Anesthesiologists (ASA) physical status index, operative time, intraoperative blood loss (mL), intraoperative and postoperative usage of antibiotics (antibiotics given within 30 min before surgery were identified as intraoperative use), and postoperative use of drainage were also extracted. For laboratory indexes within 24 h preoperatively, we reviewed white blood cells, hemoglobin (HGB), blood platelet, albumin (ALB), globulin (GLOB). CD4+ T-lymphocyte count was measured within 7 days preoperatively to evaluate the immune system status of HIV-positive patients and was classified into two levels, including <200/μL and ≥200/μL. Date of HIV diagnosis and highly active antiretroviral therapy (HAART), if the patient had an undetectable viral load before operation, was also recorded.
SSI was identified according to the Center for Disease Control (CDC)/National Healthcare Safety Network (NHSN) as infection occurring within 90 days after the index procedure. Infections of deep soft tissue, muscle or fascia; continuous wound discharge or dehiscence; visible abscess or gangrene that requires surgical debridement and implant exchange or removal were identified as deep SSI. A superficial SSI was diagnosed if it met at least one of the following criteria: only skin or subcutaneous tissue at the wound site associated with infection; oral or intravenous antibiotics treatment for incision problems (redness, swelling, pain), but did not meet the criteria of deep SSI regardless of bacterial culture results.
Demographics, description of study population
Overall 284 HIV-positive patients diagnosed with traumatic limb fractures in our institution were collected. Thirty-four patients were excluded based on our criteria and four patients were lost (2.6%). Then, totally 246 patients with complete data were included in the current cohort (Fig. 1). Among them, 221 (89.8%) cases were male and 25 (10.2%) were female, with a mean age of 40.9 years (standard deviation 12.1 years).
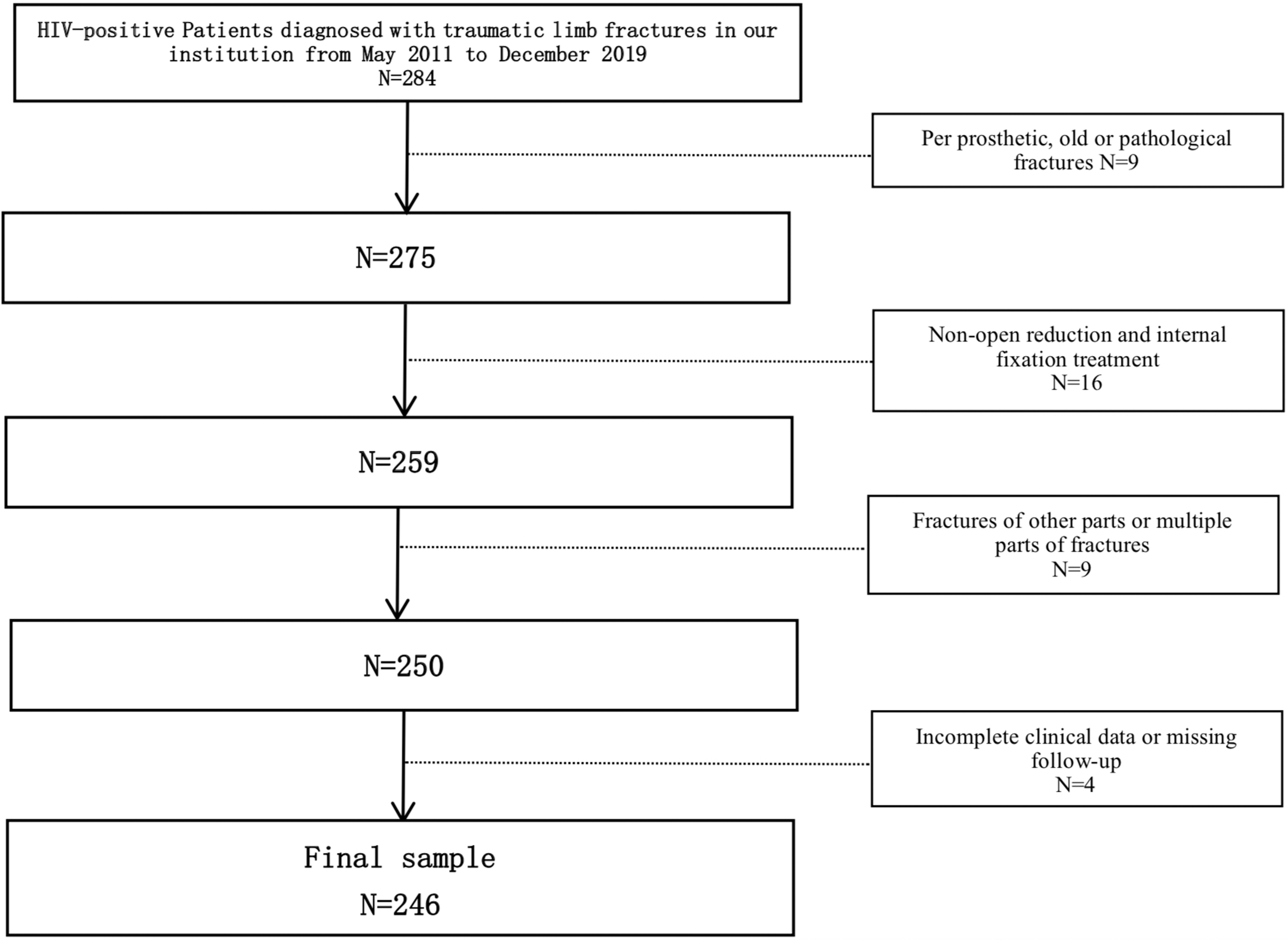
Flowchart showing study enrollment.
Upper extreme fractures were involved in 54 (22.0%) patients and lower extreme fractures in 192 (78.1%) patients. Open fractures were seen in 32 (13.0%) patients, of whom 3 cases with Grade II soft tissue injuries based on Gustilo grading system received external fixator before ORIF. Fractures were caused by high-energy trauma in 126 (51.2%) patients, including 72 (29.3%) cases falling from the height, 48 (19.5%) cases experiencing vehicle collisions, and 6 (2.4%) cases with other reasons.
For 58 (23.6%) cases, HIV infection was discovered because of the fractures, and 188 (76.4%) patients received HAART for at least 3 months before fracture and 184 (74.8%) of them presented undetectable viral load. The CD4+ T-lymphocyte count (within 1 week before surgery) analysis showed that CD4+ T-lymphocyte count <200/μL were observed in 30 (12.2%) patients, 200–499/μL in 147 (59.7%) patients, and ≥500/μL in 69 (28.1%) patients.
A total of 246 cases were finally included and the associated data were analyzed, of whom 26 had postoperative SSI and 220 were uninfected.
Statistical analysis
Data analysis of statistical handling was performed using SPSS 19.0 software (SPSS, Chicago, IL). Mann–Whitney U test was used for nonnormally distributed continuous variables and t test for normally distributed variables. A univariate logistic analysis was used to assess the relationship between each categorical variable and SSI. Only risk factors with a p value <.05 in the univariable analysis were included in the multivariable analyses. Logistic regression with backward stepwise selection was used to choose risk factors for the multivariable model. A significance level of 0.05 was required to allow a risk factor into the model, and a significance level of 0.05 was required for a risk factor to stay in the model. In addition, risk factor selection for the model may be driven by available knowledge and biological plausibility of potential confounders, taking into consideration the hypothesis of interest. The adjusted odds ratio and its 95% confidence interval (CI) were calculated for each risk factor in the presence of others in the final model. The Hosmer-Lemeshow test was used to examine the goodness-of-fit of this model, and the p value >.05 indicated an acceptable fitness. For sample size and power considerations, the prevalence of SSI was assumed as 10%. A logistic regression of SSI on a binary independent variable (X) with a sample size of 214 patients (of which 50% are in the group X = 0 and 50% are in the group X = 1) achieved 80% power at a 0.05 significance level to detect a change in probability of SSI from a value of 0.10–0.25. This difference corresponded to an odds ratio of 3.0. A two-sided Wald test was used.
Results
Proportion of SSI in HIV-positive patients receiving open reduction and internal fixation of traumatic limb fractures
There were 26 (10.6%, 95% CI = 7.2%–15.3%) cases of SSI after open reduction and internal fixation (ORIF) for extremity fractures in HIV-positive patients. Eighteen (7.3%) patients had superficial SSI and 8 (3.3%) developed deep SSI. The bacteriology on the infected group was recorded. Of the 26 infections, 15 (68.2%) bacterial isolates were obtained. Staphylococcus aureus was the most commonly found pathogens, which were successfully cultured in 5 (33.3%, 5/15) patients. Noticeably, one patient's infection was caused by methicillin-resistant S. aureus (Table 1). All eight cases with deep SSIs received irrigation and debridement in combination with intravenous culture-specific antibiotics and internal implant was removed in no cases. Perioperative variables, such as age (39.5 vs. 41.1 years, p = .515), intraoperative blood loss (469 vs. 394 mL, p = .054), and preoperative stay (3.6 vs. 3.9 days, p = .549) are presented in Table 2. There was no significant difference for these variables between the patients with and without SSI. Patients who developed postoperative infection had a significant longer operative time (150 vs. 133 min, p = .004). SSI prolonged a mean of 13.08 days of the hospitalization longer than that of no SSI (32.9 vs. 19.8 days, p < .001) (Table 2).
Bacteriology of the Infected Group
MRSA, methicillin-resistant Staphylococcus aureus.
Continuous Variables Tested in Patients With and Without Surgical Site Infection
Significant variables.
SSI, surgical site infection.
Independent risk factors for SSI of HIV-positive patients with traumatic limb fractures who received ORIF
In the univariate analysis, the parameters, including open fracture, operative time, CD4+ T-lymphocyte count, ALB, and HGB, were investigated to be approximately predictive (p < .05) for SSI. Other factors, such as demographics, comorbidity, laboratory tests, and perioperative factors were not associated with the proportion of SSI. Characters considered as the risk of SSI in univariate analysis are summarized in Table 3. All predictive variables were entered into the multivariate logistic regression model to determine the independent variables. CD4+ T-lymphocyte count (p = .002) and ALB (p = .003) remained statistically significant for the occurrence of SSI. The odds of SSI is reduced by 45% per 100/μL increase in CD4+ T-lymphocyte count (adjusted odds ratio per 100 μL increase = 0.55; 95% CI = 0.37–0.81; p = .002) and by 50% per 5 g/liter increase in albumin (adjusted odds ratio per 5 g/liter increase = 0.50; 95% CI = 0.30–0.81; p = .003). Open fracture, operative time, and HGB were eliminated from the multivariate analysis as independent risk factors (Table 4).
Univariate Analysis of Treatment-Related Predictors for Surgical Site Infection
Significant variables.
ALB, albumin; ASA, American Society of Anesthesiologists; BMI, body mass index; GLOB, globulin; HAART, highly active antiretroviral therapy; HGB, hemoglobin, PLT, blood platelet; WBC, white blood cell.
Multivariable Logistic Regression of Factors Associated with Surgical Site Infection in HIV-Positive Patients Receiving Open Reduction and Internal Fixation for Traumatic Limb Fracture
Significant variables.
CI, confidence interval.
Discussion
ORIF can effectively stabilize traumatic limb fractures and promote the function recovery when conducted safely and effectively. 10 SSIs are one common complication of ORIF for traumatic limb fractures, which occurs a higher frequency in contrast to general orthopedic surgery. 11 However, the risk factors of SSI after ORIF for traumatic limb fractures in PLWH are still less well characterized and further the conflicting data regarding whether reduced CD4+ T-lymphocyte count increases the likelihood of SSI makes many surgeons confused. 3,8,12 –14 Hence, orthopedic surgeons often face difficulties in dealing with traumatic limb fractures of PLWH. Therefore, in this study, we explored the proportion of SSI in HIV-positive patients with traumatic limb fractures who received ORIF, and also discovered the independent risk factors for SSI in this cohort of patients.
Some limitations should be noticed in this single-center study. Essentially, selection bias is possible because of the retrospective nature of this study. Furthermore, severity of comorbidities for each participant is not quantified. In addition, some surgeon-related factors such as surgical incision length, and internal fixation material, which may affect the proportion of SSI, are not included due to the incompleteness of electronic medical records.
The overall proportion of SSI in this study was 10.6% (95% CI = 7.2%–15.3%), which contained 7.3% for superficial SSI and 3.3% for deep SSI. The prevalence of SSI in our study was similar to the results in a recent systematic review, in which 50 (11.6%, 50/432) cases developed postoperative infections. 8 Guild et al. 12 reported 15 (23.4%, 15/64) HIV-positive cases with progressed to SSI after receiving the instrumentation or an implantation orthopedic surgeries, which is higher than the proportion in our study. The potential reasons for that might be the cases with multiple fractures and multiple surgeries were included in Guild et al.'s study. Moreover, the proportion of open fracture in his research (35.9%, 23/64) is much higher than that in our study (13.0%, 32/246), indicating the greater severity of fractures in his study. Bates et al. 14 reported the early wound infection rate (4.2%, 5/118, in closed fractures; 33.3%, 7/21, in open fractures) after internal fixation for trauma in 132 HIV-positive patients. The reason of lower rate of infection in his study may be that wounds were assessed for healing using the ASEPSIS score in his study rather than SSI identified according to CDC/NHSN and the follow-up time was also shorter in his study compared with our current data.
Lower CD4+ T-lymphocyte count and lower ALB were the independent factors associated with SSI of HIV-positive patients with traumatic limb fractures who received ORIF. An important factor in all analyses was CD4+ T-lymphocyte count. HIV can destroy the function of CD4+ T-lymphocytes reducing the number and further suppressing the immune system. 15 It has been well demonstrated that animals depleted of CD4+ T-lymphocyte showed a significant decreased rate of wound healing. 16 However, studies on whether low CD4+ T-lymphocyte count influences the rate of postoperative infectious complications after orthopedic surgery have yielded conflicting results. 12,14 Harrison et al. 17 and Bates et al. 14 found no evidence linking the CD4 T-lymphocyte count with the risk of infection after orthopedic surgery. While Guild et al. 12 and Xu et al. 18 discovered that CD4 count was associated with postoperative infection during orthopedic surgery, in our study, CD4 T-lymphocyte count was definitely considered as the independent factor associated with SSI and the odds of SSI is reduced by 45% per 100/μL increase in CD4+ T-lymphocyte count (adjusted odds ratio per 100/μL increase = 0.55; 95% CI = 0.37–0.81; p = .002) (Table 4).
We therefore advised lower CD4 T-lymphocyte count as a major predictor for SSI after implant surgery. The orthopedic surgeon should fully inform patients with lower CD4 count the higher risk of postoperative infection and some surgery with relative indications should not be performed.
Likewise, in our study, ALB was also definitely considered as the independent factor associated with SSI and the odds of SSI reduced by 50% per 5 g/liter increase in albumin (adjusted odds ratio per 5 g/liter increase = 0.50; 95% CI = 0.30–0.81; p = .003) (Table 4). Albumin level has been identified as one of the most widely recognized and simplest markers for nutritional status. Malnutrition has been proved to be independent predictors of SSI in orthopedic surgery. 19 Yuwen et al. 20 conducted a meta-analysis involved in 112,183 patients from 13 studies demonstrating that the serum albumin level <35 g/liter had an almost 2.5-fold increased risk of SSI in orthopedics, despite many scholars suspected the value of malnutrition (low serum albumin) to predict the SSI in orthopedics among HIV-positive patients. 9,12 To our knowledge, this is the first study to show that low albumin is associated with SSI after ORIF of traumatic limb fractures among PLWH, echoing what is known among HIV-negative individuals. Orthopedic surgeons should pay special attention to the nutritional status when dealing with fractures in HIV patients.
Univariate analysis identified the open fracture, operative time, and HGB as risk factors of SSI. However, these variables were not associated with SSI in the multivariable logistic regression model.
In conclusion, 26 cases (10.6%, 95% CI = 7.2%–15.3%) developed SSI in 246 HIV-positive patients receiving ORIF of traumatic limb fractures, 18 cases (7.3%) were superficial infection, and 8 cases (3.3%) were deep SSI. Lower CD4+ T-lymphocyte count and lower ALB were identified as significant risk factors for SSI. Orthopedic surgeons are recommended to assess nutritional status and immune suppression to understand potential for SSI to develop after ORIF of traumatic limb fractures among PLWH.
Ethical Approval
This retrospective study was approved by the Ethics Committee of Beijing Ditan Hospital, Capital Medical University. All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional and/or National Research Committee and with the Declaration of Helsinki 1964 and its later amendments or comparable ethical standards.
Informed Consent
Informed consent was obtained from all individual participants included in the study.
Data Availability
The datasets generated during and/or analyzed during the current study are available from the corresponding author on reasonable request.
Footnotes
Authors' Contributions
R.Z. and R.D. contributed equally to this work. Patients follow-up by clinical and scientific point of view: R.Z., R.D., and Q.Z. Data collection and analysis: R.Z. Writing: R.D., R.Z., and Q.Z. All authors have read and approved the final article.
Acknowledgments
We thank the patients and all the medical staff involved in this study and thank Hailong Liu for critical review of a draft of this article.
Author Disclosure Statement
The authors declare no conflict of interests.
Funding Information
Capital's Funds for Health Improvement and Research (No. 2018-2-2174), Beijing Municipal Science & Technology Commission (No. Z191100006619060).